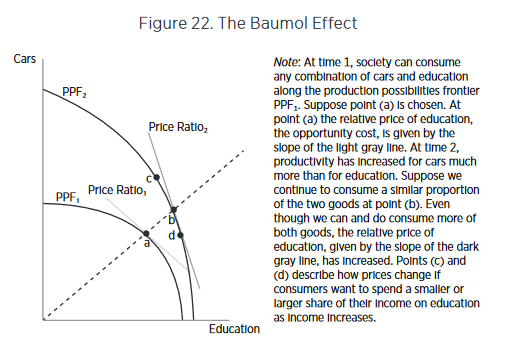
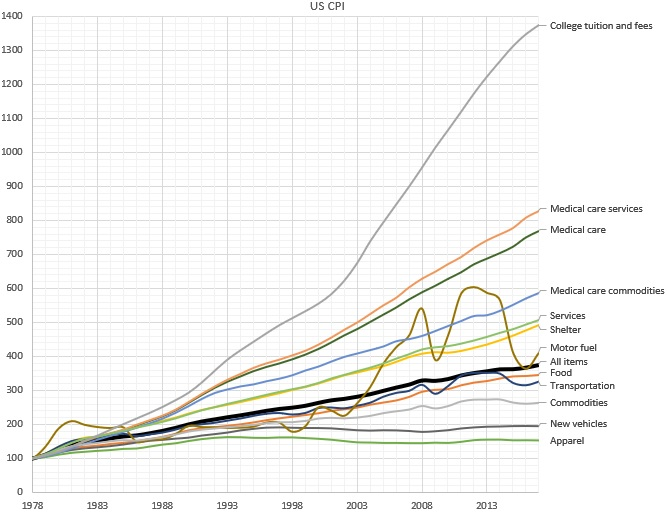
Why does the cost of education and healthcare services continue to rise rapidly, while the cost of goods rise much more slowly? According to economics theory, wages rise when there’s greater productivity; but a rise without an increase in productivity is referred to as “Baumol’s Cost Disease” . In an original study first published in 1966, economist William J. Baumol used the example of a string quartet to illustrate this idea: While the productivity of a given quartet has not increased over time over the last two hundred years, the salary (in nominal and real terms) has increased dramatically.
One way out of this trap is to turn services into goods. Employing a cobbler to make a pair of custom shoes, for instance, is expensive, so we buy factory made shoes: shoes as a good instead of as a service. In doing so, we accept some limitations: a finite set of styles and sizes to choose from; perhaps a less-than-perfect fit for each individual foot; limited styles and customizations — but with the positive trade off in favor of greatly decreased cost. In much the same way, we consume the “good” of the string quartet in the form of a digital recording of a musical piece, instead of the “service” of a live performance. In short, turning services into goods industrializes the process, increasing efficiency and reducing cost.
But is this seemingly alchemical transformation possible in healthcare?
Until today, it’s essentially been accepted as a given that this cost “disease” is incurable where there’s the need for professional, highly trained people performing services — industries like healthcare, education — and therefore drives some of the biggest cost crises of our day, that affect many people in countless ways.
To cure Baumol’s cost disease, we would have to transform the industry’s professional human labor into something that can be manufactured, commoditized, industrialized, and automated. While this has long been an issue in healthcare, for many good and bad reasons, the cure involves bringing more artificial intelligence (AI) to the industry. AI creates a new opportunity: to transform services into goods.
It’s no magic bullet for sure; even our own a16z partners Martin Casado and Matt Bornstein have argued that in enterprise companies, this won’t work, and that AI in this case effectively just replaces human services with different human services with few gains, given all the data cleanup and edge cases involved. But in healthcare, unlike in other industries — like social media content analysis, or self-driving cars — the kind of data labelling needed is actually already an intrinsic part of the healthcare system. In much the same way it is an intrinsic part of Google search — where people choose the most relevant link in the search results, and Google’s AI learns from this, improving with each search — whenever a doctor diagnoses a condition, prescribes a mediation, or interprets an x-ray, that information is then encoded into the electronic health record (EHR). Or, it’s in revenue cycle management — how all bills are paid in healthcare — where people currently perform the manual tasks of identifying what is billable, and to whom. Using AI to learn from these coders (the way, for example, Alpha Health does) means the human work — human labeling — is “free”, since it’s part of what we’re doing anyway.
What’s more, the data is high quality, because when all the doctors in the system are labellers, AI ensures every doctor has the very best teachers in the world — no single doctor alone could ever have that roster of mentors. Training is done on all patients, AI learns from everything, and everybody… and then outputs the results back out to everyone.
AI learns from everything, and everybody… and then outputs the results back out to everyone.
Of course, it’s not a total walk in the park; work needs to be done to integrate this data into the system. One you solve data labelling, you have to train with those labels. Data labelling is just one of the reasons AI based businesses are perceived to have low margins (often requiring an enormous amount of GPU or CPU time, and at great expense. But human training is also expensive: training must often be customized to individuals, and often needs to be redone as employees churn. Because computers are identical, training AI has no such challenges. If you compare the cost of AI training to the cost of executing a simple algorithm, AI training is expensive. If you compare the cost of AI training to the cost of human training, AI is cheap. And, AI training gets exponentially cheaper over time, because of Moore’s Law’s profoundly powerful compounding effects. So even if using AI is at cost parity with a service solution now, the eventual win is obvious. And to some degree, we can commoditize the AI itself as well, for more efficiency, by keeping customization low and training rare with AI.
Another complaint about AI’s ability to transform services into goods is what’s referred to as the “long tail of tasks.” This is the idea that AI won’t be useful if it can only perform a small fraction of what humans can. But in healthcare, even a small fraction of that long tail can have enormous impact. With the right, highly efficient training and labeling, AI can transform perhaps 5% of the human labor of analyzing bills and claims to automate from services to goods. By using AI to learn from medical billing — even just by triaging the “easy” and mundane cases (and escalating the “long tail” of more complex tasks to people as needed) — can bring a dramatic cost savings. Not to mention allowing people to focus on the more higher order aspects of the job, allowing them to deliver better results and service.
We’ve been waiting decades — maybe even centuries — for the ability to reverse Baumol’s Cost Disease in our most service-heavy, yet most critical, industries, such as healthcare.
The transformation of services into goods won’t occur overnight. But Baumol himself couldn’t have foreseen the revolution that AI is creating, any more than someone in the Renaissance anticipating a shoe factory and Moore’s Law since. If applied in the right places, with the right conditions, taking into account the hard realities of the healthcare system, AI can be a vastly powerful lever to pull. We may not cure Baumol’s Cost Disease overnight, but even a small gain in cost and time savings would have huge impacts in healthcare.