This week’s graphic features our assessment of the many emerging competitive challenges to traditional health systems.
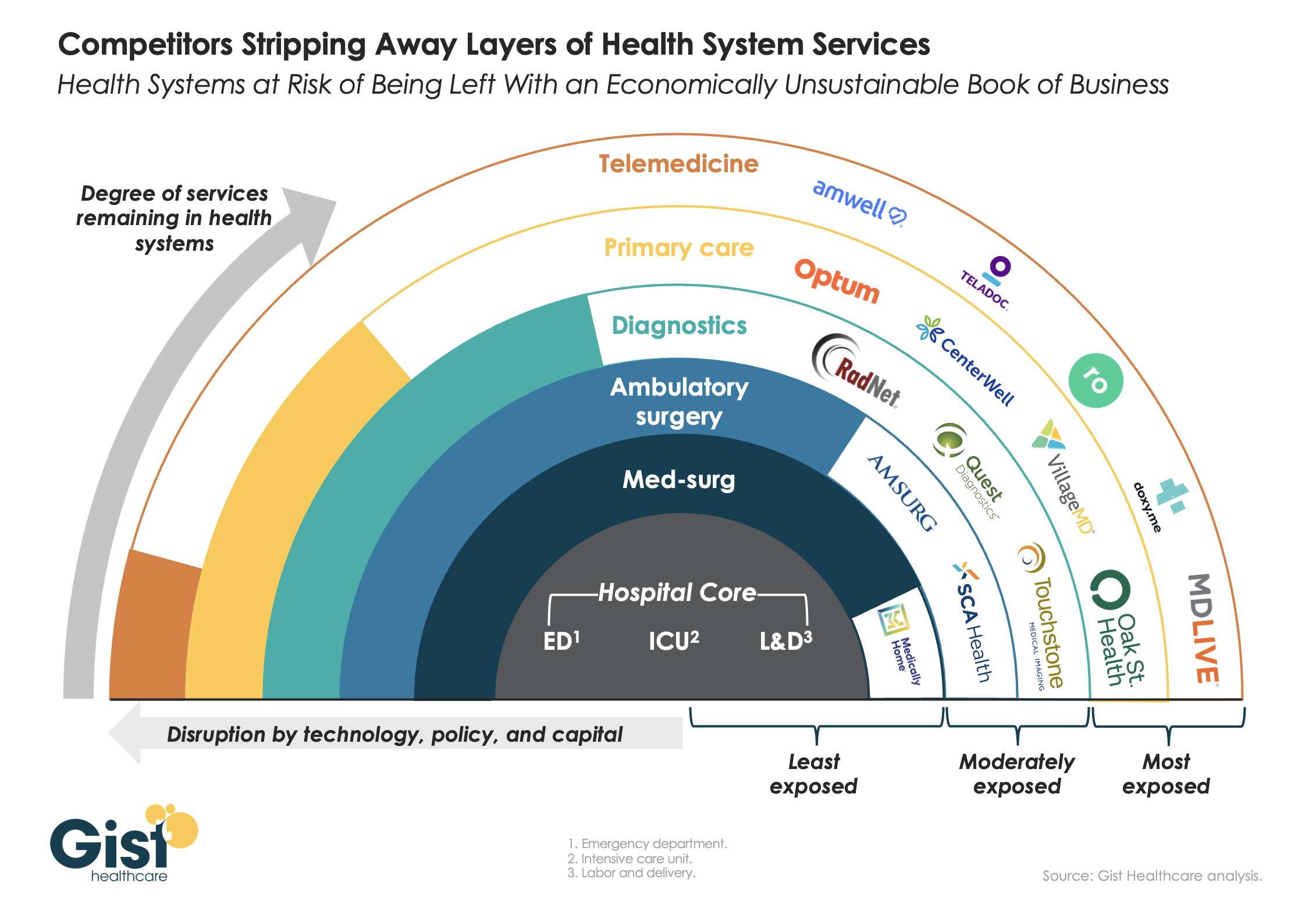
Beyond inflation and high labor costs, health systems are struggling because competitors—ranging from vertically integrated payers to PE-backed physician groups—are effectively stripping away profitable services and moving them to lower-cost care sites. The tandem forces of technological advancement, policy changes, and capital investment have unlocked the ability of disruptors to enter market segments once considered safely within health system control.
While health systems’ most-exposed services, like telemedicine and primary care, were never key revenue sources (although they are key referral drivers), there are now more competitors than ever providing diagnostics and ambulatory surgery, which health systems have relied on to maintain their margins.
Moving forward, traditional systems run the risk of being “crammed down” into a smaller portfolio of (largely unprofitable) services: the emergency department, intensive care unit, and labor and delivery.
Health systems cannot support their operations by solely providing these core services, yet this is the future many will face if they don’temulate the strategies of disruptors by embracing the site-of-care shift, prioritizing high-margin procedures, rethinking care delivery within the hospital, and implementing lower-cost care models that enable them to compete on price.
Across the hospital industry, heavy reliance on contract labor in 2021 and 2022 caused a significant challenge for profitability.
However, a chief financial officer recently posited that his system’s large contract labor load has had unexpected benefits.
“Other hospitals [in our market] thought we were crazy to keep staffing with high contract rates until recently,” he shared. “But by keeping the agency nurses around a little longer, we were able to avert raising base salaries quite as much, and are in a better place today now that the labor market has softened.” It’s a story we’ve heard several times now.
While market rates for nursing and other clinical labor have undoubtedly been rebased, salary increases are sticky—it’s hard to adjust wages downward when the labor market loosens.
Systems who were able to avert large wage increases by increasing bonuses and other non-salary benefits, or forestalled permanent hiring at higher salaries by extending contract labor, now find themselves with more flexibility and potentially lower staffing costs in the long-term.
Labor costs have spun out of control in the last few years as inflation set in and hospitals relied on contracted travel nurses to combat nationwide workforce shortages.
The secret to lowering labor costs now, hospital CEOs say, is putting a modern spin on a tried-and-true strategy: retention.
Dan Woods, CEO of El Camino Health in Mountain View, Calif., estimates the cost of recruiting a single nurse as being nearly $60,000, which drove his team’s decision to focus on reducing labor costs by decreasing turnover. The nurse turnover rate is around 22 percent nationally, but El Camino has achieved just 8 percent nurse turnover rate through a variety of retention efforts.
“We continue to chip away at our turnover rate by fostering a positive practice environment for our nurses,” said Mr. Woods. “We achieve this by creating structures and enabling processes so our staff are engaged in assisting with making changes within their practice environments. Also, our staffing and scheduling processes promote efficiency while meeting the needs of our staff, which is essential for retention.”
El Camino does have guardrails to ensure nurses don’t self-schedule overtime or other premium pay. Mr. Woods also mentioned positive labor relations as a retention tool.
“We just completed a new three-year agreement with our nursing union prior to the existing contract expiring and without strikes or the acrimony often associated with labor relations,” he said.
David Callendar, MD, president and CEO of Memorial Hermann Health System in Houston also recently told Becker’s the system is relying less on contract labor and increasing retention through its Well Together employee experience model, which allows employees to personalize programs and benefits to meet their individual needs.
“At Memorial Hermann, we believe that investing in our workforce is the most effective approach to managing labor costs,” said Dr. Callendar. “We accomplish this in three ways: one, creating a workplace where all feel valued and welcomed, and diversity is celebrated; two, investing in employee health and wellness programs; and three, providing professional development and career growth opportunities.”
Rochester (N.Y.) Regional Health is transforming its operating model and workforce strategy to offer more flexibility and build a culture valuing team members for retention.
“We’ve created a new in-house agency to significantly reduce our reliance on third-party contracts and improve staff integration within the health system to foster a more robust culture of collaboration, interdependency, alignment and system-ness,” said Richard Davis, PhD, CEO Of Rochester Regional.
Jeffrey P. Gold, chancellor of the University of Nebraska Medical Center in Omaha, said the academic medical center is focused on reducing the cost per unit of labor and lowering the number of units. The hospital is considering several tactics including additional training and mentorship, evaluating its benefits program and productivity across the organization.
The University of Nebraska Medical Center is also evaluating fixed labor cost departments and roles, and slowing or eliminating full-time employee growth to force innovation, organizational redesign, use of technology and productivity gains with staff retained.
Many hospitals are seeing wages increase within their markets, and increasing pay for existing team members is often less expensive than recruiting and onboarding new ones.
“Obviously, compensation is a key element of staffing, and we are working diligently to ensure that we are competitive within our market,” said R. Kyle Cramer, CEO of Day Kimball Health in Putnam, Conn. “Concurrently, we are evaluating how we staff our clinical areas and the mix of professionals we utilize to create a stronger level of team support and patient engagement. Ultimately we see stabilizing our workforce and reducing turnover through retaining strong members of our clinical and operational team as the key to effectively managing labor costs in this new era.”
Paula Ellis, DNP, interim CEO of F.W. Huston Medical Center in Winchester, Kan., said the critical access hospital has salaries in line with competitors but found benefits lagging. The hospital increased 401K match, provided better health insurance rates, improved tuition assistance and added competitive scholarships to keep employees engaged. The hospital also combined four positions into two.
“Staff were willing and able to take on new duties in exchange for a better schedule,” said Dr. Ellis. “We believe the best method to manage labor costs is to retain staff.”
An in-depth piece co-published this week in New York Magazine chronicles the Kafkaesque working environment of artificial intelligence (AI) annotators, whose “unprecedented feat[s] of tedious and repetitive behavior” have enabled the AI boom. AI learns by training on massive, meticulously labeled datasets, but that training is not some high-tech, futuristic process.
Instead, AI companies of all kinds have secretively hired a vast, global web of millions of low-wage laborers—mostly in the global south—to annotate these large datasets according to precise, convoluted rules sets (one worker reported marking all the knees and elbows in pictures of crowds for 36 hours straight!). AI optimists predict this phase of labor-intensive annotation will pass once the bots advance to the point of automating the annotating process, but most use cases remain far from this goal. Turns out the AI systems are pretty poor students as well: for example, the models need to be explicitly taught the difference between a shirt, and the reflection of a shirt in a mirror, and a shirt on a hangar, and a shirt on a chair, and on and on.
The Gist: If AI needs to be trained by thousands of low-skilled, low-wage workers to identify an elbow, how many doctors will it take to train the algorithms to accurately diagnose a CT scan as cancerous? Thanks to electronic health records, some of this annotation work has been built into the images, but the sensitivity and high price of patient data make it harder to assemble datasets large enough to power the training.
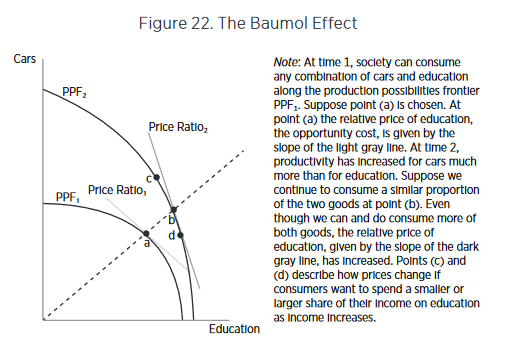
While some remain hopeful that AI has the potential to eventually cure healthcare of Baumol’s cost disease, the path to that point will be paved by significant, tedious manual labor hours performed behind the scenes—adding substantial additional cost and slowing the advent of the long-predicted future of ubiquitous, super-intelligent bots.
Last Thursday, the Senate Finance Committee heard testimony from experts who offered damning testimony about hospital consolidation (excerpts below). Committee Chair Ron Wyden (D-OR) gaveled the session to order with this commentary:
“I’d like to talk about health care costs and quality. Advocates for proposed mergers often say they will bring lower health costs due to increased efficiency. Time after time, it’s simply not proven to be the case. When hospitals merge, prices go up, not down. When insurers merge, premiums go up, not down. And quality of care is not any better with this higher cost. “
Ranking Member Mike Crapo (R-ID) offered a more conciliatory assessment in his opening statement: “In exploring and addressing these problems, we have the opportunity to build on our efforts to improve medication access and affordability by taking a broader look at the health care system through a similarly bipartisan, consensus-based lens…We need to examine the drivers of consolidation, as well as its effects on care quality and costs, both for patients and taxpayers. We also need to develop focused, bipartisan and bicameral solutions that reduce out-of-pocket spending while protecting access to lifesaving services.”
Congress’ concern about consolidation in healthcare is broad-based. Pharmacy benefits managers and health insurers face similar scrutiny. Drug price control referenda have passed in several states and a federal cap was included in the Inflation Reduction Act.
The reality is this: the entire U.S. health system is on trial in the court of public opinion for ‘careless disregard for affordability’. And hospitals are seen as part of the problem justifying consolidation as a defense mechanism.
What followed in this 3-hour hearing was testimony from 3 experts critical of hospital consolidation, a Colorado community hospital CEO who opined to competition with big hospital systems and a Peterson Foundation spokesperson who offered that data access and transparency are necessary to mitigate consolidation’s downside impact.
None of their testimony was surprising. Nor were questions from the 25 members of the committee. It’s a narrative that played out in House Energy and Commerce and Ways and Means Committee hearings last month. It’s likely to continue.
Often, Congressional Hearings on healthcare issues amount to little more than political theatre. In this one, four key themes emerged:
Consolidation among hospitals has adversely impacted quality of care and affordability of healthcare. Prices have gone up without commensurate improvements in quality harming consumers.
Larger organizations use horizontal and vertical integration to strengthen their positions relative to smaller competitors. Physician employment by hospitals is concerning. Rural and safety net hospitals are impaired most.
Anti-trust efforts, price transparency mandates, data sharing and value-based programs have not been as effective as anticipated.
Physicians are victims of consolidation and corporatization in U.S. healthcare. They’re paid less because others are paid more.
While committee members varied widely in the intensity of their animosity toward hospitals, a consensus emerged that the hospital status quo is not working for voters and consumers.
My take:
Consolidation is part of everyday life. Last Tuesday’s bombshell announcement of the merger of the PGA Tour and the Saudi Arabia’s Public Investment Fund caught the golfing world by surprise. Anti-trust issues and monopolistic behaviors are noticed by voters and lawmakers. Hospital consolidation is no exception festering suspicions among lawmakers and voters that the public’s good is ill-served. And studies showing that charity care among not-for-profit hospitals is lower than for-profit confuse and complicate.
As I listened to the hearing, I had questions…
Were all relevant perspectives presented?
Was the information provided by witnesses and cited in Committee member questioning accurate?
Will meaningful action result?
But having testified before Congressional Committees, I find myself dismissive of most hearings which seem heavy on political staging but light on meaningful insight. Many are little more than political theatre. Hospital consolidation seems different. There seems to be growing consensus that it’s harmful to some and costly to all.
Sadly, this hearing is the latest evidence that the good will built by hospital heroics in the pandemic is now forgotten. It’s clear hospital consolidation is an issue that faces strong and increased headwinds with evidence mounting—accurate or not– showing more harm than good.
This week, the Centers for Medicare and Medicaid Services (CMS) finalized a 2018 proposed rule that will impose aggressive audits on Medicare Advantage (MA) insurers. By extrapolating the audits to insurers’ entire contracts, CMS expects to claw back almost $500M annually in overpayments since 2018, but has opted not to extrapolate the audits for 2011 to 2017. While MA insurers threaten to sue over the rule’s exclusion of a “fee-for-service adjustor” that would have reduced the degree of overpayments, CMS officials note that the estimated repayments under the final rule constitute less than 0.2 percent of total MA spending.
The Gist: This MA overpayment audit is overdue, especially given how well-documented MA overbilling has become. This week the Biden administration also announced a proposed change to MA risk adjustment that would reduce MA spending by $11B annually.
Though nearly half of all US seniors are now enrolled in MA plans, the program has yet to achieve its original purpose of saving the government money by encouraging competition around delivering care more efficiently.
MA cannot continue to cost more per enrollee than traditional Medicare in perpetuity, and an eventual reduction in per-member per-year payments is inevitable.
Published last weekend in the New York Times Magazine, this wide-ranging article weaves the experiences of patients and providers within hospital-at-home programs into a broader examination of what hospital-level care at home could mean for the future of healthcare.
While the hospital-at-home movement is still small, provider interest grew sharply during the pandemic, and gave rise to Medicare’s Acute Hospital Care at Home waiver, providing 260 hospitals Medicare payment for the service. The article lays out the challenges hospital-at-home programs are still working to overcome, ranging from equity (rural hospitals have seen far less uptake of the Medicare waiver), labor models (National Nurses United, the largest union of registered nurses, opposes them), to the upfront investments required to stand up a program.
The Gist: Like telemedicine, hospital-at-home programs lingered on the fringes of care delivery before the federal COVID response delivered both the regulatory flexibility and the reimbursement needed to generate provider interest—and turbocharged start-ups providing support in implementing the model.
Despite growth in health system and payer interest, hospital-at-home programs are still not deployed widely, or at scale. Many physicians and patients either don’t understand or accept it as an alternative to inpatient hospitalization, despite the fact that patients and families who participate in the service largely report a high level of satisfaction.
But as the article points out, thebarriers to scaling hospital-at-home pilots—staffing models, quality control, and appropriate reimbursement—are ultimately financial.