https://www.axios.com/2024/04/15/doctors-union-gen-z-millennial
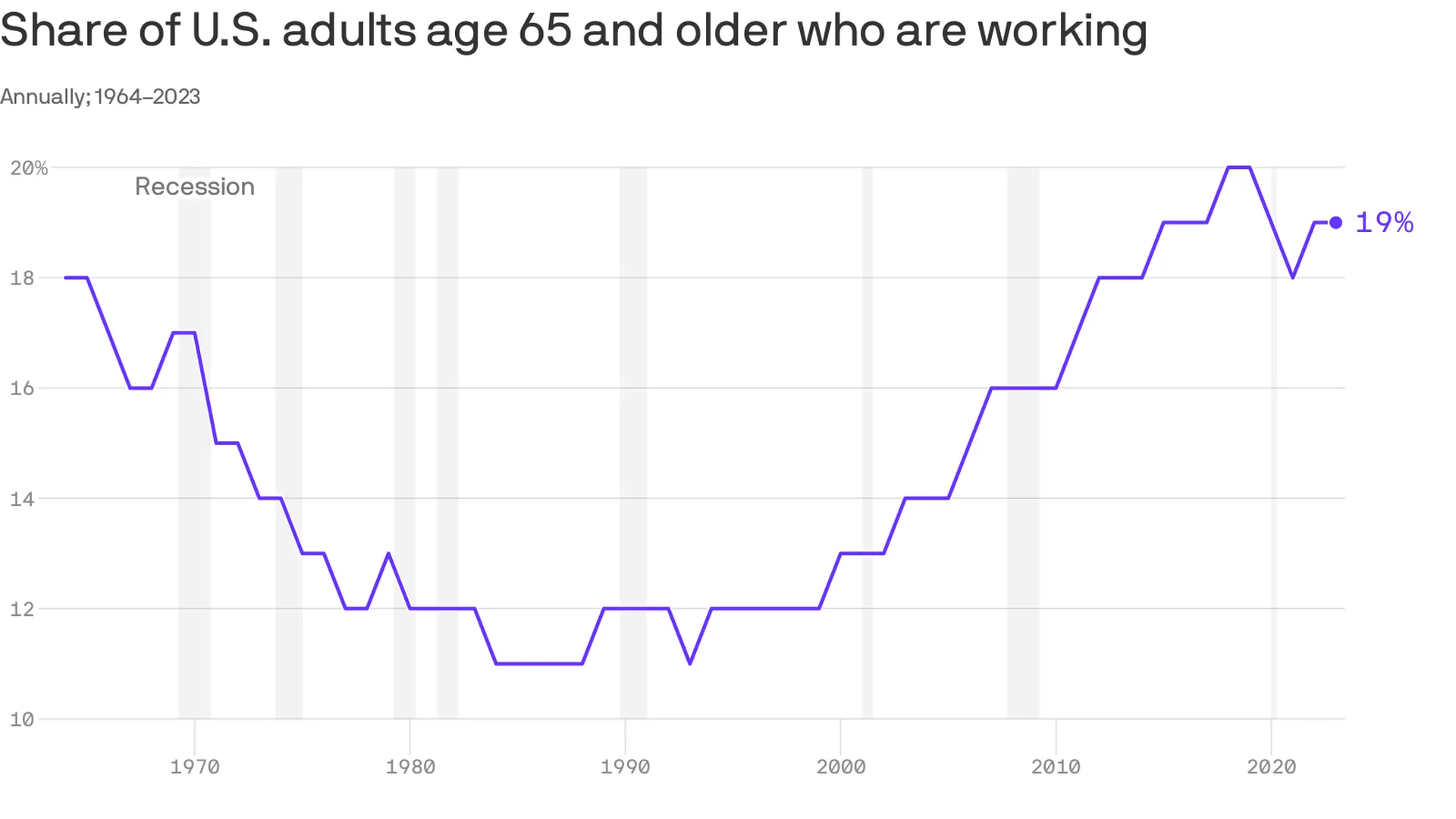
A new generation of doctors struggling with ever-increasing workloads and crushing student debt is helping drive unionization efforts in a profession that historically hasn’t organized.
Why it matters:
Physicians in training, like their peers in other industries, increasingly see unions as a way to boost their pay and protect themselves against grueling working conditions as they launch their careers.
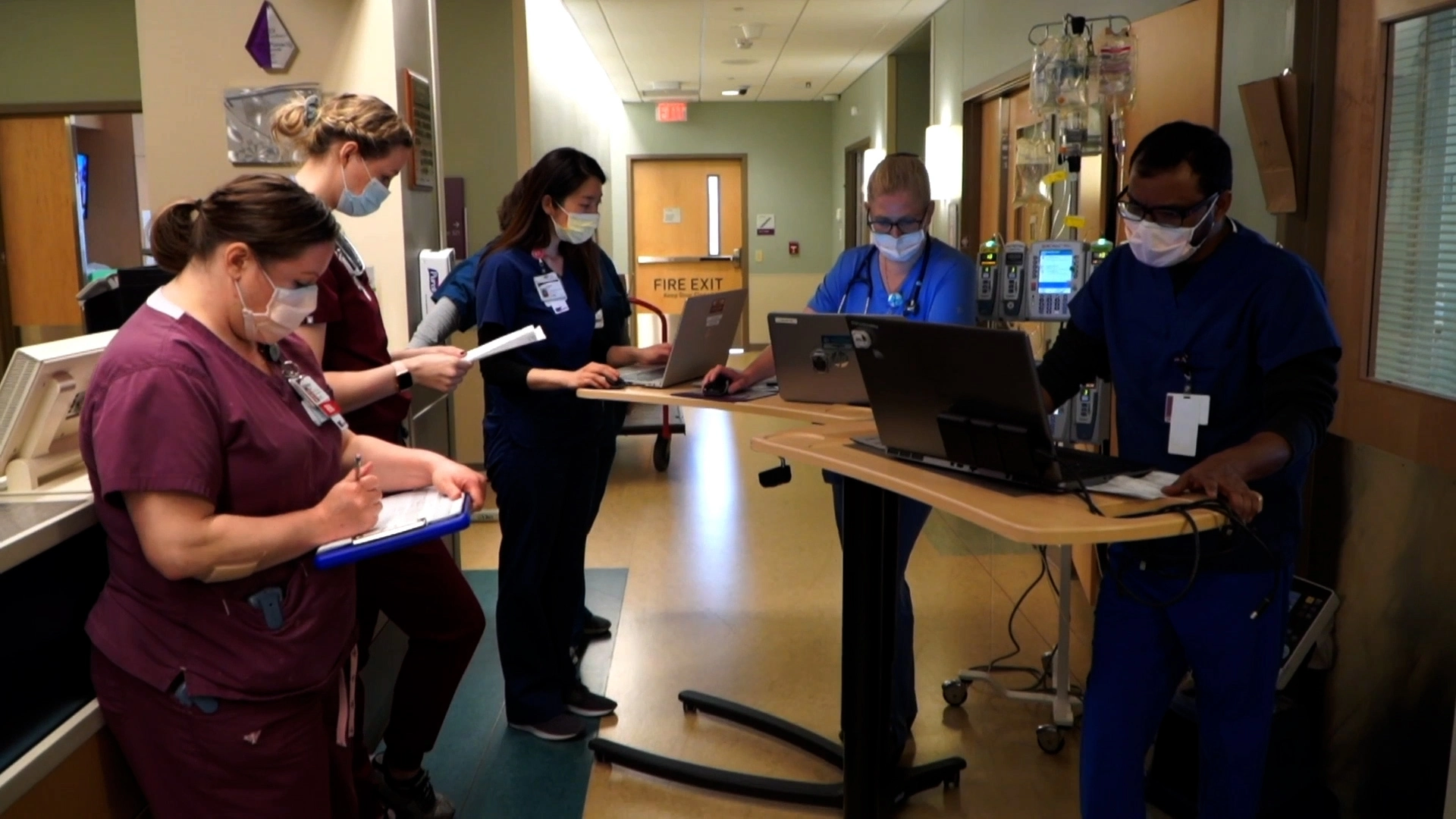
- It also comes amid a wave of unionization and labor actions by nurses and other caregivers across a health care system that’s still dealing with high levels of burnout.
What they’re saying:
“We deserve an increased salary to be able to afford to live in one of the most expensive areas in the United States,” said Ali Duffens, a third-year internal medicine resident at Kaiser Permanente’s San Francisco Medical Center.
- She’s among the 400 residents at Kaiser’s Northern California system filing to unionize earlier this month.
- Duffens earns about $82,000 per year, while paying $3,000 a month for rent and facing $350,000 in medical school loans.
The big picture:
The Kaiser residents are part of a growing number of younger peers in medicine who have been unionizing in recent years.
- The number of medical residents in unions has about doubled to more than 32,000 in three years, per CalMatters.
- In the last year, residents at Montefiore Medical Center, Stanford Health Care, George Washington University and the University of Pennsylvania voted to unionize, per WBUR.
- “The cost of day care … in a month is about half of my salary in total, and the cost of a nanny is essentially the entirety of my salary,” Leah Rethy, an internal medicine resident with Penn Medicine, told NPR last year.
- Residents can work as much as 80 hours per week while earning far less than their older colleagues.
Yes, but: Just about 6%-7% of physicians are estimated to be in unions.
- Historically, doctors have thought they could just suck up the long hours and relatively low pay in training as part of the tradition of medicine, said Robert Wachter, chair of the department of medicine at the University of California, San Francisco.
- “For a new generation, they look at it and say, ‘That’s crazy. I can’t believe you did that. I want to work hard, but I also want a life and I want a family, and I want a reasonable income,'” he said.
And it’s not just younger doctors.
Those more established in their careers are also unionizing as they see the industry changing in ways that they think undermine their profession.
- In recent months, attending physicians at Salem Hospital, owned by Mass General Brigham, and a Cedars Sinai-owned anesthesiology practice filed to unionize.
- About 600 doctors at Allina Health in Minnesota and Wisconsin last fall agreed to form what appears to be the largest union of private sector physicians.
Zoom in:
The corporatization of American medicine is seen as a key driver. More than half of all U.S. doctors now work for a health system or large medical group rather than running an independent practice.
- This shift has brought heavier workloads and less control over how they care for patients, said John August, director of health care labor relations in the Scheinman Institute on Conflict Resolution at the ILR School at Cornell.
- That could mean demands to see more patients, limiting the time that doctors can spend with them.
- “What you will hear from them 100% of the time in every conversation they have is they feel that they have lost control over the patient-physician relationship. I mean, every single physician says that now,” August said.
The other side:
Health systems and large practices generally say they value their doctors and the relationships they hold with patients.
- Hospitals have also struggled with pandemic-era financial shortfalls, including increasing labor costs.
The bottom line:
While this is a labor issue, it ultimately trickles down to quality and safety for patients, said Rachel Flores, organizing director of the Union of American Physicians and Dentists.
- “Patients should care because that’s less time to address their issues,” she said. “Patients should care because there’s not enough staff to support the physician.”