Hospitals in California are being warned not to violate state law on staffing levels or face fines. New state policy narrows the circumstances under which hospitals can claim “unpredictable circumstances” for violating the mandate.
The California Department of Public Health this week, in a notice to hospitals, warned that noncompliance can result in a $15,000 fine for a first violation and $30,000 for a second.
The state conducts periodic, unannounced inspections to enforce compliance.
New policy by Governor Newsom narrows the circumstances under which hospitals will not be penalized for violations due to “unpredictable circumstances,” requiring them to document efforts to maintain safe staffing and that such instances be truly unforeseen.
In an advisory letter to hospitals, the public health department said, “Situations that are not considered unpredictable, unknown or uncontrollable include consistent, ongoing patterns of understaffing. Facilities are expected to maintain required nurse-to-patient ratios at all times, including but not limited to, weekends, holidays, leaves of absences, among others.”
WHY THIS MATTERS
Minimum staffing ratios have been law in California since nurses and healthcare workers fought to pass AB 394, the nation’s first nurse-patient staffing ratio law in 1999.
In addition, SB 227, which passed in 2019, requires the state to assess administrative fines on hospitals that violate the safe staffing law. Law AB 1422 requires public comment before the public health department grants waivers to the critical care program flexibility requests.
THE LARGER TREND
Nurse staffing ratios are controversial and California remains the only state to have enacted them.
A study reportedly commissioned by the Centers for Medicare and Medicaid Services said there was “no single staffing level that would guarantee quality care.”
The NIH looked at survey data from 22,336 hospital staff nurses in California, Pennsylvania and New Jersey in 2006 and state hospital discharge databases. California hospital nurses cared for one less patient on average than nurses in the other states and two fewer patients in medical and surgical units, the NIH research said.
The study found that lower ratios were associated with significantly lower mortality. When nurses’ workloads were in line with California-mandated ratios in all three states, nurses’ burnout and job dissatisfaction were lower, and nurses reported consistently better quality of care, the NIH said.
Also, the hospital nurse staffing ratios in California were associated with better nurse retention than in the other states.
ON THE RECORD
“Patients in California are safer today because nurses and healthcare workers demanded that hospitals be held accountable for violating safe-staffing laws,” said Leo Pérez, RN and president of SEIU 121RN. “The COVID-19 pandemic taught us that our state’s health depends on supporting and listening to those who are on the front lines of patient care – a lesson we should never forget. Today’s action is the result of SEIU’s relentless vigilance. We applaud the step CDPH has taken to enforce laws that keep patients safe.”
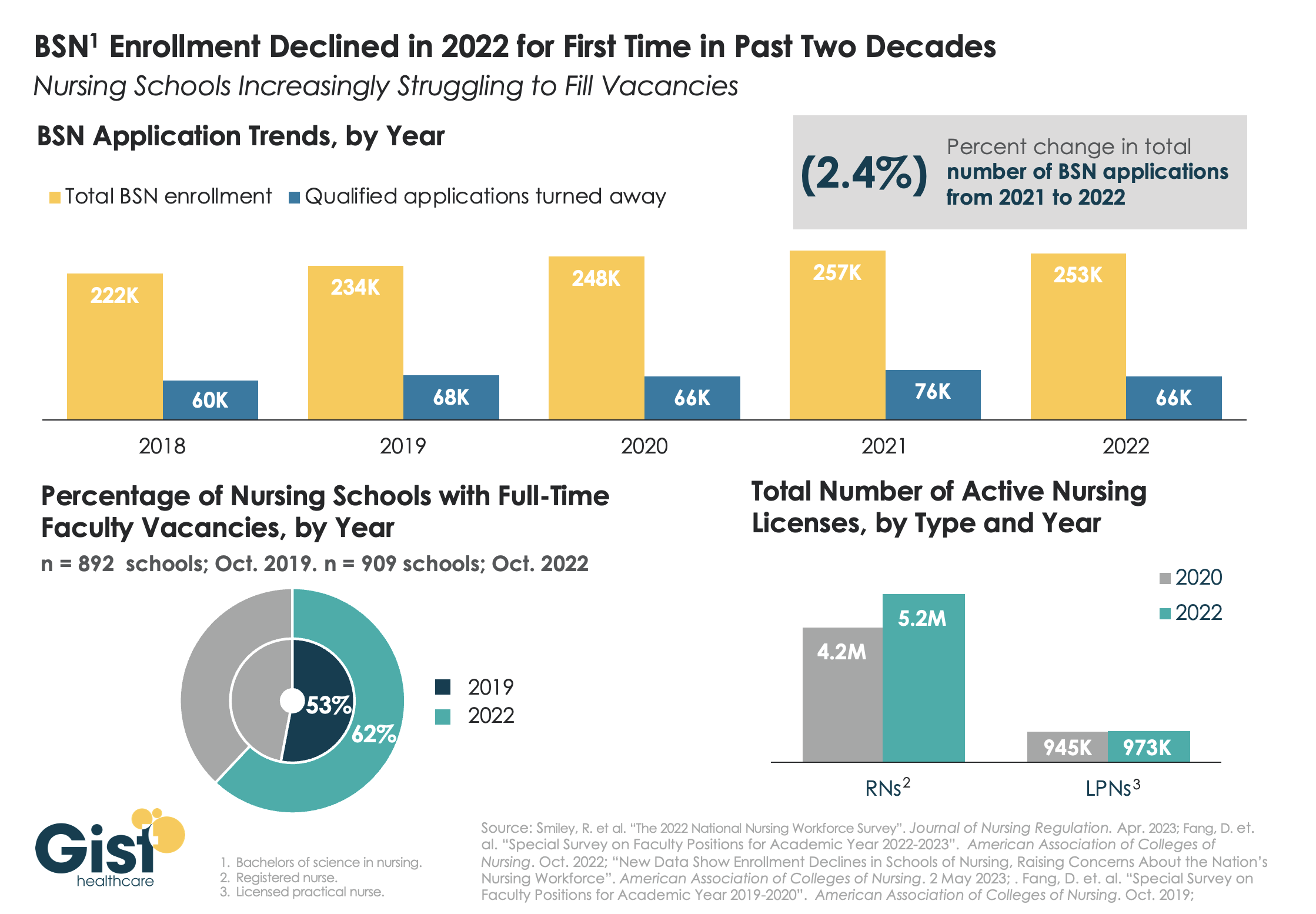
While last week’s graphic looked at how a wave of retirements has hit the nursing workforce, this week we take a look at the pipeline of nurses in training to fill that gap. In recent years, there has been a consistent stream of qualified applicants who want to become BSN nurses, but schools don’t have the capacity to admit them.
One reason: an ongoing shortage of nursing faculty, which recent retirements have exacerbated. The percentage of nursing schools with at least one full-time faculty vacancy grew from53 percent in 2019 to 62 percent in 2022.
Looking at registered nurses (RNs), the number with active licenses has continued to grow at a much higher rate than the supply of licensed practice nurses (LPNs) with active licenses.
The relatively small LPN workforce is especially significant, given rising interest in team-based nursing care, which aims to utilize a higher number of LPNs, supervised by RNs and BSNs.
Expanding training programs with an eye toward the skills and mix needed to deliver team-based care will be critical to ensuring a stable, efficient nursing workforce for future decades.
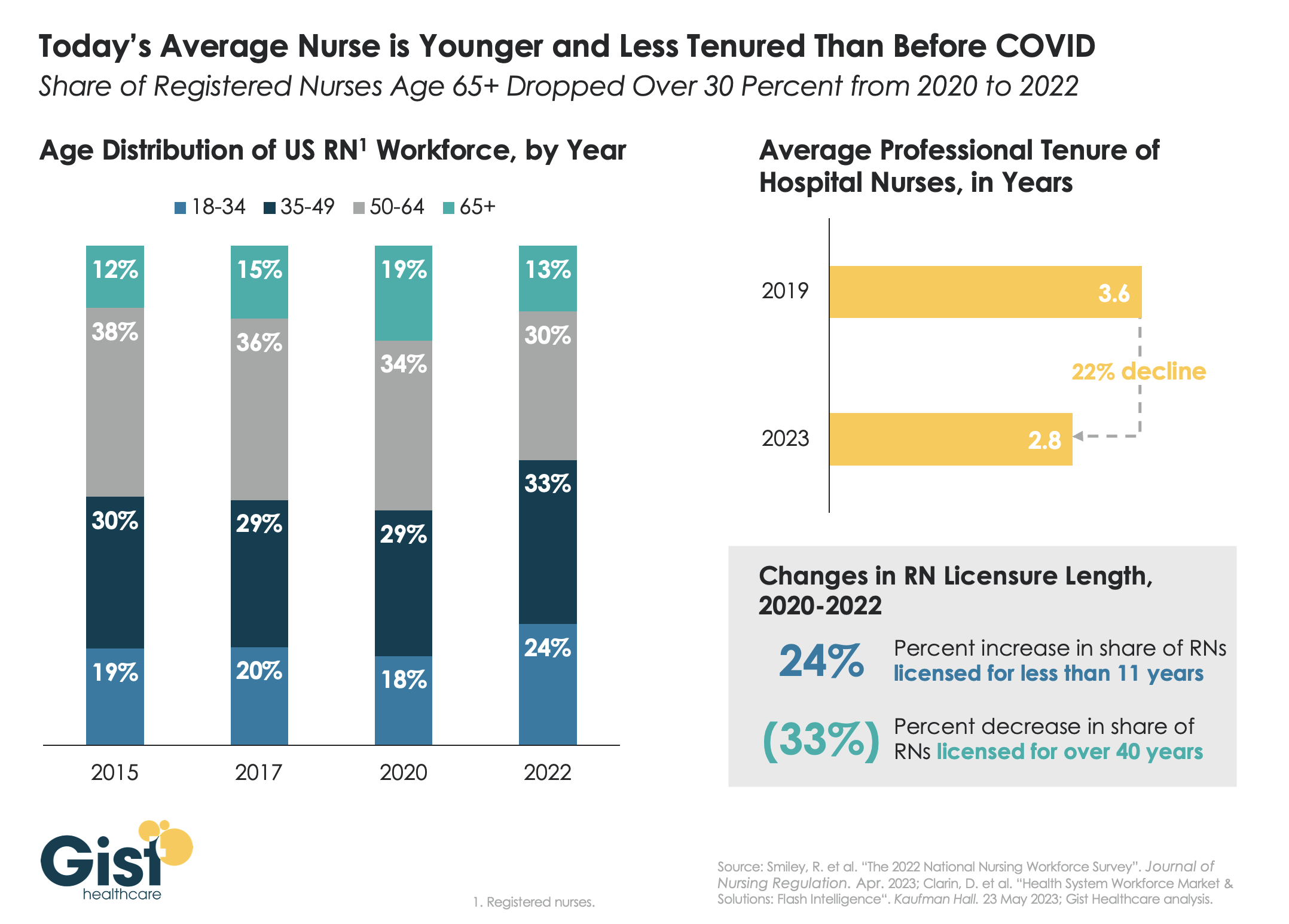
Last week we discussed how hospitals are still struggling to retain talent. This week’s graphic offers one explanation for this trend:
a significant share of older nurses, who continued to work during the height of the pandemic, have now exited the workforce, and health systems are even more reliant on younger nurses.
Between 2020 and 2022, the number of nurses ages 65 and older decreased by 200K, resulting in a reduction of that age cohort from 19 percent to 13 percent of the total nursing workforce. While the total number of nurses in the workforce still increased, the younger nurses filling these roles are both earlier in their nursing careers (thus less experienced), and more likely to change jobs.
Case in point:
From 2019 to 2023, the average tenure of a hospital nurse dropped by 22 percent. The wave of Baby Boomer nurse retirements has also resulted in a 33 percent decrease from 2020 to 2022 in the number of registered nurses who have been licensed for over 40 years.
Given these shifts, hospitals must adjust their current recruitment, retention, training, and mentorship initiatives to match the needs of younger, early-career nurses.
More than a year after launching an in-house travel staffing agency, UPMC is adding a new regional approach to the effort.
Maribeth McLaughlin, MPM, BSN, RN, chief nursing executive for the Pittsburgh-based health system, told Becker’s the approach provides a new option for nurses and surgical technologists who desire to travel.
“Our overall travel program, when you travel for us, you travel across our hospitals in New York, Maryland and Pennsylvania,” she said. “And now we are launching a regional travel strategy where some staff can choose to travel only within certain regions.”
UPMC initially announced in December 2021 that it had created UPMC Travel Staffing, a new in-house travel staffing agency to address a nursing shortage and to attract and retain workers.
Through the agency, nurses and surgical technologists earn $85 an hour and $63 an hour, respectively, in addition to a $2,880 stipend at the beginning of each six-week assignment.
Ms. McLaughlin said the rate is lower — about $60 an hour — for those who opt for the regional approach.
As of June 1, UPMC has hired more than 700 staff into the in-house travel staffing agency, with 60 percent of those workers being external hires, according to Ms. McLaughlin. And there have been fewer workers leaving UPMC to go to other travel agencies.
“One of my goals since I’ve taken this role is to really look at building in as many flexible programs as I could for staff,” said Ms. McLaughlin, who has served in her current role since August 2022. “I think as we came out of the pandemic, it’s clear to me that work-life harmony means something different to staff today than it maybe meant when I was a young staff nurse years ago, and that we need to have as much flexibility and as many different programs as we can.”
She said UPMC Travel Staffing has delivered this flexibility and allowed the health system to cancel about 90 contracts with external travel agencies. Additionally, some external travelers have now moved into UPMC’s in-house agency. Ms. McLaughlin expects more to join the in-house agency now that UPMC has launched the regional approach.
“We’re launching a win-back program where we’re going out and trying to see some of the people who we know we lost and see if they’re interested in coming back closer to home and traveling closer to home,” she explained.
Still, she acknowledged some of the challenges along the way.
“Our IT department built us an app to be able to manage all of this because, as you can imagine, we have external travel, internal travelers, core staff and at times it could get a little confusing,” said Ms. McLaughlin. “So we’ve been able to build that to be able to figure out the best ways to assign the staff where the greatest needs are.”
Another challenge she noted is that shifts for workers from external travel agencies are often 12 weeks, while shifts with UPMC Travel Staffing are six weeks. She said this is a purposeful move because those in UPMC Travel Staffing receive benefits and are considered UPMC employees, rather than receiving an hourly rate.
“Overall, it’s been a really successful program for us because it’s allowed us to look at things in a different way,” said Ms. McLaughlin. “It’s a central function. It’s not something we did and farmed out to every hospital to administer themselves. We did it as a system and as a core, which I also think is important.”
Now, she said she’s excited about the new regional approach and the opportunities it presents for recruiting and retention.
“We’re growing our own students, we’re bringing in all these students, and we’re not saying, ‘You have to just work here.’ We’re saying, ‘You can work for us at UPMC, and here are all the options. You can even be a traveler with us,'” she said.
During the pandemic, many nurses left hospital staff jobs for more lucrative travel jobs. However, many of these nurses are returning to hospitals for full-time positions, especially as travel pay falls and organizations offer new staff benefits, Melanie Evans writes for the Wall Street Journal.
Hospitals see more nurses return to their positions
During the pandemic, many hospitals struggled with staffing shortages as many nurses left their positions as a result of burnout or for more high-paying travel opportunities. However, many nurses are now returning to staff positions, especially as travel pay declines.
According to Aya Healthcare CEO Alan Braynin, travel nurse pay is now down 28% compared to a year ago. Hospital openings for travel nurses were also down by 51% at the end of April compared to the same time last year.
At HCA Healthcare, the country’s largest publicly traded hospital chain, nurse hiring increased by 19% in the first three months of the year compared to the average across the last four quarters. In addition, turnover levels have almost declined to pre-pandemic levels, and HCA’s travel nurse costs have dropped by 21% in the first quarter of this year compared to 2022.
According to the organization, many nurses who initially left their hospitals during the pandemic are now coming back. Since 2022, around 20% of the 37,000 nurses hired at HCA hospitals previously worked for the company at some point between 2016 and 2022.
Similarly, Houston Methodist has rehired around 60 nurses who initially left during the pandemic. Roberta Schwartz, the chief innovation officer at the health system’s flagship hospital, said these returning nurses have helped the hospital make more beds available and keep up with an 8% increase in demand.
“The boomerang nurses have returned,” said Gail Vozzella, Houston Methodist’s chief nurse.
How hospitals are attracting boomerang nurses
To attract more nurses to staff positions, hospital officials said they are offering higher pay, as well as several new benefits, such as childcare, less demanding work positions, and more flexible schedules.
For example, Suzane Nguyen, who took a teaching job during the pandemic, rejoined Houston Methodist in June 2022 after she was offered a virtual job. In her new position, she collects patient information by video. “The stress doesn’t compare,” she said.
Similarly, Linda Allen, an ED nurse who left to work for a temporary agency during the pandemic, returned to Sentara Healthcare in 2022 after the hospital system increased its wages and offered new, more flexible schedules.
According to Terrie Edwards, Sentara’s regional VP, the organization has increased its nurse wages by around 21% in the last two years and now offers student debt relief up to $10,000, as well as adoption and infertility benefits.
Overall, these changes have helped Sentara hire around 400 boomerang nurses, which has reduced staff overtime and cut its travel nurse expenses in half.
“They really did step up,” said Allen, who became a full-time employee in September 2022 after initially working temporary 13-week contracts.
Outside of these benefits, some nurses are also just ready for more permanent positions after spending the pandemic working in several different hospitals. “There is something to be said for working in the same place every day, consistently,” said Alexis Brockting, an advanced practice nurse at Mercy Hospital South.
Addressing the education pipeline is one thing that legislators could focus on to improve nurse and physician shortages, medical school and health system leaders said.
As the healthcare industry continues to face pandemic-driven workforce challenges, lawmakers are exploring ways to boost the number of clinicians practicing in the U.S.
“A shortage of healthcare personnel was a problem before the pandemic and now it has gotten worse,” Chairman Sen. Bernie Sanders I-Vt., said during a Thursday Senate HELP committee hearing. “Health care jobs have gotten more challenging and, in some cases, more dangerous,” he said.
Hospitals are currently facing shortages of registered nurses as burnout and other factors drive them to other roles.
For example, 47-hospital system Ochsner Health in New Orleans has about 1,200 open nursing positions, Chief Academic Officer Leonardo Seoane said at Thursday’s hearing.
The workforce shortaged led Ochsner to close about 100 beds across its system during the past six months, leading to it use already-constrained emergency departments as holding bays for patients, he said.
Like other systems, labor costs have also been a concern due to a continued reliance on temporary staff to fill gaps. Ochsner’s non-agency labor costs grew just under 60% since 2019, while its costs for contract staff grew nearly 900%, he said.
“Our country is perilously short of nurses, and those we do have are often not working in the settings that could provide the most value,” Sarah Szanton, dean of Johns Hopkins School of Nursing said.
“This was true before the pandemic and has become more acute,” she said.
While many nurses left permanent roles for higher-paying contract positions during the pandemic, others have turned to jobs at outpatient clinics, coinciding with a shift toward non-hospital based care.
Registered nurse employment is nearly 5% above where it was in 2019, with nearly all that growth occurring outside of hospitals, Douglas Staiger, a professor of economics at Dartmouth College, found in his research and said at the hearing.
One major concern: Driving current and projected shortages in hospitals that lawmakers can address is the educational pipeline, medical school and health system leaders said.
Educational programs for nurses and physicians face site shortages and educators who are often allured by other higher-paying jobs in the industry.
Nursing educators in Vermont earn about $65,000 a year — about half of what nurses with similar degrees working in hospitals earn, Sanders said during the hearing. He asked members to consider expanding the Nurse Corps and nurse faculty loan repayments, among other programs.
Supporting partnerships between universities and hospitals to create more training opportunities is another way Congress can help, along with addressing high costs of tuition, James Herbert, president of University of New England, said during the hearing.
“Scholarship and loan repayment programs are critical to make healthcare education more accessible for those who would otherwise find it out of reach,” Herbert said.
That includes expanding and improving Medicare-funded physician residencies, he said.
Creating a more diverse workforce that looks more like the population it serves is another important task, and one lawmakers can address by supporting historically black colleges and universities.
Federal funding could help improve classrooms and other infrastructure at HBCUs “that have been egregiously are underfunded for decades,” in addition to expanding Medicare-funded residencies for hospitals that train a large number of graduates for HBCU medical schools, said James Hildreth Sr., president and CEO at Meharry Medical College in Nashville.
The American Hospital Association submitted a statement to the HELP subcommittee and said it also supports increasing the number of residency slots eligible for Medicare funds and rejecting cuts to curb long-term physician shortages.
Other AHA supported policies to address current and long-term workforce shortages include better funding for nursing schools and supporting expedited visas for foreign-trained nurses.
AHA also asked lawmakers to look into travel nurse staffing agencies, reviving requests it made last year alleging that staffing companies engaged in price gouging during the pandemic.
Monday’s walkout of tens of thousands of nurses and ambulance staff was the largest in the NHS’s 75-year history.
Labor demonstrations have been ongoing across the past few months, as workers demand higher pay and better working conditions amid rampant national inflation and increased workloads.
Specific demands vary by union and nation within the United Kingdom. Welsh nurses called off their strike this week to review a proposal from Wales’ Labour Party-run government, while the Royal College of Nurses, the UK’s largest nursing union, has countered a nominal 5 percent pay increase proposal with demands for a five percent pay raise on top of inflation, which topped 10 percent in Britain in December.
The Gist: A glance at our neighbors across the pond shows that the US healthcare system is not the only one currently experiencing a labor crisis.
The UK’s nationalized system has also failed to shield its workers from the combined impact of COVID burnout and inflation. But the NHS, as the UK’s largest employer and perennial object of political maneuvering, is more susceptible to organized labor actions.
In contrast, American healthcare unions, which only covered 17 percent of the country’s nurses in 2021, must negotiate with local employers, whose responses to their demands vary.
While this may enhance the bargaining power of US health system leaders, it also heightensthe risk that we will fail to adequately secure our nursing workforce, a key national resource already in short supply, for the longer term.
As hospitals and health system leaders continue to grapple with persistently high nursing vacancy rates and severe staffing challenges, and face growing pressure to cut costs, we’re beginning to hear serious—if paradoxical—consideration being given to sharpening the axe, with an eye on a long-standing sacred cow: “Magnet” status.
For years, leading systems have invested significant time and resources to earn Magnet status, a designation of nursing quality granted by the American Nursing Association through its American Nurses’ Credentialing Center. Applying for—and then renewing—the designation can cost millions of dollars and involve significant process changes and staff time. In return, participants can market themselves as “Magnet hospitals”, presumably garnering additional patient business and giving them a leg up in recruiting high-quality nurses. At a time of severe nursing shortage, you might expect interest in earning or maintaining Magnet status to be spiking.
But that’s not what we’re hearing. “It’s just too expensive,” shared one system CEO recently. “We haven’t really seen it move the needle on volume, and our Magnet-designated facilities are just as stretched as the non-Magnet ones, with equally low morale.” Plus, at a time when the ability to pursue flexible staffing models is at a premium, keeping up with Magnet standards is increasingly handcuffing some hospitals looking to evaluate alternative staffing solutions.
“We can achieve all of the benefits of Magnet without having to jump through their hoops on process and data collection,” a system chief nursing officer told us. “We’re working on our own, internally-branded alternative to Magnet—something our own staff comes up with, rather than something artificially imposed from an outside organization.”
Ironically, this may be another area—like the battle against contract labor—in which systems now find themselves aligned with nursing unions, which have long opposed the Magnet program as just a marketing gimmick. There’s no question that programs like Magnet have helped increase the visibility of nursing as a driver of quality care. But given the current economic environment, it’ll be interesting to see how much hospitals are willing to continue to invest to maintain the designation.
The majority of hospitals are predicted to have negative margins in 2022, marking the worst year financially for hospitals since the beginning of the Covid-19 pandemic.
In Part 1 of Radio Advisory’s Hospital of the Future series, host Rachel (Rae) Woods invites Advisory Board experts Monica Westhead, Colin Gelbaugh, and Aaron Mauck to discuss why factors like workforce shortages, post-acute financial instability, and growing competition are contributing to this troubling financial landscape and how hospitals are tackling these problems.
As we emerge from the global pandemic, health care is restructuring. What decisions should you be making, and what do you need to know to make them? Explore the state of the health care industry and its outlook for next year by visiting advisory.com/HealthCare2023.
Radio Advisory’s Rachel Woods sat down with Optum EVP Dr. Jim Bonnette to discuss the sustainability of modern-day hospitals and why scaling down might be the best strategy for a stable future.
Rachel Woods:When I talk about hospitals of the future, I think it’s very easy for folks to think about something that feels very futuristic, the Jetsons, Star Trek, pick your example here. But you have a very different take when it comes to the hospital, the future, and it’s one that’s perhaps a lot more streamlined than even the hospitals that we have today. Why is that your take?
Jim Bonnette: My concern about hospital future is that when people think about the technology side of it, they forget that there’s no technology that I can name that has lowered health care costs that’s been implemented in a hospital. Everything I can think of has increased costs and I don’t think that’s sustainable for the future.
And so looking at how hospitals have to function, I think the things that hospitals do that should no longer be in the hospital need to move out and they need to move out now. I think that there are a large number of procedures that could safely and easily be done in a lower cost setting, in an ASC for example, that is still done in hospitals because we still pay for them that way. I’m not sure that’s going to continue.
Woods: And to be honest, we’ve talked about that shift, I think about the outpatient shift. We’ve been talking about that for several years but you just said the change needs to happen now. Why is the impetus for this change very different today than maybe it was two, three, four, five years ago? Why is this change going to be frankly forced upon hospitals in the very near future, if not already?
Bonnette: Part of the explanation is regarding the issues that have been pushed regarding price transparency. So if employers can see the difference between the charges for an ASC and an HOPD department, which are often quite dramatic, they’re going to be looking to say to their brokers, “Well, what’s the network that involves ASCs and not hospitals?” And that data hasn’t been so easily available in the past, and I think economic times are different now.
We’re not in a hyper growth phase, we’re not where the economy’s performing super at the moment and if interest rates keep going up, things are going to slow down more. So I think employers are going to become more sensitized to prices that they haven’t been in the past. Regardless of the requirements under the Consolidated Appropriations Act, which require employers to know the costs, which they didn’t have to know before. They’re just going to more sensitive to price.
Woods: I completely agree with you by the way, that employers are a key catalyst here and we’ve certainly seen a few very active employers and some that are very passive and I too am interested to see what role they play or do they all take much more of an active role.
And I think some people would be surprised that it’s not necessarily consumers themselves that are the big catalyst for change on where they’re going to get care, how they want to receive care. It’s the employers that are going to be making those decisions as purchasers themselves.
Bonnette: I agree and they’re the ultimate payers. For most commercial insurance employers are the ultimate payers, not the insurance companies. And it’s a cost of care share for patients, but the majority of the money comes from the employers. So it’s basically cutting into their profits.
Woods: We are on the same page, but I’m going to be honest, I’m not sure that all of our listeners are right. We’re talking about why these changes could happen soon, but when I have conversations with folks, they still think about a future of a more consolidated hospital, a more outpatient focused practice is something that is coming but is still far enough in the future that there’s some time to prepare for.
I guess my question is what do you say to that pushback? And are there any inflection points that you’re watching for that would really need to hit for this kind of change to hit all hospitals, to be something that we see across the industry?
Bonnette: So when I look at hospitals in general, I don’t see them as much different than they were 20 years ago. We have talked about this movement for a long time, but hospitals are dragging their feet and realistically it’s because they still get paid the same way until we start thinking about how we pay differently or refuse to pay for certain kinds of things in a hospital setting, the inertia is such that they’re going to keep doing it.
Again, I think the push from employers and most likely the brokers are going to force this change sooner rather than later, but that’s still probably between three and five years because there’s so much inertia in health care.
On the other hand, we are hitting sort of an unsustainable phase of cost. The other thing that people don’t talk about very much that I think is important is there’s only so many dollars that are going to health care.
And if you look at the last 10 years, the growth in pharmaceutical spend has to eat into the dollars available for everybody else. So a pharmaceutical spend is growing much faster than anything else, the dollars are going to come out of somebody’s hide and then next logical target is the hospital.
Woods: And we talked last week about how slim hospital margins are, how many of them are actually negative. And what we didn’t mention that is top of mind for me after we just come out of this election is that there’s actually not a lot of appetite for the government to step in and shore up hospitals.
There’s a lot of feeling that they’ve done their due diligence, they stepped in when they needed to at the beginning of the Covid crisis and they shouldn’t need to again. That kind of savior is probably not their outside of very specific circumstances.
Bonnette: I agree. I think it’s highly unlikely that the government is going to step in to rescue hospitals. And part of that comes from the perception about pricing, which I’m sure Congress gets lots of complaints about the prices from hospitals.
And in addition, you’ll notice that the for-profit hospitals don’t have negative margins. They may not be quite as good as they were before, but they’re not negative, which tells me there’s an operational inefficiency in the not for-profit hospitals that doesn’t exist in the for-profits.
Woods: This is where I wanted to go next. So let’s say that a hospital, a health system decides the new path forward is to become smaller, to become cheaper, to become more streamlined, and to decide what specifically needs to happen in the hospital versus elsewhere in our organization.
Maybe I know where you’re going next, but do you have an example of an organization who has had this success already that we can learn from?
Bonnette: Not in the not-for-profit section, no. In the for-profits, yes, because they have already started moving into ambulatory surgery centers. So Tenet has a huge practice of ambulatory surgery centers. It generates high margins.
So, I used to run ambulatory surgery centers in a for-profit system. And so think about ASCs get paid half as much as a hospital for a procedure, and my margin on that business in those ASCs was 40% to 50%. Whereas in the hospital the margin was about 7% and so even though the total dollars were less, my margin was higher because it’s so much more efficient. And the for-profits already recognize this.
Woods: And I’m guessing you’re going to tell me you want to see not-for-profit hospitals make these moves too? Or is there a different move that they should be making?
Bonnette: No, I think they have to. I think there are things beyond just ASCs though, for example, medical patients who can be treated at home should not be in the hospital. Most not-for-profits lose money on every medical admission.
Now, when I worked for a for-profit, I didn’t lose money on every Medicare patient that was a medical patient. We had a 7% margin so it’s doable. Again, it’s efficiency of care delivery and it’s attention to detail, which sometimes in a not-for-profit friends, that just doesn’t happen.