Companies are turning to interim financial leadership more frequently as they struggle to fill widening gaps in their accounting and finance functions.
Dive Brief:
Demand for interim financial leadership skyrocketed last year, with requests for interim CFOs jumping by 46%, according to a report by Business Talent Group, a Heidrick & Struggles company.
As well as interim CFO leadership, requests for on-demand talent with skills in key areas of finance also jumped; requests for talent that’s skilled in audit, accounting and financial controls have increased 33%, while those for FP&A and modeling skills increased 28%, the report found.
The rise in demand for audit, accounting and similar skills is “a logical consequence of the declining pipeline of accounting majors and CPA candidates,” Jack Castonguay, an assistant professor of accounting at New York’s Hofstra University, said in an email.
Dive Insight:
Competition to nab skilled accounting talent has only become fiercer in recent years amid a worsening shortage of accounting professionals, leaving companies with critical gaps in their financial leadership and function.
In addition to surging demand for interim CFOs, requests for senior vice president or vice president-level financial professionals — such as controllers and the heads of financial planning & analysis — rose by 114%, according to BTG.
When it comes to roles such as the head of FP&A or controllers, for example, “I think as you have shortages on one end, you’re going to have demand with organizations, whether it be full time or on-demand, for talent coming in,” Sunny Ackerman, global managing partner for on-demand talent at Heidrick & Struggles said in an interview. Ackerman does believe there is a link between the shortage in talent and the spike in requests for on-demand employees in these areas, she said. “So I think there is definitely a correlation for that.”
Historically, many companies have looked to fill roles in FP&A, audit, financial reporting and up to the CFO or controller chair with employees that have previously worked for an accounting firm, but dynamics have changed in recent years where many roles in accounting are now outsourced, Castonguay said.
“With accounting firm dynamics, largely insufficient salaries and work-life balance leaving firms struggling to attract people to the profession, the companies needing these people are now logically also struggling,” he said in an email. “You cannot disconnect the two.”
The narrower pipeline of new accounting graduates plus a high rate of retirement in the industry can leave the employees that are left overworked, increasing the likelihood of mistakes, according to a report by Fortune.
“Significant attrition” in the accounting department for retail brand Tupperware contributed to a delay in the company’s ability to file its annual 10-K form on time with the Securities and Exchange Commission, for example, the second consecutive year the brand will be filing late.
“Fewer grads lead to fewer public accountants which leads to fewer qualified and experienced hires for companies to place in their internal accounting-focused roles,” Castonguay said. “The dynamic makes me wonder how the temporary or outsourced staffing firms are finding candidates at their staffing firms. It’s possible that will be the next shoe to drop.”
On the labor side, changing ways of working may also be impacting how employees want to work; while there may be shortages in certain areas, the company is not necessarily seeing a slowdown of new candidates joining their platform, Ackerman said.
“So I think, even though there’s shortages in certain areas, I think talent is looking at this way of working differently than they did five years ago, and more companies are engaging with it,” she said.
Companies may also be more motivated to try out on-demand talent as they look to plug critical skill gaps in their workforces. Ninety-five percent of executives said they anticipate difficulty finding the “ideal combination of skills, capacity and expertise” inside their teams, BTG’s report said.
Today’s companies “now are starting to really open up and look at how they can blend full time talent with more independent talent and tapping into those capabilities at the desired time,” Ackerman said.
That includes how they might be approaching interim leadership; many firms are looking for on-demand talent to help provide critical support for larger-scale projects or initiatives, according to BTG, a category that makes up 27% of all talent requests.
Interim leadership can provide benefits to companies who are in transition or who are undertaking major changes, according to a 2023 CFO Dive report citing BTG data from that year.
An interim controller, for example, could take point on business process optimization for the business to successfully execute such a project; “the CFO or that finance function is quite a bit of a right hand, I would say to the executive suite,” Ackerman said.
Health systems are recovering from the worst financial year in recent history. We surveyed strategic planners to find out their top priorities for 2024 and where they are focusing their energy to achieve growth and sustainability. Read on to explore the top six findings from this year’s survey.
Research questions
With this survey, we sought the answers to five key questions:
How do health system margins, volumes, capital spending, and FTEs compare to 2022 levels?
How will rebounding demand impact financial performance?
How will strategic priorities change in 2024?
How will capital spending priorities change next year?
Bigger is Better for Financial Recovery
What did we find?
Hospitals are beginning to recover from the lowest financial points of 2022, where they experienced persistently negative operating margins. In 2023, the majority of respondents to our survey expected positive changes in operating margins, total margins, and capital spending. However, less than half of the sample expected increases in full-time employee (FTE) count. Even as many organizations reported progress in 2023, challenges to workforce recovery persisted.
40%
Of respondents are experiencing margins below 2022 levels
Importantly, the sample was relatively split between those who are improving financial performance and those who aren’t. While 53% of respondents projected a positive change to operating margins in 2023, 40% expected negative changes to margin.
One exception to this split is large health systems. Large health systems projected above-average recovery of FTE counts, volume, and operating margins. This will give them a higher-than-average capital spending budget.
Why does this matter?
These findings echo an industry-wide consensus on improved financial performance in 2023. However, zooming in on the data revealed that the rising tide isn’t lifting all boats. Unequal financial recovery, especially between large and small health systems, can impact the balance of independent, community, and smaller providers in a market in a few ways. Big organizations can get bigger by leveraging their financial position to acquire less resourced health systems, hospitals, or provider groups. This can be a lifeline for some providers if the larger organization has the resources to keep services running. But it can be a critical threat to other providers that cannot keep up with the increasing scale of competitors.
Variation in financial performance can also exacerbate existing inequities by widening gaps in access. A key stakeholder here is rural providers. Rural providers are particularly vulnerable to financial pressures and have faced higher rates of closure than urban hospitals. Closures and consolidation among these providers will widen healthcare deserts. Closures also have the potential to alter payer and case mix (and pressure capacity) at nearby hospitals.
Volumes are decoupled from margins
What did we find?
Positive changes to FTE counts, reduced contract labor costs, and returning demand led the majority of respondents in our survey to project organizational-wide volume growth in 2023. However, a significant portion of the sample is not successfully translating volume growth to margin recovery.
44%
Of respondents who project volume increases also predict declining margins
On one hand, 84% of our sample expected to achieve volume growth in 2023. And 38% of respondents expected 2023 volume to exceed 2022 volume by over 5%. But only 53% of respondents expected their 2023 operating margins to grow — and most of those expected that the growth would be under 5%. Over 40% of respondents that reported increases in volume simultaneously projected declining margins.
Why does this matter?
Health systems struggled to generate sufficient revenue during the pandemic because of reduced demand for profitable elective procedures. It is troubling that despite significant projected returns to inpatient and outpatient volumes, these volumes are failing to pull their weight in margin contribution. This is happening in the backdrop of continued outpatient migration that is placing downward pressure on profitable inpatient volumes.
There are a variety of factors contributing to this phenomenon. Significant inflationary pressures on supplies and drugs have driven up the cost of providing care. Delays in patient discharge to post-acute settings further exacerbate this issue, despite shrinking contract labor costs. Reimbursements have not yet caught up to these costs, and several systems report facing increased denials and delays in reimbursement for care. However, there are also internal factors to consider. Strategists from our study believe there are outsized opportunities to make improvements in clinical operational efficiency — especially in care variation reduction, operating room scheduling, and inpatient management for complex patients.
Strategists look to technology to stretch capital budgets
What did we find?
Capital budgets will improve in 2024, albeit modestly. Sixty-three percent of respondents expect to increase expenditures, but only a quarter anticipate an increase of 6% or more. With smaller budget increases, only some priorities will get funded, and strategists will have to pick and choose.
Respondents were consistent on their top priority. Investments in IT and digital health remained the number one priority in both 2022 and 2023. Other priorities shifted. Spending on areas core to operations, like facility maintenance and medical equipment, increased in importance. Interest in funding for new ambulatory facilities saw the biggest change, falling down two places.
Why does this matter?
Capital budgets for health systems may be increasing, but not enough. With the high cost of borrowing and continued uncertainty, health systems still face a constrained environment. Strategists are looking to get the biggest bang for their buck. Technology investments are a way to do that. Digital solutions promise high impact without the expense or risk of other moves, like building new facilities, which is why strategists continue to prioritize spending on technology.
The value proposition of investing in technology has changed with recent advances in artificial intelligence (AI), and our respondents expressed a high level of interest in AI solutions. New applications of AI in healthcare offer greater efficiencies across workforce, clinical and administrative operations, and patient engagement — all areas of key concern for any health system today.
Building is reserved for those with the largest budgets
What did we find?
Another way to stretch capital budgets is investing in facility improvements rather than new buildings. This allows health systems to minimize investment size and risk. Our survey found that, in general, strategists are prioritizing capital spending on repairs and renovation while deprioritizing building new ambulatory facilities.
When the responses to our survey are broken out by organization type, a different story emerges. The largest health systems are spending in ways other systems are not. Systems with six or more hospitals are increasing their overall capital expenditures and are planning to invest in new facilities. In contrast, other systems are not increasing their overall budgets and decreasing investments in new facilities.
AMCs are the only exception. While they are decreasing their overall budget, they are increasing their spending on new inpatient facilities.
Why does this matter?
Health systems seek to attract patients with new facilities — but only the biggest systems can invest in building outpatient and inpatient facilities. The high ranking of repairs in overall capital expenditure priorities suggests that all systems are trying to compete by maintaining or improving their current facilities. Will renovations be enough in the face of expanded building from better financed systems? The urgency to respond to the pandemic-accelerated outpatient shift means that building decisions made today, especially in outpatient facilities, could affect competition for years to come. And our survey responses suggest that only the largest health system will get the important first-mover advantage in this space.
AMCs are taking a different tack in the face of tight budgets and increased competition. Instead of trying to compete across the board, AMCs are marshaling resources for redeployment toward inpatient facilities. This aligns with their core identity as a higher acuity and specialty care providers.
Partnerships and affiliations offer potential solutions for health systems that lack the resources for building new facilities. Health systems use partnerships to trade volumes based on complexity. Partnerships can help some health systems to protect local volumes while still offering appropriate acute care at their partner organization. In addition, partnerships help health systems capture more of the patient journey through shared referrals. In both of these cases, partnerships or affiliations mitigate the need to build new inpatient or outpatient facilities to keep patients.
Eighty percent of respondents to our survey continued to lose patient volumes in 2023. Despite this threat to traditional revenue, health systems are turning from revenue diversification practices. Respondents were less likely to operate an innovation center or invest in early-stage companies in 2023. Strategists also reported notably less participation in downside risk arrangements, with a 27% decline from 2022 to 2023.
Why does this matter?
The retreat from revenue diversification and risk arrangements suggests that health systems have little appetite for financial uncertainty. Health systems are focusing on financial stabilization in the short term and forgoing practices that could benefit them, and their patients, in the long term.
Strategists should be cautious of this approach. Retrenchment on innovation and value-based care will hold health systems back as they confront ongoing disruption. New models of care, patient engagement, and payment will be necessary to stabilize operations and finances. Turning from these programs to save money now risks costing health systems in the future.
Market intelligence and strategic planning are essential for health systems as they navigate these decisions. Holding back on initiatives or pursuing them in resource-constrained environments is easier when you have a clear course for the future and can limit reactionary cuts.
Advisory Board’s long-standing research on developing strategy suggests five principles for focused strategy development:
Strategic plans should confront complexity. Sift through potential future market disruptions and opportunities to establish a handful of governing market assumptions to guide strategy.
Ground strategy development in answers to a handful of questions regarding future competitive advantage. Ask yourself: What will it take to become the provider of choice?
Communicate overarching strategy with a clear, coherent statement that communicates your overall health system identity.
A strategic vision should be supported by a limited number of directly relevant priorities. Resist the temptation to fill out “pro forma” strategic plan.
Pair strategic priorities with detailed execution plans, including initiative roadmaps and clear lines of accountability.
Strategists align on a strategic vision to go back to basics
What did we find?
Despite uneven recovery, health systems widely agree on which strategic initiatives they will focus more on, and which they will focus less on. Health system leaders are focusing their attention on core operations — margins, quality, and workforce — the basics of system success. They aim to achieve this mandate in three ways. First, through improving efficiency in care delivery and supply chain. Second, by transforming key elements of the care delivery system. And lastly, through leveraging technology and the virtual environment to expand job flexibility and reduce administrative burden.
Health systems in our survey are least likely to take drastic steps like cutting pay or expensive steps like making acquisitions. But they’re also not looking to downsize; divesting and merging is off the table for most organizations going into 2024.
Why does this matter?
The strategic priorities healthcare leaders are working toward are necessary but certainly not easy. These priorities reflect the key challenges for a health system — margins, quality, and workforce. Luckily, most of strategists’ top priorities hold promise for addressing all three areas.
This triple mandate of improving margins, quality, and workforce seems simple in theory but is hard to get right in practice. Integrating all three core dimensions into the rollout of a strategic initiative will amplify that initiative’s success. But, neglecting one dimension can diminish returns. For example, focusing on operational efficiency to increase margins is important, but it’ll be even more effective if efforts also seek to improve quality. It may be less effective if you fail to consider clinicians’ workflow.
Health systems that can return to the basics, and master them, are setting a strong foundation for future growth. This growth will be much more difficult to attain without getting your house in order first.
Vendors and other health system partners should understand that systems are looking to ace the basics, not reinvent the wheel. Vendors should ensure their products have a clear and provable return on investment and can map to health systems’ strategic priorities. Some key solutions health systems will be looking for to meet these priorities are enhanced, easy-to-follow data tools for clinical operations, supply chain and logistics, and quality. Health systems will also be interested in tools that easily integrate into provider workflow, like SDOH screening and resources or ambient listening scribes.
Going back to basics
Craft your strategy
1. Rebuild your workforce.
One important link to recovery of volume is FTE count. Systems that expect positive changes in FTEs overwhelmingly project positive changes in volume. But, on average, less than half of systems expected FTE growth in 2023. Meanwhile, high turnover, churn, and early retirement has contributed to poor care team communication and a growing experience-complexity gap. Prioritize rebuilding your workforce with these steps:
Recover: Ensure staff recover from pandemic-era experiences by investing in workforce well-being. Audit existing wellness initiatives to maximize programs that work well, and rethink those that aren’t heavily utilized.
Recruit: Compete by addressing what the next generation of clinicians want from employment: autonomy, flexibility, benefits, and diversity, equity, and inclusion (DEI). Keep up to date with workforce trends for key roles such as advance practice providers, nurses, and physicians in your market to avoid blind spots.
Retain: Support young and entry-level staff early and often while ensuring tenured staff feel valued and are given priority access to new workforce arrangements like hybrid and gig work. Utilize virtual inpatient nurses and virtual hubs to maintain experienced staff who may otherwise retire. Prioritize technologies that reduce the burden on staff, rather than creating another box to check, like ambient listening or asynchronous questionnaires.
2. Become the provider of choice with patient-centric care.
Becoming the provider of choice is crucial not only for returning to financial stability, but also for sustained growth. To become the provider of choice in 2024, systems must address faltering consumer perspectives with a patient-centric approach. Keep in mind that our first set of recommendations around workforce recovery are precursors to improving patient-centered care. Here are two key areas to focus on:
Front door: Ensure a multimodal front door strategy. This could be accomplished through partnership or ownership but should include assets like urgent care/extended hour appointments, community education and engagement, and a good digital experience.
Social determinants of health: A key aspect of patient-centered care is addressing the social needs of patients. Our survey found that addressing SDOH was the second highest strategic priority in 2023. Set up a plan to integrate SDOH screenings early on in patient contact. Then, work with local organizations and/or build out key services within your system to address social needs that appear most frequently in your population. Finally, your workforce DEI strategy should focus on diversity in clinical and leadership staff, as well as teaching clinicians how to practice with cultural humility.
3. Recouple volume and margins.
The increasingly decoupled relationship between volume and margins should be a concern for all strategists. There are three parts to improving volume related margins: increasing volume for high-revenue procedures, managing costs, and improving clinical operational efficiency.
Revenue growth: Craft a response to out-of-market travel for surgery. In many markets, the pool of lucrative inpatient surgical volumes is shrinking. Health systems are looking to new markets to attract patients who are willing to travel for greater access and quality. Read our findings to learn more about what you need to attract and/or defend patient volumes from out-of-market travel.
Cost reduction: Although there are many paths health systems can take to manage costs, focusing on tactics which are the most likely to result in fast returns and higher, more sustainable savings, will be key. Some tactics health systems can deploy include preventing unnecessary surgical supply waste, making employees accountable for their health costs, and reinforcing nurse-led sepsis protocols.
Clinical operational efficiency: The number one strategic priority in 2023, according to our survey, was clinical operational efficiency, no doubt in response to faltering margins. Within this area, the top place for improvement was care variation reduction (CVR). Ensure you’re making the most out of CVR efforts by effectively prioritizing where to spend your time. Improve operational efficiency outside of CVR by improving OR efficiency and developing protocols for complex inpatient management.
The post-pandemic labor force has 1.5 million fewer individuals with some post-secondary education short of a bachelor’s degree. This shortfall is hitting healthcare hardest, affecting wages and qualification levels among jobholders.
Job vacancies requiring a post-secondary certificate or associate degree, particularly in healthcare, remain high. The mismatch between the supply of workers with this education level and the ongoing demand for them is leading to increased wages and greater reliance on more educated workers, according to a December 2023 bulletin from the Federal Reserve Bank of Kansas City.
Five takeaways from the bank’s report:
1. Before the pandemic, job openings across educational groups moved together and subsequently peaked together in mid-2022. Since then, while vacancies for most groups have fallen, the number of job vacancies requiring some college education remains 60% above its pre-pandemic level.
2. Vacancies for jobs requiring some college education are concentrated in healthcare. As of August 2023, about 50% of all open jobs posted in 2023 that required an associate degree or non-degree certificate were in healthcare.
3. As a result of the high demand, healthcare employers are turning to more educated workers to fill positions with requirements for some college education. Healthcare employment among workers with some college education has dropped by about 400,000 since 2019; healthcare employment among workers with a bachelor’s degree or more has increased by 600,000.
4. Combined, these factors can place upward pressure on healthcare wages. The supply-demand mismatch can lead employers to offer higher wages to competitively attract qualified workers. Employers turning to workers with more education, who are generally more expensive, will increase the average wage in these occupations.
5. From 2019 to 2023, overall wages for healthcare workers rose by nearly 25%, an increase the bank partially attributes to both increased wages within educational groups and composition effects. The shift in employment toward higher-educated workers accounts for an additional 2.7 percentage points of the total wage increase, for instance.
Robert Wood Johnson University Hospital in New Brunswick, N.J., said it plans to temporarily cut off healthcare benefits for striking union workers, effective Sept. 1.
Hospital spokesperson Wendy Gottsegen described the move as unfortunate.
“We have said all along that no one benefits from a strike — least of all our nurses. We hope the union considers the impact a prolonged strike is having on our nurses and their families,” Ms. Gottsegen said in an Aug. 28 news release shared with Becker’s. “As of Sept. 1, RWJUH nurses must pay for their health benefits through COBRA. This hardship, in addition to the loss of wages throughout the strike, is very unfortunate and has been openly communicated to the union and the striking nurses since prior to the walkout on Aug. 4.”
The ongoing strike involves the United Steelworkers Local 4-200, which represents about 1,700 nurses at the facility.
Union members voted to authorize a strike in July. The union and hospital have been negotiating a new agreement for months, with the last bargaining session occurring Aug. 16.
During negotiations, the union has said it seeks a contract that provides safe staffing standards, living wages and quality, affordable healthcare.
Local 4-200 President Judy Danella, RN, said in a previous union release, “Our members remain deeply committed to our patients. However, we must address urgent concerns, like staffing. We need enough nurses on each shift, on each floor, so we can devote more time to each patient and keep ourselves safe on the job.”
Several nurses told TAPinto New Brunswick last week that they began preparing for the current situation ahead of the strike, taking overtime shifts and saving as much money as possible. Others told the publication they are taking part-time jobs or temporary employment elsewhere in the nursing field or adjacent roles.
“I think it’s important that you [remember] you might not get the job you want to do at that moment, but people have to do what they have to do to get it done,” Jessica Newcomb, RN, told TAPinto New Brunswick.
Meanwhile, the hospital has contracted with an agency to hire replacement nurses during the strike.
“As always, our top priority is to our patients. RWJUH is open, fully operational and completely staffed, and we remain steadfast in our commitment to deliver the highest quality and always-safe patient care,” Ms. Gottsegen said.
As of Aug. 28, no further dates for negotiations were scheduled by mediators.
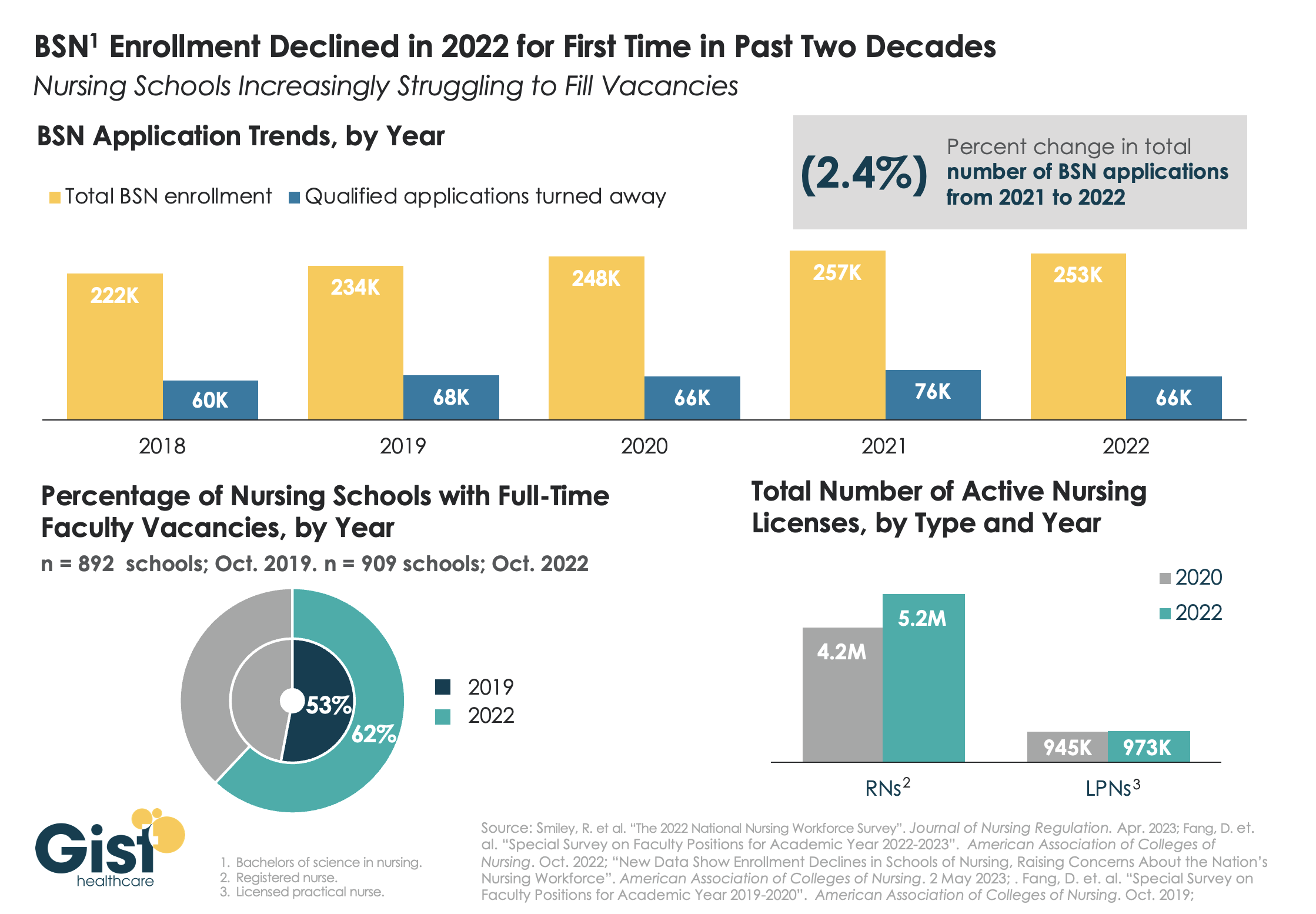
While last week’s graphic looked at how a wave of retirements has hit the nursing workforce, this week we take a look at the pipeline of nurses in training to fill that gap. In recent years, there has been a consistent stream of qualified applicants who want to become BSN nurses, but schools don’t have the capacity to admit them.
One reason: an ongoing shortage of nursing faculty, which recent retirements have exacerbated. The percentage of nursing schools with at least one full-time faculty vacancy grew from53 percent in 2019 to 62 percent in 2022.
Looking at registered nurses (RNs), the number with active licenses has continued to grow at a much higher rate than the supply of licensed practice nurses (LPNs) with active licenses.
The relatively small LPN workforce is especially significant, given rising interest in team-based nursing care, which aims to utilize a higher number of LPNs, supervised by RNs and BSNs.
Expanding training programs with an eye toward the skills and mix needed to deliver team-based care will be critical to ensuring a stable, efficient nursing workforce for future decades.
Hospital margins continued to stabilize in March with a slight improvement over February, according to data from Kaufman Hall’s National Hospital Flash Report. However, margins remain below pre-pandemic levels, leaving hospitals in a vulnerable position should a recession or a new public health emergency materialize.
For provider practices, physician productivity increased but the increased revenues could not keep pace expenses, according to the quarterly Physician Flash Report.
While things appear relatively calm at the moment, there remain significant challenges—specifically labor shortages and diminished margins—that could quickly reach the surface if hospitals and health systems are faced with another crisis.
Kaufman Hall experts are seeing increased reliance on advanced practice providers (APPs)—e.g. Nurse Practitioners and Physician Associates—and note that those that hire, retain and deploy this critical workforce most effectively will see more success in the long term.
Healthcare added almost 45,000 jobs in November, but many hospitals and health systems will continue to struggle to meet staffing needs, retain top executives and providers, and foster long-term pipelines for talent, Ted Chien, president and CEO of independent consulting firm SullivanCotter, wrote in a Dec. 15 article for Nasdaq.
Hospitals and health systems are living “paycheck to paycheck” and unable to make long-term investments at the height of the current workforce crisis, Mr. Chien said.
The challenge boils down to a healthcare delivery problem, not a demand problem.
Baby Boomers are the greatest source of care demand on the healthcare system, but are unable to contribute to the provider workforce in the numbers needed to achieve balance, according to Mr. Chien. To compound that issue, burnout is a major factor why “too many” frontline workers have left or plan to exit healthcare, he said.
Last year, an estimated 333,942 healthcare providers dropped out of the workforce, including about 53,000 nurse practitioners, which has led hospitals to spend more on contract labor and feeling more pressure to consolidate, according to an October report published by Definitive Healthcare.
Long term, a continued lack of healthcare workers would force hospitals to operate in a heightened crisis mode, according to Mr. Chien, depriving non-critical patients of sufficient health prevention and demanding too much of providers who are already overly taxed.
Mr. Chien highlighted three key areas to tackle the workforce crisis: smarter technology, resilient teams and excellent leadership.
Technologies that alleviate providers’ administrative burdens will be critical to reduce burnout and keep caregivers focused on patient care, while smarter tech can also forge pipelines for future providers by streamlining clinical experience operations and aligning student placements with existing opportunities.
Building resilient teams begins with competitive pay and robust benefit packages, which fosters trust and demonstrates that a hospital values its staff, according to Mr. Chen. Supporting career growth, including upskilling and redeploying staff when appropriate, empowers employees.
Lastly, capable executive leadership teams, under intense scrutiny from industry stakeholders, must clearly outline their hospital or health system’s strategy and provide the change needed to support their staff. Lack of trust in leaders drives staff out of healthcare, so it is crucial to recruit and retain “modern, strategic thinkers with depth of experience who are prepared to lead,” Mr. Chien wrote.