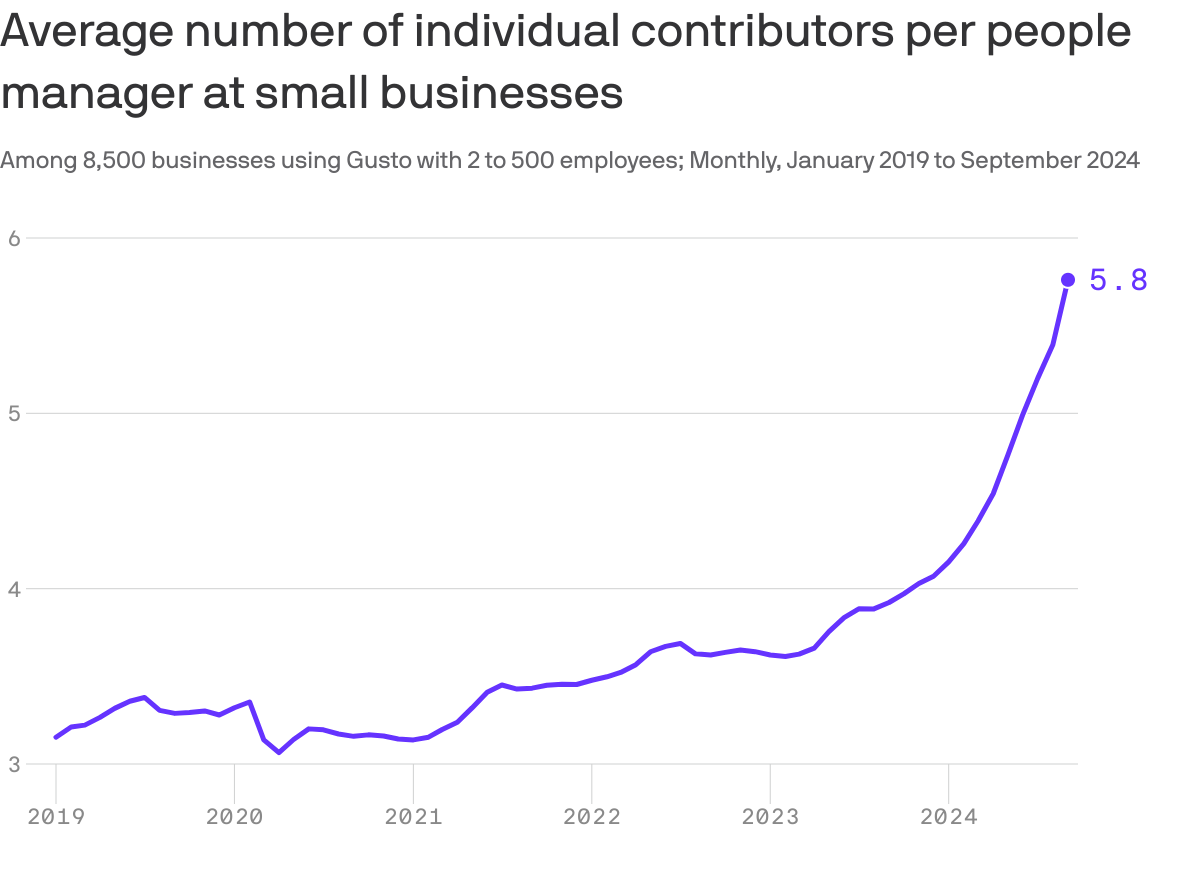
This chart may explain why your boss is taking longer to get back to you lately: They’ve got more underlings to watch over, Axios’ Emily Peck writes from a new analysis.
Why it matters: Middle managers — i.e., bosses who have bosses — were already quietly going extinct, and now AI may be hastening the process.
By the numbers:
People managers now oversee about twice as many workers as just five years ago.
There are now nearly six individual contributors per manager at the 8,500 small businesses analyzed in a report by Gusto, which handles payroll for small and medium-sized employers.
That’s up from a little over three in 2019.
🎨 The big picture:
Big Tech has been shedding middle managers for the past few years, a process that’s been dubbed the Great Flattening.
Reducing management layers is one of Microsoft’s stated goals in laying off thousands of workers this year as it ramps up its AI strategy.
Amazon CEO Andy Jassy last year announced an effort to reduce managers (memo).
Congress returns from its July 4 break today and its focus will be on the President: will he resign or tough it out through the election in 120 days. But not everyone is paying attention to this DC drama.
In fact, most are disgusted with the performance of the political system and looking for something better. Per Gallup, trust and confidence in the U.S. Congress is at an all-time low.
The same is true of the healthcare system:
69% think it’s fundamentally flawed and in need of systemic change vs. 7% who think otherwise (Keckley Poll). And 60% think it puts its profits above all else, laying the blame at all its major players—hospitals, insurers, physician, drug companies and their army of advisors and suppliers.
These feelings are strongly shared by its workforce, especially the caregivers and support personnel who service patient in hospital, clinic and long-term care facilities. Their ranks are growing, but their morale is sinking.
Career satisfaction among clinical professionals (nurses, physicians, dentists, counselors) is at all time low and burnout is at an all-time high.
Last Friday, the Bureau of Labor issued its June 2024 Jobs report. To no one’s surprise, job growth was steady (+206,000 for the month) –slightly ahead of its 3-month average (177,000) despite a stubborn inflation rate that’s hovered around 3.3% for 15 months. Healthcare providers accounted for 49,000 of those jobs–the biggest non-government industry employer.
But buried in the detail is a troubling finding: for hospital employment (NAICS 6221.3): productivity was up 5.9%, unit labor costs for the month were down 1.1% and hourly wages grew 4.8%–higher than other healthcare sectors.
For the 4.7 million rank and file directly employed in U.S. hospitals, these productivity gains are interpreted as harder work for less pay. Their wages have not kept pace with their performance improvements while executive pay seems unbridled.
Next weekend, the American Hospital Association will host its annual Leadership Summit in San Diego: 8 themes are its focus:
Building a More Flexible and Sustainable Workforce is among them. That’s appropriate and it’s urgent.
An optimistic view is that emergent technologies and AI will de-lever hospitals from their unmanageable labor cost spiral. Chief Human Resource Officers doubt it. Energizing and incentivizing technology-enabled self-care, expanding scope of practice opportunities for mid-level professionals and moving services out of hospitals are acknowledged keys, but guilds that protect licensing and professional training push back.
By contrast, the application of artificial intelligence to routine administrative tasks is more promising: reducing indirect costs (overhead) that accounts for a third of total spending is the biggest near-term opportunity and a welcome focus to payers and consumers.
Thus, most organizations advance workforce changes cautiously. That’s the first problem.
The second problem is this:
lack of a national healthcare workforce modernization strategy to secure, prepare and equip the health system to effectively perform. Section V of the Affordable Care Act (March 2010) authorized a national workforce commission to modernize the caregiver workforce. Due to funding, it was never implemented. It’s needed today more than ever. The roles of incentives, technologies, AI, data and clinical performance measurement were not considered in the workforce’ ACA charter: Today, they’re vital.
Transformational changes in how the healthcare workforce is composed, evaluated and funded needs fresh thinking and boldness. It must include input from new players and disavow sacred cows. It includes each organization’s stewardship and a national spotlight on modernization.
It’s easier to talk about healthcare’s workforce issues but It’s harder to fix them. That’s why incrementalism is the rule and transformational change just noise.
PS: In doing research for this report, I found wide variance in definitions and counts for the workforce. It may be as high as 24 million, and that does not include millions of unpaid caregivers. All the more reason to urgently address its modernization.
A number of hospitals and health systems are reducing their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations announced this year.
June
West Monroe, La.-based Glenwood Regional Medical Center, part of Dallas-based Steward Health Care, laid off 23 employees. Affected roles included leadership, a spokesperson for the hospital said in a statement shared with Becker’s.
Cleveland-based University Hospitals is reducing its leadership structure by more than 10% as part of more than 300 layoffs. COO Paul Hinchey, MD, told Becker’s C-suite level leaders and vice presidents were included in the cuts.
Portland-based Oregon Health & Science Universitytold staff June 6 that it plans to lay off at least 500 employees, citing financial issues. The news follows the institution and Portland-based Legacy Health signing a binding, definitive agreement to come together as one health system under OHSU Health.
May
The All of Us Research Program, a collaboration of the University of Arizona in Tucson and Phoenix-based Banner Health, plans to lay off 45 workers due to reduced federal research funding, according to an Arizona WARN notice filed May 28. The program, launched in 2018, is part of HHS’ National Institutes of Health.
Burlington, Mass.-based Tufts Medicine will lay off 174 employees due to industry challenges, the health system confirmed in a May 21 statement shared with Becker’s. The layoffs, which have varying effective dates, will primarily affect administrative and non-direct patient care roles. Some leadership roles were affected, a spokesperson told Becker’s.
Doral, Fla.-based Sanitas Medical Centerlaid off 56 employees between May 17 and May 20. Some of the affected roles included nine care coordinators, one care educator, and two case managers, according to a May 20 WARN notice accessed by Becker’s.
Select Specialty Hospital in Longview, Texas, will close on or about June 30, affecting 94 employees, Becker’s has confirmed. The hospital, operated by Mechanicsburg, Pa.-based Select Medical, is a 32-bed, critical illness recovery facility.
White Rock Medical Center in Dallaslaid off nearly 35% of its staff. The hospital temporarily stopped taking patients transported by emergency medical services due to the layoffs, The Dallas Morning News reported. It has since resumed accepting those patients.
Oakland-based Kaiser Foundation Hospitals is laying off 76 workers in California. The layoffs primarily affect employees in IT and marketing, according to regulatory documents filed with the state May 1.
April
Pittsburgh-based UPMC will lay off approximately 1,000 employees. The layoffs, which represent more than 1% of the health system’s 100,000 workforce will primarily affect nonclinical, administrative and non-member-facing employees.
Union Springs, Ala.-based Bullock County Hospitallaid off 95 employees beginning April 9, according to regulatory documents filed with the state. The layoffs occurred as Bullock seeks to become a rural emergency hospital and is ending psychiatric services as part of the shift, AL.com reported April 25.
Jackson Health Systemreduced compensation programs for senior leaders; laid off fewer than 25 people, including one hospital CEO; and froze many vacant positions, especially in support and nonclinical areas, a spokesperson for the Miami-based organization confirmed to Becker’s. President and CEO Carlos Migoya shared these efforts in a message to staff, citing financial challenges.
Coos Bay, Ore.-based Bay Area Hospital plans to conduct layoffs as it outsources its revenue cycle management operations, a spokesperson for the hospital confirmed to Becker’s. The transition will affect 27 positions.
Manchester, N.H.-based Catholic Medical Centerplans to cut 142 positions, including 54 layoffs. An April 18 letter to employees from CMC president and CEO Alex Walker, obtained by Becker’s, said cuts would occur through the 54 staff eliminations, open position cuts, reduced hours, planned departures, and resource redeployment in satellite locations for CMC.
Marshfield (Wis.) Clinic Health System will lay off furloughed staff, effective in early May. The health system furloughed about 3% of its workforce in January, affecting positions mostly in non-patient-seeing departments, including leadership roles.
Norwalk, Ohio-based Fisher-Titus Medical Centerlaid off some workers in nonclinical roles and reduced hours for others. Seven employees, about 0.5% of the health system’s workforce, were laid off April 1. Work hours were reduced for another 10 positions, a hospital spokesperson told Becker’s.
March
Robbinsdale, Minn.-based North Memorial Health is laying off 103 employees in clinical and nonclinical roles, citing financial challenges. The layoffs affect several services across the two-hospital system.
AHMC’s San Gabriel (Calif.) Valley Medical Center is laying off 62 workers, according to regulatory documents filed with the state March 13. The layoffs take effect May 13.
Miami-based North Shore Medical Center, part of Steward Health Care, started conducting layoffs as part of cuts to some of its programs amid the Dallas-based health system’s continued financial struggles. Around 152 workers represented by 1199SEIU were laid off, a union spokesperson confirmed. However that number could be higher as their members do not represent every employee at NSMC, the spokesperson said.
Oakland, Calif.-based Kaiser Foundation Hospitals is laying off more than 70 employees. The layoffs primarily affect those in IT roles.
February
Lion Star, the group that operates Nacogdoches (Texas) Memorial Hospital, is closing four of its clinics on March 22, which will result in fewer than 50 layoffs, a Lion Star spokesperson confirmed to Becker’s. No additional layoffs are planned.
Little Rock-based Arkansas Heart Hospital has laid off fewer than 50 employees since the beginning of 2024, citing low reimbursement rates. The layoffs affected lower-paying positions, Bruce Murphy, MD, CEO of the hospital, said, according to Arkansas Business.
Cincinnati-based Mercy Health will lay off some call center positions. The system attributed the move to its partnership with a third party to operate its enterprise contact center for primary care scheduling.
Ridgecrest (Calif.) Regional Hospital announced more layoffs to avoid closure. It is laying off 31 more employees, including seven licensed vocational nurses and four registered nurses, two months after it announced plans to lay off nearly 30 others and suspend its labor and delivery unit, Bakersfield.com reported Feb. 15.
Medford, Ore.-based Asante health system laid off about 3% of its workforce. The layoffs primarily affected administrative and support roles and were necessary to offset “financial headwinds” over the past several years, according to a report from NBC affiliate KOBI-TV, which is based on an internal memo sent to staff Feb. 9.
Oakdale, Calif.-based Oak Valley Hospital District is scaling back services and laying off workers to improve its finances. The hospital said in a Feb. 2 statement shared with Becker’s that it will close its five-bed intensive care unit, discontinue its family support network department and lay off 28 employees, including those in senior management and supervisor positions.
Chicago-based Rush University System for Healthlaid off an undisclosed number of workers in administrative and leadership positions, citing “financial headwinds affecting healthcare providers nationwide.” No additional information was provided about the layoffs, including the number of affected employees.
University of Chicago Medical Center laid off about 180 employees, or less than 2% of its roughly 13,000-person workforce. The majority of affected positions are not direct patient facing, the organization said in a statement shared with Becker’s.
Fountain Valley, Calif.-based MemorialCarelaid off 72 workers due to restructuring efforts at its Long Beach (Calif.) Medical Center and Long Beach, Calif.-based Miller Children’s and Women’s Hospital. The layoffs include 13 positions at Long Beach Medical Center’s outpatient retail pharmacy, which is closing Feb. 2, a spokesperson for MemorialCare said in a statement shared with Becker’s.
January
George Washington University Hospital in Washington, D.C., part of King of Prussia, Pa.-based Universal Health Services, is laying off “less than 3%” of its employees. The move is attributed to restructuring efforts.
Amarillo-based Northwest Texas Healthcare System, also part of Universal Health Services, announced plans to lay off a “limited number of positions.” The move is attributed to restructuring efforts.
Lehigh Valley Health Network is cutting its chiropractic services and laying off 10 chiropractors. The layoffs are effective April 12 and due to restructuring. The Allentown, Pa.-based health system has 10 chiropractic locations, according to its website.
Central Maine Healthcare is laying off 45 employees as part of management reorganization. The Lewiston-based system, which also ended urgent care services at its Maine Urgent Care on Sabattus Street in Lewiston on Jan. 12, has 3,100 employees total.
University of Vermont Health Network, based in Burlington, is cutting 130 open positions. The move is part of the health system’s efforts to reduce expenses by $20 million.
Med-Trans, a medical transport provider based in Lewisville, Texas,closed its UF Health ShandsCair base serving Gainesville, Fla.-based UF Health Shands Hospital on Jan. 10 due to decreased transportation demands. The move also resulted in layoffs, a spokesperson for UF Health, the hospital’s parent company, told Becker’s in a statement.
RWJBarnabas Health, based in West Orange, N.J., is laying off 79 employees, according to documents filed with the state on Jan. 8. The layoffs are effective March 31 and April 5. A spokesperson for the health system told Becker’s that 74 of the positions were “time-limited information technology training job functions.” The other layoffs were due to closure of an urgent care center.
Citing financial challenges, Cleveland-based University Hospitals is reducing its leadership structure by more than 10% as part of more than 300 layoffs.
Rising costs of supplies, labor and purchase services, and reduced Medicare reimbursement rates, have affected UH and various other systems, according to COO Paul Hinchey, MD.
“All of that’s creating significant downward pressure on our revenue,” Dr. Hinchey told Becker’s.
The news from UH follows a national trend of hospitals facing significant headwinds. Kaufman Hall found in early June that 40% of hospitals in the U.S. are still losing money.
At UH, revenue has increased nearly 9% year over year due to various changes, such as increased access for patients and implementing a new EHR system, according to UH.
“[However], in spite of our efforts and being successful in growth, that downward pressure on revenue and the increasing prices is pinching our margin,” said Dr. Hinchey.
Dr. Hinchey said the health system has been optimizing operations since the end of the pandemic.
“We took a look at our cost structure and recognized we needed to get our cost structure down,” he said. “We’ve done a couple initiatives that we put under the auspices of a Medicare break-even initiative to try to drive down our cost structure.”
Some actions already taken have included increasing efficiency, consolidating service lines and closing hospitals in Bedford and Richmond Heights, according to UH.
Most recently, the health system identified an opportunity to make cuts to leadership. Dr. Hinchey said C-suite level leaders and vice presidents were included in the cuts.
“These decisions are never easy,” Cliff Megerian, MD, CEO and Jane and Henry Meyer Chief Executive Officer Distinguished Chair, said in a news release. “The important thing is that we make these strategic moves now so we can continue to serve our community and fulfill our mission for decades to come. We are thankful for our hometown team that delivers lifesaving care to our neighbors, friends and relatives each and every day.”
Dr. Hinchey said UH began notifying employees of the layoffs on June 17. Affected workers will receive a severance package aligned with their roles and tenure.
Portland-based Oregon Health & Science University told staff June 6 that it plans to lay off at least 500 employees, citing financial issues.
“Our expenses, including supplies and labor costs, continue to outpace increases in revenue,” top leaders told staff in a message shared with Becker’s. “Despite our efforts to increase our revenue, our financial position requires difficult choices about internal structures, workforce and programs to ensure that we achieve our state-mandated missions and thrive over the long term.”
Willamette Week was first to report the news, which follows Oregon Health & Science University and Portland-based Legacy Health signing a binding, definitive agreement to come together as one health system under OHSU Health. OHSU Health would comprise 12 hospitals and, more than 32,000 employees and will be one of the largest providers of services to Medicaid members in Oregon.
An Oregon Health & Science University spokesperson told Becker’s more information about the layoffs will be provided in the coming weeks.
In the June 6 message, leaders told staff that “while we work to address short-term financial challenges, we must also plan for an impactful and successful future. We understand that last week’s announcement regarding the Legacy Health definitive agreement, while exciting and potentially transformational, raises questions about how we can afford the required investment in light of our financial situation.”
They added that a capital investment in Legacy “represents a strategic expansion designed to enhance our capacity,” and will be funded by borrowing with 30-year bonds.
“These capital dollars cannot be used to close gaps in our fiscal year 2025 OHSU budget or to pay our members. The OHSU Strategic Alignment and budgetary work would be necessary with or without the Legacy Health integration,” leaders said.
OHSU has planned a town hall next week to further discuss the combination with Legacy.
Leaders said discussions between managers and members about workforce reductions will begin after the annual review and contract renewal process, with additional reductions occurring over the next few months.
Hundreds of nurses at University Hospitals are facing a decrease in pay as the Cleveland-based health system pivots from its COVID-19 pandemic model, cleveland.com reported.
A spokesperson told Becker’s the pay adjustment is effective June 16 and applies to 350 Enterprise Staffing Services nurses.
“UH’s Enterprise Staffing Services is an in-house staffing agency formed in response to the once-in-a-lifetime global health pandemic that stretched our resources and workforce to the extreme,” a UH statement shared with Becker’s said. “During the pandemic, hospitals across the country (including UH) increased their use of agency nurses to fill gaps in staffing with government funding assistance, with agency costing up to twice as much or more than our hospital-based full-time nurses.
“Nurses are the heartbeat of our health system and we will never be able to thank them enough for their commitment and dedication to our patients during the pandemic. Unfortunately, the pandemic care model is not sustainable in today’s environment.”
The statement said those affected by the pay adjustment, representing 1% of the health system’s workforce, will still be paid about twice the national average.
Pay for staffing services nurses on night shift will decrease from $75 to $65 an hour, a 13% cut, UH said, according to cleveland.com, which obtained a health system memo related to the change. Pay for staffing services nurses on day shift will decrease 8%, from $60 to $55 an hour.
Pay for a new staffing services job without benefits will be $75 per hour for night shift, and $65 per hour for day shift, UH said in the memo, which also encouraged staffing services nurses to apply for other health system roles, according to cleveland.com.
“As we continue to exit from our pandemic model, external nursing staffing agencies and internal hospital nurse staffing agencies nationwide are adjusting pay accordingly,”
UH’s statement said. “We have provided cutting-edge, compassionate care to our neighbors in Northeast Ohio since 1866. We’re taking the appropriate steps to ensure we can continue fulfilling our mission for future generations.”
A number of hospitals and health systems are reducing their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations announced this year.
Editor’s Note: This webpage was created Jan. 19 and updated May 10.
May
White Rock Medical Center in Dallaslaid off nearly 35% of its staff. The hospital temporarily stopped taking patients transported by emergency medical services due to the layoffs, The Dallas Morning News reported. It has since resumed accepting those patients.
Oakland-based Kaiser Foundation Hospitals is laying off 76 workers in California. The layoffs primarily affect employees in IT and marketing, according to regulatory documents filed with the state May 1.
April
Pittsburgh-based UPMC will lay off approximately 1,000 employees. The layoffs, which represent more than 1% of the health system’s 100,000 workforce will primarily affect nonclinical, administrative and non-member-facing employees.
Union Springs, Ala.-based Bullock County Hospitallaid off 95 employees beginning April 9, according to regulatory documents filed with the state. The layoffs occurred as Bullock seeks to become a rural emergency hospital and is ending psychiatric services as part of the shift, AL.com reported April 25.
Jackson Health Systemreduced compensation programs for senior leaders; laid off fewer than 25 people, including one hospital CEO; and froze many vacant positions, especially in support and nonclinical areas, a spokesperson for the Miami-based organization confirmed to Becker’s. President and CEO Carlos Migoya shared these efforts in a message to staff, citing financial challenges.
Coos Bay, Ore.-based Bay Area Hospital plans to conduct layoffs as it outsources its revenue cycle management operations, a spokesperson for the hospital confirmed to Becker’s. The transition will affect 27 positions.
Manchester, N.H.-based Catholic Medical Centerplans to cut 142 positions, including 54 layoffs. An April 18 letter to employees from CMC president and CEO Alex Walker, obtained by Becker’s, said cuts would occur through the 54 staff eliminations, open position cuts, reduced hours, planned departures, and resource redeployment in satellite locations for CMC.
Marshfield (Wis.) Clinic Health System will lay off furloughed staff, effective in early May. The health system furloughed about 3% of its workforce in January, affecting positions mostly in non-patient-seeing departments, including leadership roles.
Norwalk, Ohio-based Fisher-Titus Medical Centerlaid off some workers in nonclinical roles and reduced hours for others. Seven employees, about 0.5% of the health system’s workforce, were laid off April 1. Work hours were reduced for another 10 positions, a hospital spokesperson told Becker’s.
March
Robbinsdale, Minn.-based North Memorial Health is laying off 103 employees in clinical and nonclinical roles, citing financial challenges. The layoffs affect several services across the two-hospital system.
AHMC’s San Gabriel (Calif.) Valley Medical Center is laying off 62 workers, according to regulatory documents filed with the state March 13. The layoffs take effect May 13.
Miami-based North Shore Medical Center, part of Steward Health Care, started conducting layoffs as part of cuts to some of its programs amid the Dallas-based health system’s continued financial struggles. Around 152 workers represented by 1199SEIU were laid off, a union spokesperson confirmed. However that number could be higher as their members do not represent every employee at NSMC, the spokesperson said.
Oakland, Calif.-based Kaiser Foundation Hospitals is laying off more than 70 employees. The layoffs primarily affect those in IT roles.
February
Lion Star, the group that operates Nacogdoches (Texas) Memorial Hospital, is closing four of its clinics on March 22, which will result in fewer than 50 layoffs, a Lion Star spokesperson confirmed to Becker’s. No additional layoffs are planned.
Little Rock-based Arkansas Heart Hospital has laid off fewer than 50 employees since the beginning of 2024, citing low reimbursement rates. The layoffs affected lower-paying positions, Bruce Murphy, MD, CEO of the hospital, said, according to Arkansas Business.
Cincinnati-based Mercy Health will lay off some call center positions. The system attributed the move to its partnership with a third party to operate its enterprise contact center for primary care scheduling.
Ridgecrest (Calif.) Regional Hospitalannounced more layoffs to avoid closure. It is laying off 31 more employees, including seven licensed vocational nurses and four registered nurses, two months after it announced plans to lay off nearly 30 others and suspend its labor and delivery unit, Bakersfield.com reported Feb. 15.
Medford, Ore.-based Asante health systemlaid off about 3% of its workforce. The layoffs primarily affected administrative and support roles and were necessary to offset “financial headwinds” over the past several years, according to a report from NBC affiliate KOBI-TV, which is based on an internal memo sent to staff Feb. 9.
Oakdale, Calif.-based Oak Valley Hospital District is scaling back services and laying off workers to improve its finances. The hospital said in a Feb. 2 statement shared with Becker’s that it will close its five-bed intensive care unit, discontinue its family support network department and lay off 28 employees, including those in senior management and supervisor positions.
Chicago-based Rush University System for Healthlaid off an undisclosed number of workers in administrative and leadership positions, citing “financial headwinds affecting healthcare providers nationwide.” No additional information was provided about the layoffs, including the number of affected employees.
University of Chicago Medical Center laid off about 180 employees, or less than 2% of its roughly 13,000-person workforce. The majority of affected positions are not direct patient facing, the organization said in a statement shared with Becker’s.
Fountain Valley, Calif.-based MemorialCarelaid off 72 workers due to restructuring efforts at its Long Beach (Calif.) Medical Center and Long Beach, Calif.-based Miller Children’s and Women’s Hospital. The layoffs include 13 positions at Long Beach Medical Center’s outpatient retail pharmacy, which is closing Feb. 2, a spokesperson for MemorialCare said in a statement shared with Becker’s.
January
George Washington University Hospital in Washington, D.C., part of King of Prussia, Pa.-based Universal Health Services, is laying off “less than 3%” of its employees. The move is attributed to restructuring efforts.
Amarillo-based Northwest Texas Healthcare System, also part of Universal Health Services, announced plans to lay off a “limited number of positions.” The move is attributed to restructuring efforts.
Lehigh Valley Health Network is cutting its chiropractic services and laying off 10 chiropractors. The layoffs are effective April 12 and due to restructuring. The Allentown, Pa.-based health system has 10 chiropractic locations, according to its website.
Central Maine Healthcare is laying off 45 employees as part of management reorganization. The Lewiston-based system, which also ended urgent care services at its Maine Urgent Care on Sabattus Street in Lewiston on Jan. 12, has 3,100 employees total.
University of Vermont Health Network, based in Burlington, is cutting 130 open positions. The move is part of the health system’s efforts to reduce expenses by $20 million.
Med-Trans, a medical transport provider based in Lewisville, Texas, closed its UF Health ShandsCair base serving Gainesville, Fla.-based UF Health Shands Hospital on Jan. 10 due to decreased transportation demands. The move also resulted in layoffs, a spokesperson for UF Health, the hospital’s parent company, told Becker’s in a statement.
RWJBarnabas Health, based in West Orange, N.J., is laying off 79 employees, according to documents filed with the state on Jan. 8. The layoffs are effective March 31 and April 5. A spokesperson for the health system told Becker’s that 74 of the positions were “time-limited information technology training job functions.” The other layoffs were due to closure of an urgent care center.
Expenses per provider remained considerably higher than revenue generated in the first quarter of 2024, although there are signs the gap could be closing, according to the Kaufman Hall “Physician Flash Report,” released May 2.
Kaufman Hall based their findings on a monthly report from Syntellis Performance Solutions, part of Strata. The report gathered data from more than 200,000 employed providers, including physicians and advanced practice providers.
Net patient revenue per provider full-time equivalent was $383,881 for the first quarter, up 4% from the same period last year. Total direct expenses per provider FTE hit $620,729 for the quarter. Expense growth has slowed over the last three years, with a 5% growth from 2022 to 2023 and just 3% growth from 2023 to 2024.
“Labor expenses are a growing proportion of total expenses, a trend that is unlikely to change significantly. Organizations should shift from optimizing downstream revenue to optimizing downstream margins,” the report authors advised, noting hospitals and physician organizations can evaluate provider specialties by outcomes or other metrics when they aren’t big revenue drivers.
Provider productivity was up 4% as measured by work relative value units. Physician wRVU per FTE was 5,979 for the first quarter, up 6% year over year. Physician compensation jumped 3% to $364,319, down from 6% growth between 2022 to 2023.
Labor expenses continue to rise while support staff decline across specialties. Labor was 84% of total expenses in the first quarter, and support staff per 10k provider wRVUs dropped 6% year over year to 3.14, even after an 8% drop from 2022 to 2023. Report authors recommended organizations find better ways to use APPs for higher physician productivity.
Here are specific data points from the first quarter report.
Median net patient revenue per provider FTE by specialty cohort were:
UPMC is laying off about 1,000 employees in a “realignment” the nonprofit said will help it face “the realities of a still-evolving, post-pandemic marketplace.”
The layoffs reflect about 1% of UPMC’s total workforce of over 100,000 people and are primarily among nonclinical and administrative staff, Vice President and Chief Communications Officer Paul Wood said in an emailed statement. He said the system will be offering those impacted “enhanced severance pay and benefits coverage.”
The “limited reductions” will also involve the closing of open positions, the elimination of redundancies and “other actions,” Wood said.
“This realignment will not alter UPMC’s investments in our communities, facilities, commitment to clinical care and research, strategic growth or to offering those throughout our workforce industry-leading benefits,” Wood wrote in the statement.
Pittsburgh-based UPMC is an integrated health system and one of Pennsylvania’s largest employers. Its provider, insurance and other business arms logged $27.7 billion of revenue across 2023 as volumes rose and insurance membership grew.
However, the nonprofit reported a $198.3 million operating loss (-0.7% operating margin) last year as insurance claims expenses jumped 13.6% and labor costs rose 6.4%. It had posted a $162 million operating gain (0.6% operating margin) the year before.
The system did narrow its 2023 bottom line loss to $31 million thanks to its investment returns, though it had logged roughly a billion in net losses during the 2022 fiscal year.
In its year-end financial report, UPMC’s management wrote that “even with increased expenses to deliver high-quality care as a result of various economic factors, in 2023 UPMC continued to forge ahead with investments to grow access to world-class clinical care … advance healthcare excellence through quality and innovation, care for our communities, grow our insurance services and invest in our future workforce.”