In my report June 10, I wrote: “The major sources of physician discontent are administrative hassles and unwelcome clinical oversight that create dissonance. They conflict with a false sense of autonomy that the majority of physicians imagined when choosing medicine. Cuts to reimbursement, participation in alternative payment models and medical inflation are manifestations of a system in which ‘suits’ are intruders who make rules, exact handsome salaries, generate corporate profits and distance physicians from patient care purposely… “
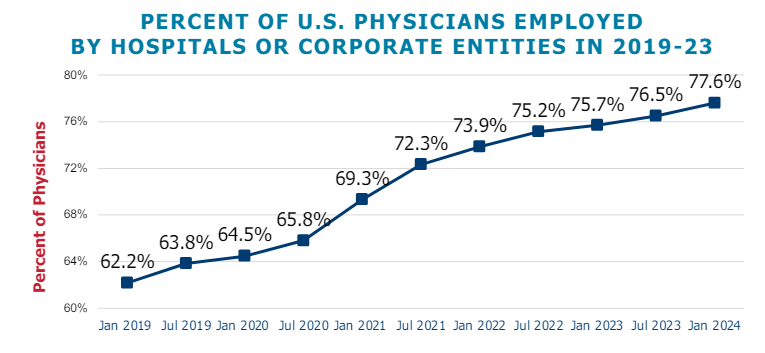
This assessment remains true today. Discontent among physicians is palpable and it’s magnified by a growing sense of financial despair among many clinicians. And it poses a unique challenge to hospitals that now employ more than half of America’s physician workforce.
In the “good ole days”, hospitals provided a place for physicians to ply their trade. They were credentialled to practice their chosen specialty, granted special parking, food and amenities and treated as the hospital’s most welcome customer. Made sense: physicians controlled most patient decisions about the hospital services they use. Physicians controlled the hospital’s revenue, sustainability and bonuses earned by administrators. Insurers brought privately-insured patients to doctors who charged them 1.6-2.5 times what Medicare paid and physician income was not threatened. That was then. This is now.
Today, insurers play a larger role. Consumer expectations have changed. Policymakers are paying more attention. And demand has shifted from inpatient services to outpatient, home and office settings for health and wellbeing services in addition to acute care. And the current forecast by CMS through 2032 predicts spending for hospitals will increase at a compound rate of 5.7% vs. 5.6% for physicians adding more hospital-physician financial tension to the system. Both well-above inflation and CDP growth prompting heightened pressure to spend less.
In anticipation, consolidation of hospitals into multi-hospital systems has been a staple in recent years: only 1 in 5 hospitals is independent these days, and most of these are small, rural or otherwise destined to independence for their uncertain future. Whether public, investor-owned or not-for-profit (or tax exempt as some prefer), the economic realities of running hospitals coupled with the regulatory constraints imposed by state and federal law forced all to re-think their future.And, for most, employing physicians directly was a means to an end of staying alive while the dust settles.
But the unintended consequence of physician employment is soured relationships between the employed physicians and their hospital:
their financial and emotional security has become tangled up by interactions with hospital leaders and former peers appointed to oversee their work.
And their views about their hospital have morphed to negativity based on four underlying beliefs:
Hospitals spend too much on overhead and executive salaries and not enough on direct patient care.
Hospitals are run poorly: we could run them better but they don’t listen to us.
Hospitals get rate increases from Medicare and physicians get screwed.
Hospitals need us more than we need them. But they don’t understand that.
On March 9, 2024, President Biden signed the Consolidated Appropriations Act, 2024, which included a 2.93% update to the CY 2024 Physician Fee Schedule (PFS) Conversion Factor (CF) for dates of service March 9 through December 31, 2024. But physicians saw that as not enough since their overhead increased even more. And for 2025, CMS is proposing to reduce average payment rates under the MPFS by2.93% compared to the average amount reimbursed for these services in CY 2024 based on CY 2025 MPFS conversion factor decrease of $0.93 (or 2.8%) from the current CY 2024 conversion factor.
Understandably, physicians are upset. They’re not delusional that private insurers will make up the difference nor imagining hospitals will divert funds their way from brick, stick and tech priorities. But they’re speaking out expressing their views to anyone who’ll listen.
For hospitals that employ physicians, the issue of their financial anxiety requires urgent attention–not as one of many alongside 340B, site neutral payments and others but as the one at the top of the list. The issue is not whether physician income relative to other professions and average households is high. The issue is about managing physician expectations about their livelihood realistically and practically while improving their clinical acumen as professionals.
The core beliefs held by employed physicians about their hospitals may not be fair, objective or accurate, but they’re no less deeply felt and impactful. Hospital boards and C suite leaders would be well-served to refresh plans accordingly.
On Wednesday, the Centers for Medicare & Medicaid Services (CMS) issued its proposed annual changes to physician payments in its 2025 Medicare Physician Fee Schedule Proposed Rule. Required by statute to maintain budget neutrality, CMS is proposing to reduce the conversion factor—which translates the cost of providing medical services into physician payments—by 2.8%.
This is expected to lower physician payments by 2.93% on average. The proposed rule also includes new telehealth flexibilities, changes allowing eligible accountable care organizations access to a quarterly advance on their earned savings, and new payments for providers that help patients at high risk of overdose or suicide.
The Gist: With CMS proposing to reduce physician payments for the fifth straight year, the American Medical Association and other physician groups are once again calling on Congress to avert these cuts.
Congress has previously responded with “Band-Aid” solutions to temporarily reduce or eliminate reductions for the next calendar year, but physician groups are demanding a more comprehensive fix that ties Medicare payment updates to the Medicare Economic Index, a measure of practice cost inflation.
Medicare physician pay has declined 20% relative to practice costs from 2000 to 2021, and post-COVID inflation has only worsened the issue. Although lawmakers on Capitol Hill have explored various means of doing so, structural changes to Medicare budgetary policy face an uphill legislative battle in a presidential election year.
A recent engagement with a health system executive team to discuss an underperforming service line uncovered a serious issue that’s becoming more common across the industry.
“Our providers are more productive than ever,” the CFO informed our team, “and yet we keep losing money on the service line.”
After digging into their physician compensation model, we came upon one source of the system’s issue. Because it was incentivizing physician RVUs equally across all payers, its providers responded, quite rationally, by picking up market share where growth was easiest: Medicaid patients, who weren’t generating any margin.
“We recognize that we’ve been employing these physicians as loss leaders in order to generate downstream revenue,” the CFO shared, “but what’s the point of that revenue if there’s no longer any downstream margin?”
The economics of physician employment becomes a tough conversation very quickly; it’s a sensitive topic to many, and one with myriad facets.
But the loss leader physician employment model obviously only works when it produces positive downstream margins.
We’re in a critical window of time, where hospital margins are just beginning to recover as volumes return—but those volumes are not necessarily in the same places as before.
The opportunity is ripe for systems to work closely with their aligned physicians to reexamine the post-pandemic margin picture for individual service lines and ensure incentives are aligning all parties to hit operating margin goals.
Are these kinds of conversations taking place at your health system?
Physicians at the American Medical Association Annual Meeting called for an overhaul of the Medicare payment system, arguing that it is outdated and threatens the survival of independent practices and patients’ access to care.
“This cannot wait; we are past the breaking point. Congress must urgently address physician concerns about Medicare to account for inflation and the post-pandemic economic reality facing practices nationwide,” AMA President Jack Resneck Jr., MD, said in a June 12 news release. “Our patients are counting on us to deliver the message that access to health care is jeopardized by Medicare’s payment system. Being mad isn’t enough. We will develop a campaign — targeted and grass roots — that will drive home our message.”
Inflation, the pandemic, declining reimbursements and rising cost are making it more challenging for independent physicians to maintain their autonomy and are jeopardizing access to care, according to the AMA, which argues that CMS physician payments have declined 26 percent from 2001 to 2023 after accounting for inflation.
In January, the Medicare Payment Advisory Commission called for a physician payment update tied to the Medicare Economic Index for the first time, and, in April, a group of House members introduced a bill that would provide annual inflation updates to the Medicare fee schedule based on the index.
“Duct-taping the widening cracks of a dilapidated payment system has put us in this precarious situation,” Dr. Resneck said. “Physicians are united in our determination to build a solid foundation rather than further jury-rigging the system.”
The Medicare Advisory Payment Commission recommends a higher-than-current-law fee-for-service payment update in 2024 for acute care hospitals and positive payment updates for clinicians paid under the physician fee schedule. It recommends reductions in base payment rates for skilled nursing facilities, home health agencies and inpatient rehabilitation facilities.
MedPAC gave Congress recommendations on payment rates in both traditional fee-for-service and Medicare Advantage for 2024, satisfying a legislative mandate comparing per enrollee spending in both programs.
MedPAC estimates that Medicare spends 6% more for MA enrollees than it would spend if those enrollees remained in fee-for-service Medicare.
In their March 2023 Report to the Congress: Medicare Payment Policy, commissioners said they were acutely aware of how providers’ financial status and patterns of Medicare spending varied in 2020 and 2021 due to COVID-19 and were also aware of higher and more volatile cost increases.
However, they’re statutorily charged to evaluate available data to assess whether Medicare payments are sufficient to support the efficient delivery of care and ensure access to care for Medicare’s beneficiaries, commissioners said.
FEE-FOR-SERVICE RATE RECOMMENDATIONS
MedPAC’s payment update recommendations are based on an assessment of payment adequacy, beneficiaries’ access to and use of care, the quality of the care, the supply of providers, and their access to capital, the report said. As well as higher payments for acute care hospitals and clinicians, MedPAC recommends positive rates for outpatient dialysis facilities.
It recommends providing additional resources to acute care hospitals and clinicians who furnish care to Medicare beneficiaries with low incomes. It also recommends a positive payment update in 2024 for hospice providers concurrent with wage adjusting and reducing the hospice aggregate Medicare payment cap by 20%.
It recommends negative updates, which are reductions in base payment rates, for skilled nursing facilities, home health agencies and inpatient rehabilitation facilities.
Acute care
For acute care hospitals paid under the inpatient prospective payment system, commissioners recommend adding $2 billion to current disproportionate share and uncompensated care payments and distributing the entire amount using a commission-developed “Medicare SafetyNet Index” to direct funding to those hospitals that provide care to large shares of low-income Medicare beneficiaries.
This recommendation got pushback from America’s Essential Hospitals.
“We appreciate the Medicare Payment Advisory Commission’s desire to define safety net hospitals for targeted support, but the commission’s Medicare safety net index (MSNI) could have the perverse effect of shifting resources away from hospitals that need support the most,” said SVP of Policy and Advocacy Beth Feldpush. “The MSNI methodology fails to account for all the nation’s safety net hospitals by overlooking uncompensated care and care provided to non-Medicare, low-income patients – especially Medicaid beneficiaries. Any practical definition of a safety net provider must consider the care of Medicaid and uninsured patients, yet the MSNI misses on both counts.”
Feldpush urged policymakers to develop a federal designation of safety net hospitals and to reject the MSNI.
“Further, policymaking for these hospitals should supplement, rather than redistribute, existing Medicare DSH funding, which reflects a congressionally sanctioned, well-established methodology,” she said.
Physicians and clinicians
For clinicians, the commission recommends that Medicare make targeted add-on payments of 15% to primary care clinicians and 5% to all other clinicians for physician fee schedule services provided to low-income Medicare beneficiaries.
The American Medical Association commended MedPAC, but also said that an update tied to just 50% of the Medicare Economic Index would cause physician payment to chronically fall even further behind increases in the cost of providing care. AMA president Dr. Jack Resneck Jr. urged Congress to pass legislation providing for an annual inflation-based payment update.
MedPAC has long championed a physician payment update tied to the Medicare Economic Index, Resneck said. Physicians have faced the cost of inflation, the COVID-19 pandemic and growing expenses to run medical practices, jeopardizing access to care, particularly in rural and underserved areas.
“Not only have Medicare payments failed to respond adequately, but physicians saw a 2% payment reduction for 2023, creating an additional challenge at a perilous moment,” Resneck said. “As one of the only Medicare providers without an inflationary payment update, physicians have waited a long time for this change. When adjusted for inflation, Medicare physician payment has effectively declined 26% from 2001 to 2023. These increasingly thin or negative operating margins disproportionately affect small, independent, and rural physician practices, as well as those treating low-income or other historically minoritized or marginalized patient communities. Our workforce is at risk just when the health of the nation depends on preserving access to care.”
The AMA and 134 other health organizations wrote to congressional leaders urging for a full inflation-based update to the Medicare Physician Fee Schedule.
MGMA’s SVP of Government Affairs Anders Gilberg said, “Today’s MedPAC report recommends Congress provide an inflationary update to the Medicare base payment rate for physician and other health professional services of 50% of the Medicare Economic Index (MEI), an estimated annual increase of 1.45% for 2024. In the best of times such a nominal increase would not cover annual medical practice cost increases. In the current inflationary environment, it is grossly insufficient.”
MGMA urged Congress to pass legislation to provide an annual inflationary update based on the full MEI.
Ambulatory surgical centers and long-term care hospitals
Previously, the commission considered an annual update recommendation for ambulatory surgical centers (ASCs). However, because Medicare does not require ASCs to submit data on the cost of treating beneficiaries, the commissioners said they had no new significant data to inform an ASC update recommendation for 2024.
Commissioners also previously considered an annual update recommendation for long-term care hospitals (LTCHs). But as the number of cases that qualify for payment under Medicare’s prospective payment system for LTCHs has fallen, they said they have become increasingly concerned about small sample sizes in the analyses of this sector.
“As a result, we will no longer provide an annual payment adequacy analysis for LTCHs but will continue to monitor that sector and provide periodic status reports,” they said in the report.
MEDICARE ADVANTAGE
Commissioners said that overall, indicators point to an increasingly robust MA program. In 2022, the MA program included over 5,200 plan options, enrolled about 29 million Medicare beneficiaries (49% of eligible beneficiaries), and paid MA plans $403 billion (not including Part D drug plan payments).
In 2023, the average Medicare beneficiary has a choice of 41 plans offered by an average of eight organizations. Further, the level of rebates that fund extra benefits reached a record high of about $2,350 per enrollee, on average.
Medicare payments for these extra benefits – which are not covered for beneficiaries in FFS – have more than doubled since 2018. For 2023, the average MA plan bid to provide Medicare Part A and Part B benefits was 17% less than FFS Medicare would be projected to spend for those enrollees.
However, the benefits from MA’s lower cost relative to FFS spending are shared exclusively by the companies sponsoring MA plans and MA enrollees (in the form of extra benefits). The taxpayers and FFS Medicare beneficiaries (who help fund the MA program through Part B premiums) do not realize any savings from MA plan efficiencies.
Medicare should not continue to overpay MA plans, MedPAC said. Over the past few years, the commission has made recommendations to address coding intensity, replace the quality bonus program and establish more equitable benchmarks, which are used to set plan payments, the report said. All of these would stem Medicare’s excess payments to MA plans, helping to preserve Medicare’s solvency and sustainability while maintaining beneficiary access to MA plans and the extra benefits they can provide.
PART D
Medicare’s cost-based reinsurance continues to be the largest and fastest growing component of Part D spending, totaling $52.4 billion, or about 55% of the total, according to the report.
As a result, the financial risk that plans bear, as well as their incentives to control costs, has declined markedly. The value of the average basic benefit that is paid to plans through the capitated direct subsidy has plummeted in recent years.
In 2023, direct subsidy payments averaged less than $2 per member per month, compared with payments of nearly $94 per member, per month, for reinsurance. To help address these issues, in 2020 the commission recommended substantial changes to Part D’s benefit design to limit enrollee out-of-pocket spending; realign plan and manufacturer incentives to help restore the role of risk-based, capitated payments; and eliminate features of the current program that distort market incentives.
In 2022, Congress passed the Inflation Reduction Act, which included numerous policies related to prescription drugs. One such provision is a redesign of the Part D benefit with many similarities to the commission’s recommended changes.
The changes adopted in the IRA will be implemented over the next several years, and are likely to alter the drug-pricing landscape, commissioners said.
Physicians are set to see a 4.5 percent decrease in Medicare payment next year, in part due to the expiration of a temporary payment boost that was passed by Congress in December 2021 to avert scheduled sequester cuts. Physician groups are expected to lobby lawmakers heavily in the final months of the year, hoping to secure a reprieve, especially as inflation and labor costs continue to rise.
Other changes in the 2023 rules include advance payments to new participants in the Medicare Shared Savings Program, intended to boost participation of providers in rural and underserved areas. Some pandemic-era telehealth flexibilities that are set to expire with the end of the federal COVID public health emergency were also extended.
The Gist: We do not expect the full Medicare physician reimbursement cut to physicians to go into effect, as a bipartisan group of Senators has already asked leadership to address it in the upcoming lame-duck session. However, the cut serves the important purpose ofrebasing negotiations between physician lobbies and Congress, such that keeping rates flat or obtaining a small boost would feel like a win for both groups—even if it falls far short of the rate increases needed to meet the rising cost of running a practice.
If Congress continues to intervene to push off or mitigate Medicare’s sequestration payment reductions, we could find ourselves back in a Sustainable Growth Rate (SGR)-type situation where a payment cut constantly looms, physicians continually lobby for yet another reprieve, and the delayed cuts balloon in size.
On July 7, 2022, the Centers for Medicare & Medicaid Services (CMS) released the 2023 Medicare Physician Fee Schedule (MPFS) proposed rule, which includes payment provisions and policy changes to the Quality Payment Program (QPP) and Alternative Payment Model (APM) participation options and requirements for 2023.
MPFS Key Proposals and Additional Potential Medicare Reductions:
For 2023, CMS proposes a Conversion Factor (CF) of $33.0775 which is a decrease of $1.53 or -4.42% from the 2022 conversion factor of 34.6062.
This significant reduction in the CF accounts for the expiration of the 3.00% increase in PFS payments for CY 2022 as required by the Protecting Medicare and American Farmers from Sequester Cuts Act, in addition to the statutorily required budget neutrality adjustment to account for changes in Relative Value Units.
The separately calculated Anesthesia CF is proposed at 20.7191, a -3.91% decrease from the 2022 conversion factor of $21.5623.
Key Takeaways: CMS estimates an impact to allowed charges from policy changes in the rule as outlined below. These impacts are due in part due changes in the RVUs and the second year of the transition to clinical labor pricing updates.
(Please note: These estimates do not include the impact on payments from the expiration of the congressionally mandated 3.00% boost to the 2022 CF.)
Anesthesiology: -1%
Diagnostic Radiology: -3%
Interventional Radiology: -4%
Emergency Medicine: +1%
Critical Care: +1%
Nuclear Medicine: -3%
Pathology: -1%
Radiation Oncology/Therapy Centers: -1%
Internal Medicine: +3%
Independent Laboratory -1%
Additional Potential Medicare Reductions:
In addition to the proposed cut to the CF, the second of two sequestration cuts was implemented on July 1, 2022, at -1%, bringing the total sequestration cut to -2% which will continue without Congressional intervention.
Also, the lack of full funding of the American Rescue Plan meant that the Medicare program would contribute 4% under the “PAYGO” (Pay as You Go) rules and that cut will come back into the Medicare fee schedule in 2023. In total, hospital-based physicians face in the approximate range of -10% in 2023 without Congressional intervention.
Appropriate Use Criteria (AUC): CMS did not address the appropriate use criteria (AUC)/clinical decision support (CDS) mandate for advanced diagnostic imaging services in this rule. CMS posted an update on its website indicating that the current educational and operations testing period will continue beyond January 1, 2023, even if the COVID-19 public health emergency (PHE) ends in 2022. The notice states that the agency is unable to forecast when the payment penalty phase of the program will begin. Read more at CMS.gov.
Additional highlights of the MPFS Proposed Rule include: Evaluations and Management (E/M) Services: As part of the ongoing updates to E/M visits and the related coding guidelines that are intended to reduce administrative burden, the AMA CPT Editorial Panel approved revised coding and updated guidelines for Other E/M visits, effective January 1, 2023.
Like the approach CMS finalized in the CY 2021 MPFS final rule for office/outpatient E/M visit coding and documentation, CMS is proposing to adopt most changes in coding and documentation for Other E/M visits including: hospital inpatient, hospital observation, emergency department, nursing facility, home or residence services, and cognitive impairment assessment, effective January 1, 2023. This revised coding and documentation framework would include CPT code definition changes (revisions to the Other E/M code descriptors), and for the first time would mean that AMA CPT and CMS would follow the same coding guidelines, including:
• New descriptor times (where relevant). • Revised interpretive guidelines for levels of medical decision making. • Choice of medical decision making or time to select code level (except for services such as emergency department visits (time has never been a component of ED E/M services except critical care) and cognitive impairment assessment, which are not timed services). • Eliminated use of history and exam to determine code level (instead there would be a requirement for a medically appropriate history and exam).
Split (or Shared) Visits (Where services are performed by advance practice clinicians.) CMS had previously finalized in the 2022 MPFS final rule a new January 1, 2023 billing policy for instances in which a physician delivers an E/M service along with an advanced practice clinician (APC). Recall that E/M services billed under an APC reimburse at 85% of the MPFS unless there is a documented shared service by the supervising physician.
• The key determinant for deciding if there was a shared service is if the physician provided key elements of the history, exam, or medical decision making ─ OR half of the total time spent treating the patient. • There were significant concerns that in hospital-based settings, the rule (set for implementation on January 1, 2023) would have required only time as the determinative element, and that the majority of APC services would then be reimbursed at 85% of the fee schedule. After significant advocacy by multiple stakeholders, CMS has delayed the policy that would have based the determination of the billing practitioner solely on time. This policy is proposed for delay until January 1, 2024 while CMS collects additional input.
Expand Telehealth Coverage: • CMS is proposing making several services that are temporarily available as telehealth services for the PHE available through CY 2023 on a Category III basis, which will allow more time for collection of data that could support their eventual inclusion as permanent additions to the Medicare telehealth services list. • CMS is also proposing to extend the duration of time that services are temporarily included on the telehealth services list during the PHE, but are not included on a Category I, II, or III basis for a period of 151 days following the end of the PHE, in alignment with the Consolidated Appropriations Act, 2022 (CAA, 2022).
Highlights of the Quality Payment Program (QPP): CMS stated they are limiting proposals for traditional MIPS and focusing on further refining implementation of MIPS Value Pathways (MVPs). 2023 Proposed Performance Threshold and Performance Category Weights: The performance threshold for the 2023 performance year is proposed to be 75 points, same as 2022. • Beginning with 2023, CMS will no longer offer an exceptional performance adjustment. • The category weights for the 2023 performance year are proposed to remain the same as the 2022 weights: o Quality – 30%, o Cost – 30% o Promoting interoperability – 25% o Improvement Activities – 15%
Data Completeness Requirements: • For 2023, CMS is proposing quality measure submissions should continue to account for at least 70% of total exam volume – same as 2022.
• CMS proposed to increase this threshold to 75% beginning with the 2024 and 2025 performance years.
Quality Category – Measure Scoring System • Beginning with 2023 CMS will change the scoring range for benchmarked measures to 1 to 10 points, doing away with the 3-point floor. • Score existing non-benchmarked measures at 0 points even if data completeness is met • New measures will continue to be scored at a minimum of 7 points for their first year and a minimum of 5 points in their second year. • CMS is maintaining the small practice bonus of 6 points that is included in the Quality • performance category score. • CMS also continues to award small practices 3 points for submitted quality measures that do not meet case minimum requirements or do not have a benchmark.
MIPS Value Pathways (MVPs) CMS is proposing 5 new MVPs and revising the 7 previously established MVPs that would be available beginning with the 2023 performance year. • Advancing Cancer Care • Optimal Care for Kidney Health • Optimal Care for Patients with Episodic Neurological Conditions • Supportive Care for Neurodegenerative Conditions • Promoting Wellness
Advanced Alternative Payment Models For payment years 2019 through 2024, Qualifying APM Participants (QPs) receive a 5 percent APM Incentive Payment. After performance year 2022, which correlates with payment year 2024, there is no further statutory authority for a 5 percent APM Incentive Payment for eligible clinicians who become QPs for a year.
CMS is concerned that the statutory incentive structure under the QPP beginning in the 2023 performance year. corresponding 2025 payment year, could lead to a drop in Advanced APM participation, and a corresponding increase in MIPS participation. As a result, CMS concluded that it would forego action for the 2023 performance period and 2025 payment year. They instead are seeking public input in identifying potential options for the 2024 performance period and 2026 payment year of the QPP.