Congress returns from its July 4 break today and its focus will be on the President: will he resign or tough it out through the election in 120 days. But not everyone is paying attention to this DC drama.
In fact, most are disgusted with the performance of the political system and looking for something better. Per Gallup, trust and confidence in the U.S. Congress is at an all-time low.
The same is true of the healthcare system:
69% think it’s fundamentally flawed and in need of systemic change vs. 7% who think otherwise (Keckley Poll). And 60% think it puts its profits above all else, laying the blame at all its major players—hospitals, insurers, physician, drug companies and their army of advisors and suppliers.
These feelings are strongly shared by its workforce, especially the caregivers and support personnel who service patient in hospital, clinic and long-term care facilities. Their ranks are growing, but their morale is sinking.
Career satisfaction among clinical professionals (nurses, physicians, dentists, counselors) is at all time low and burnout is at an all-time high.
Last Friday, the Bureau of Labor issued its June 2024 Jobs report. To no one’s surprise, job growth was steady (+206,000 for the month) –slightly ahead of its 3-month average (177,000) despite a stubborn inflation rate that’s hovered around 3.3% for 15 months. Healthcare providers accounted for 49,000 of those jobs–the biggest non-government industry employer.
But buried in the detail is a troubling finding: for hospital employment (NAICS 6221.3): productivity was up 5.9%, unit labor costs for the month were down 1.1% and hourly wages grew 4.8%–higher than other healthcare sectors.
For the 4.7 million rank and file directly employed in U.S. hospitals, these productivity gains are interpreted as harder work for less pay. Their wages have not kept pace with their performance improvements while executive pay seems unbridled.
Next weekend, the American Hospital Association will host its annual Leadership Summit in San Diego: 8 themes are its focus:
Building a More Flexible and Sustainable Workforce is among them. That’s appropriate and it’s urgent.
An optimistic view is that emergent technologies and AI will de-lever hospitals from their unmanageable labor cost spiral. Chief Human Resource Officers doubt it. Energizing and incentivizing technology-enabled self-care, expanding scope of practice opportunities for mid-level professionals and moving services out of hospitals are acknowledged keys, but guilds that protect licensing and professional training push back.
By contrast, the application of artificial intelligence to routine administrative tasks is more promising: reducing indirect costs (overhead) that accounts for a third of total spending is the biggest near-term opportunity and a welcome focus to payers and consumers.
Thus, most organizations advance workforce changes cautiously. That’s the first problem.
The second problem is this:
lack of a national healthcare workforce modernization strategy to secure, prepare and equip the health system to effectively perform. Section V of the Affordable Care Act (March 2010) authorized a national workforce commission to modernize the caregiver workforce. Due to funding, it was never implemented. It’s needed today more than ever. The roles of incentives, technologies, AI, data and clinical performance measurement were not considered in the workforce’ ACA charter: Today, they’re vital.
Transformational changes in how the healthcare workforce is composed, evaluated and funded needs fresh thinking and boldness. It must include input from new players and disavow sacred cows. It includes each organization’s stewardship and a national spotlight on modernization.
It’s easier to talk about healthcare’s workforce issues but It’s harder to fix them. That’s why incrementalism is the rule and transformational change just noise.
PS: In doing research for this report, I found wide variance in definitions and counts for the workforce. It may be as high as 24 million, and that does not include millions of unpaid caregivers. All the more reason to urgently address its modernization.
Companies demand employees come into the office for many legitimate reasons. But in some cases, it appears to be a tactic to force employees out.
Companies, large and small, are asking employees to return to the office at least a few days a week. But in some cases, these return-to-office (RTO) policies appear to be a passive-aggressive approach to eliminate roles, rather than doing layoffs.
Case in point: AT&T recently said it would require thousands of managers from across the country to work in person at just nine locations. One manager referred to the move as “a layoff wolf in return-to-office sheep’s clothing.”
While there are several reasons companies could be using RTO to avoid actively laying people off, Maurice Cayer, lecturer and coordinator of the master of science human resources program at the University of New Haven, said it could backfire.
“It’s a blunt instrument,” he said of the tactic.
A Disconnect Between Employers and Employees
Research from the University of Pittsburgh found companies use RTO mandates at times for “power grabbing and blaming employees for poor performance,” yet the results harm employee satisfaction and fail to improve performance.
Employees’ feelings about in-office work are clear. So why are companies choosing to enforce such an unpopular — and ineffective — tactic?
One reason is that some organizations, especially tech companies, overstaffed as they rebounded from the pandemic and now have too many employees, Cayer said. The introduction of new technology, like artificial intelligence, also might be behind a reduction in staff.
Others may be using RTO as a test. The mandate in those cases screens employees to determine “who’s the most committed to the organization” and open to a more traditional work model, said Colleen Flaherty Manchester, a professor in the Work and Organizations department at the University of Minnesota.
The tactic highlights the disconnect between employers’ perceptions of flexible work and employees’ desires to work remotely for personal or productivity reasons, she said.
Requiring employees to return to work in person may have some advantages, such as improved communication and more opportunities for mentorship, but organizations typically haven’t experienced extensive productivity issues with remote work, said Carrie Urrutia, a labor and employment attorney at Eastman & Smith in Toledo, Ohio.
“Many companies simply want things to revert to the way they were before COVID,” she said.
The Consequences of Using RTO to Trim Staff
Companies risk losing their best people with RTO policies, said Cayer.
“Organizations are placing bets, and they’re willing to live with the consequences of losing some highly desirable people in the process,” he explained. “But, maybe they’ll make up for it by having people who are engaged at work.”
Quietly laying off workers under the RTO guise could anger employees and damage an organization’s reputation, which might impact future hiring and meeting business goals, Urrutia added.
Yet the approach is attractive to companies. “It could be a less-costly way to achieve a goal of reducing the workforce without a formal reduction in force,” said Urrutia.
Employees who quit as a result of RTO mandates wouldn’t be eligible for unemployment compensation and typically wouldn’t receive a severance package as opposed to those who were laid off, she explained. “Generally speaking, employees who voluntarily resign are not entitled to those benefits.”
However companies would be better served implementing hiring freezes or enabling more flexibility, she argued. Urrutia said organizations should examine their current remote or hybird work arrangements and assess what’s working for them and employees. If RTO is mandated, they should clearly articulate the business reasons why it’s necessary and why remote work isn’t working.
“Aim to find a sweet spot that achieves the manager’s goals of in-person connection for innovation and group productivity, yet also meets some of the needs of employees,” Manchester said.
Are Quiet Layoffs Legal?
As a rule, employees don’t have a legal right to work from home, so employers are free to require in-person work as a condition of employment, Urrutia said. Workers therefore typically don’t have legal recourse if they feel a RTO mandate is designed to make them quit.
One exception is if an employee had a contract that specifically stipulated they’re allowed to work remotely, Urrutia explained. Another is unionized employees, where RTO could be a subject of collective bargaining.
Organizations also must ensure their RTO decisions aren’t discriminatory or unfairly impact groups protected under the Civil Rights Act,Cayer said. The law prohibits employment discrimination based on race, color, sex, national origin, age, disability and medical history.
Employers are also required to provide reasonable accommodation under the Americans with Disabilities Act or Pregnant Workers Fairness Act, and that might include allowing remote work, Urrutia added.
“Employees who work from home are not a protected classification, but many employees who work from home are in protected classifications,” she said.
Still, employees could file a lawsuit if they feel they RTO policies unfairly led them to quit, Cayer added. Organizations can choose to protest the suit. “A lot of times that leads into some settlement,” he said.
As finance departments undergo seismic tech-driven changes, controllers are poised to play a crucial role as the CFOs’ right hand.
Today’s finance chiefs are making strategic decisions and driving digital transformation, but to execute their changing roles successfully, they need to be supported by an equally resilient, adaptive team.
New technologies, ways of working and shifting business needs are impacting the day-to-day roles not just of the CFO, but of other crucial financial executives as “at the highest level, the entire finance organization is [undergoing] a seismic shift in ways that they haven’t seen ever,” said Sanjay Sehgal, advisory head of markets for Big Four accounting firm KPMG.
Taking a look at the evolving new responsibilities that controllers — as well as other staff in finance departments — must embrace will be crucial for finance chiefs who must build modern finance teams capable of tackling the upcoming challenges of 2024.
Trusted advisor
The controller “is really becoming and has become the trusted advisor to the CFO,” Sehgal said in an interview.
As with many jobs, the role can vary depending on the company. But generally controllers oversee their company’s daily accounting operations, along with payroll and the accounts payable and receivable departments, according to human resource consulting firm Robert Half. It can also entail preparing internal and external records, handling the firm’s general ledger and taxes as well as reconciling accounts, coordinating audits and managing budgets.
Already, the importance of the controller position is reflected in compensation trends: the role ranks among the most well-paid members of the finance team, with corporate controllers in the 75th percentile — meaning they take home salaries greater than three-quarter of financial professionals — in compensation earning annual average salaries around $210,750, according to data from human resource consulting firm Robert Half.
Controllers rank among top paid financial professionals
Starting salaries for corporate accounting executives in the 75th percentile
Central to the role too is the responsibility controllers take for their company’s close activities, ensuring the business is “producing information in a controlled fashion, to report to the street and to the Securities and Exchange Commission for a public company,” said Kevin McBride, corporate controller and chief accounting officer for software-as-a-service company ServiceNow.
In his capacity as controller for the Santa Clara, California-based SaaS company, McBride oversees global payroll, accounts payable, travel, collections, and credit, he said in an interview. The role of controller and chief accounting officer can also have some overlap, but don’t need to be combined; a CAO can be another name for a principal accounting officer as required under the Sarbanes-Oxley Act, for example, McBride said. A CAO typically focuses on more broad corporate governance, therefore, while a controller’s focus is more narrowly on processes such as the close and ensuring financial statements are compliant with GAAP.
Controllership is “really getting to the numbers and the descriptors and the story behind financial performance and ensuring that process is well-controlled,” McBride said. Joining ServiceNow in November 2021, he previously logged a 21-year tenure at tech giant Intel, where he served in a variety of key financial roles including as its vice president of finance and corporate controller as well as its global accounting and financial services controller. He also spent time at the Financial Accounting Standards Board as an industry fellow before joining Intel.
Opening a path to the touchless close
In recent years, however, controllers have also found themselves branching out from a pure numbers function as part of the ongoing “seismic shift” taking place in the whole of finance — driven partly by the advent of generative AI, machine learning, cloud technologies and other digital tools which have captivated the attention of finance leaders in recent months, Sehgal said.
New technologies such as GenAI could fundamentally change how controllers operate and the purpose of the role — for example, “I can see a future where we have a touchless close process,” Sehgal said.
This would mean the entire financial close process would no longer need routine manual intervention by such people as the controller, according to a 2022 report by Gartner which noted 55% of finance executives were targeting a touchless close by 2025.
Finance teams could inch closer to making such a process a reality in 2024 as companies continue to experiment with the applications of generative AI, something that could rapidly shift where today’s controllers are directing their time and focus.
The new technologies that have filtered into accounting over the past few decades have enabled their own improvements in quality, efficiency and cost, McBride said, allowing business leaders to get the information they need to run the business at a lower cost. When it comes to the controllership, “it also gives us capacity to invest in other ways to help drive business impact,” he said.
However, it’s also important to remember that technology is “nothing new in accounting,” McBride — who started his career working on paper spreadsheets — said and that in “each one of these technology introductions, there’s the hype and then there’s the reality,” he said. Generative AI and the promise it brings remains in its early stages, he said.
As automation seeps into finance, technology opens up more time by removing routine tasks, in turn enabling the controller and the CFO to deepen their relationship. “With the CFO, we’re spending more time talking about strategic matters and how to best position not just the controllership but finance,” McBride said.
The evolution of the relationship comes as CFOs are likewise pivoting to a role more focused on driving strategy and controllers are finding themselves responsible for processes that may previously have been under the remit of the finance chief.
“As the CFO elevates himself or herself, I think the controller plays a bigger role in the organization,” Sehgal said.
Finance chiefs are serving more and more often as the “right hand” of the CEO and spending less time poring over day-to-day numbers, said Claire Bramley, CFO of San Diego, California-based AI cloud analytics and data platform Teradata. The controller and the CFO work closely together to drive an effective, innovative and forward-looking finance function, but that focus on day-to-day operations is what separates the two positions, Bramley said in an interview.
As a finance chief, “you need to make sure that you’ve got the processes in place, you understand what’s going on,” she said. However, the finance chief is now spending more time figuring out how to drive things forward at the company, she said.
Adding free cash flow forecasts
Bramley pointed to something like free cash flow as an example: because she’s now spending more time conducting strategy transformation work on part of Teradata, she’s now relying on her controller to take on free cash flow management forecasting, she said.
Controllers, critically, still serve as “the owners of the financial data, from a protocols perspective, from a reporting perspective, and the CFO and the executive teams depend on that,” Sehgal said. Indeed, taking responsibility for the numbers is still the core of the controller’s role, McBride agreed.
However, controllers are not immune to the job creep plaguing the financial function amid a lack of qualified accounting talent, emerging technologies and new business needs. As the CFO’s role evolves into a more strategic position, the rest of finance could potentially be pulled along in their wake.
“It’s very easy for a controller to be kind of put off to one side … and not be pulled into, I’ll say some of the business and strategic decisions,” Bramley said. “But if you decide as a controller that you want to be more involved in that, I think many companies give you the opportunity to build your business acumen, to build your business relationships and to be able to be an important part of managing the business.”
For example, the controller today has a huge opportunity to take point on digital transformation at a business — the controller organization tends to be the biggest team in the finance function, “so if they can drive [digital transformation], and they can be leading edge, then the rest of finance can adopt that moving forward,” Bramley said.
This can also provide a pathway to controllers to the CFO seat — Bramley spent two years serving as the global controller for HP, where she logged a 14-year tenure before making the jump to Teradata.
“The modern-day controller who is involved in strategic decision making, who is helping add business value, who is having an impact from a technology standpoint, I think, is an obvious candidate for a CFO,” she said.
Companies are turning to interim financial leadership more frequently as they struggle to fill widening gaps in their accounting and finance functions.
Dive Brief:
Demand for interim financial leadership skyrocketed last year, with requests for interim CFOs jumping by 46%, according to a report by Business Talent Group, a Heidrick & Struggles company.
As well as interim CFO leadership, requests for on-demand talent with skills in key areas of finance also jumped; requests for talent that’s skilled in audit, accounting and financial controls have increased 33%, while those for FP&A and modeling skills increased 28%, the report found.
The rise in demand for audit, accounting and similar skills is “a logical consequence of the declining pipeline of accounting majors and CPA candidates,” Jack Castonguay, an assistant professor of accounting at New York’s Hofstra University, said in an email.
Dive Insight:
Competition to nab skilled accounting talent has only become fiercer in recent years amid a worsening shortage of accounting professionals, leaving companies with critical gaps in their financial leadership and function.
In addition to surging demand for interim CFOs, requests for senior vice president or vice president-level financial professionals — such as controllers and the heads of financial planning & analysis — rose by 114%, according to BTG.
When it comes to roles such as the head of FP&A or controllers, for example, “I think as you have shortages on one end, you’re going to have demand with organizations, whether it be full time or on-demand, for talent coming in,” Sunny Ackerman, global managing partner for on-demand talent at Heidrick & Struggles said in an interview. Ackerman does believe there is a link between the shortage in talent and the spike in requests for on-demand employees in these areas, she said. “So I think there is definitely a correlation for that.”
Historically, many companies have looked to fill roles in FP&A, audit, financial reporting and up to the CFO or controller chair with employees that have previously worked for an accounting firm, but dynamics have changed in recent years where many roles in accounting are now outsourced, Castonguay said.
“With accounting firm dynamics, largely insufficient salaries and work-life balance leaving firms struggling to attract people to the profession, the companies needing these people are now logically also struggling,” he said in an email. “You cannot disconnect the two.”
The narrower pipeline of new accounting graduates plus a high rate of retirement in the industry can leave the employees that are left overworked, increasing the likelihood of mistakes, according to a report by Fortune.
“Significant attrition” in the accounting department for retail brand Tupperware contributed to a delay in the company’s ability to file its annual 10-K form on time with the Securities and Exchange Commission, for example, the second consecutive year the brand will be filing late.
“Fewer grads lead to fewer public accountants which leads to fewer qualified and experienced hires for companies to place in their internal accounting-focused roles,” Castonguay said. “The dynamic makes me wonder how the temporary or outsourced staffing firms are finding candidates at their staffing firms. It’s possible that will be the next shoe to drop.”
On the labor side, changing ways of working may also be impacting how employees want to work; while there may be shortages in certain areas, the company is not necessarily seeing a slowdown of new candidates joining their platform, Ackerman said.
“So I think, even though there’s shortages in certain areas, I think talent is looking at this way of working differently than they did five years ago, and more companies are engaging with it,” she said.
Companies may also be more motivated to try out on-demand talent as they look to plug critical skill gaps in their workforces. Ninety-five percent of executives said they anticipate difficulty finding the “ideal combination of skills, capacity and expertise” inside their teams, BTG’s report said.
Today’s companies “now are starting to really open up and look at how they can blend full time talent with more independent talent and tapping into those capabilities at the desired time,” Ackerman said.
That includes how they might be approaching interim leadership; many firms are looking for on-demand talent to help provide critical support for larger-scale projects or initiatives, according to BTG, a category that makes up 27% of all talent requests.
Interim leadership can provide benefits to companies who are in transition or who are undertaking major changes, according to a 2023 CFO Dive report citing BTG data from that year.
An interim controller, for example, could take point on business process optimization for the business to successfully execute such a project; “the CFO or that finance function is quite a bit of a right hand, I would say to the executive suite,” Ackerman said.
CFOs and finance department recruiters have faced a workforce problem for years now, labor experts say: a shrinking pool of U.S. accounting professionals needed to close the books every quarter, complete audits, and make sure the company’s financials comply with GAAP and other regulations.
The hits that have chipped away at accounting labor health are myriad and the statistics stark. While the number of practicing accountants and auditors in the U.S. spiked in 2019, across the past decade since 2013 the total declined by about 10% to 1.62 million last year, with roughly 190,000 jobs disappearing from the work rolls, according to the Bureau of Labor Statistics.
Meanwhile, the total number of test takers who passed the CPA Exam fell to 18,847 in 2022 from 19,544 the year earlier, and the lowest level since 2007, according to the latest numbers available from the Association of International Certified Professional Accountants.
Studies and those analyzing the trend point to a variety of likely culprits: the onerous 150 hours of course credit — equivalent to a fifth year of college — students typically need to become a CPA, generally lower starting salaries compared to other areas of finance, and the demanding hours and rising regulations that lead some practicing accountants to look for the exits once they’re in the field. At the same time, the launch of the generative AI tool ChatGPT in late 2022 led to a new wave of questions about the industry’s future.
Tom Hood, executive vice president of business engagement and growth at the AICPA, is in the optimistic camp of those who believe the pipeline decline is poised to turn around, noting that he has seen other cycles when disruptive shocks such as Microsoft’s Excel in the 1980s damped interest and sparked doomsday talk around the possible “end of accounting.”
“We’ve had ebbs and flows, we’ve had these shortages before and every time that’s happened we as a profession have rallied together,” said Hood, a CPA, adding that AI will automate certain tasks in accounting but will not replace accountants. “We’ve moved this needle before and I think we’re already starting to see it move now.”
In 2024 professional associations and lawmakers are working on numerous initiatives as well as legislation to close the cracks that have leaked talent from the field. In the meantime, companies have found ways to get the staff needed to get their finance work done. CFO Dive talked to experts about some notable tactics that are likely to shape the accounting workforce this year.
States, CPAs and the 150-hour credit question
Currently state regulatory bodies that set the rules require those who want to to become a Certified Public Accountant to have 150 credit hours of education in accounting or related subjects to become a licensed CPA. But amid the growing shortage, there has been a controversial push by states to create another pathway to licensure which include cutting the college credit hour requirement back to 120 hours.
For example, this year Minnesota lawmakers are expected to consider new legislation introduced in the state’s Senate and House in 2023 that would allow candidates to earn a CPA certificate with only 120 hours of college credit, along with passing the CPA exam and some additional work experience or professional education. This alternative would be in addition to the current system that requires 150 hours and one year of work experience, plus passing the CPA exam.
Geno Fragnito, director of government relations for the Minnesota Society of CPAs that supports the change, notes that the current national shift to the 150 rule gained steam in the 1980s after Florida made the change amid a surplus of accountants due to many wanting to move to the state. Florida started the ball rolling by increasing the credit hour requirement to 150 hours in 1983, according to a Journal of Accountancy report.
But in recent years, the MNCPA’s members have consistently pinpointed the credit requirement as one of the main contributors to the drop in CPAs.
“I don’t think there was a meeting that either our CEO or I attended where it was not brought up organically. It was never on our agenda to discuss but it always came up,” Fragnito said. Looking ahead, Fragnito said that other states that are seeking to tweak the credit hour formula include South Carolina and Washington state.
A “volatile year” for CPA exam takers
Two exam-related changes are impacting accounting candidates this year in very different ways. “It’s an exciting time but I think 2024 will be a very volatile year,” Mike Decker, vice president of the CPA Examination & Pipeline Extension for AICPA, said in a recent interview. One of the changes is student-friendly: it’s designed to ease deadline pressures and address pandemic-related delays that might have affected some test takers. In a move announced last spring, the National Association of State Boards of Accountancy extended the window that a candidate has to complete the exam once they pass the first section from 18 months to 30 months. The move grew out of the AICPA’s effort to address the accounting shortage, known as its pipeline acceleration plan.
Meanwhile, this month marked the launch of a revamped CPA Exam called the CPA Evolution. The test has both new content and structure and a greater focus on technology in an effort to combat research that found that accounting firms were hiring fewer accountants in favor of non-accountants with tech backgrounds, according to a Nov. 7 report by Michael Potenza of Becker. “It’s not that CPA Evolution is meant to be harder than the previous version of the exam, it’s simply meant to better prepare you for the skills and competencies needed in modern accounting,” Potenza, a CPA, wrote.
Raises and remote work
Tactics that CFOs themselves are using to meet their staff needs include sweetened offers and going offshore or considering remote workers to gain talent. With most small and medium-size CPA firms unable to find enough qualified U.S. accountants, this summer a study found that over half of firms planned to hike starting salaries by 14%, CFO Dive previously reported. Lisa Simpson, vice president of firm services at AICPA, is hearing about similar approaches taken by firm leaders she’s spoken with. In the past few years, she said, firm leaders indicated they were providing several high percentage salary increases for new hires and existing employees. Last year firms gave raises at rates above inflation as well as continuing bonuses, and business leaders said they expect to continue raises into 2024.
Meanwhile, many firms are outsourcing U.S. accounting work to professionals in India, the Philippines, and Eastern European countries like Poland, according to Matt Wood, head of global FAO Services at Austin, Texas-based Personiv, a global outsourcing provider which serves those needs. While outsourcing to other companies was previously the domain of larger firms, the pandemic has led to more companies being comfortable with remote accounting staff, he said.
The shift to hiring accounting staff outside the U.S. “has been happening for a while now, but it really accelerated in 2020. The accounting talent pool was already shrinking, and businesses were feeling the impact of that pre-pandemic. Then, all of these other pieces fell into place; teams were working remotely and protecting cashflow took priority,” Wood said in an emailed response to questions from CFO Dive.
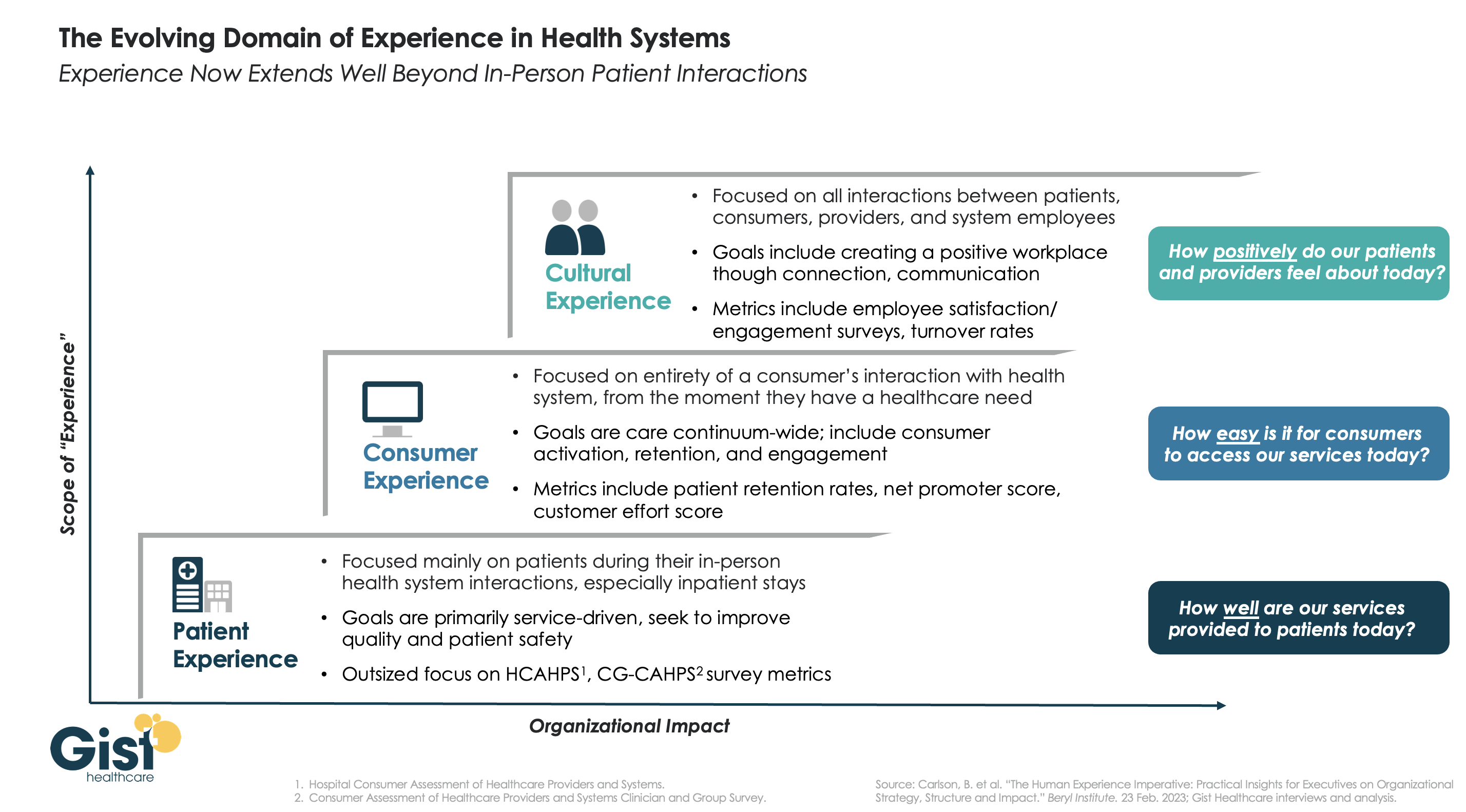
In this week’s graphic, we highlight the importance of broadening the domain of health system experience initiatives beyond patients to include consumers and even employees.
While reimbursements tied to HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and CG-CAHPS (Clinician and Group Consumer Assessment of Healthcare Providers and Systems) scores have made patient experience a main focus for years, an increasingly consumer-driven healthcare industry means that health systems must consider the experience of all consumers in their markets, with the hopes of meeting their needs and eventually welcoming them as new—or retuning—patients.
Embracing this mindset requires focusing on the entirety of a consumer’s interactions with the health system and the tracking of non-traditional metrics that measure the strength and value of their relationship to the system. Some systems are expanding their experience purview even further by also focusing on the working conditions and morale of their providers and other staff, as a healthy workplace environment serves to better both the patient and consumer experience. Easily accessible services and positive interactions with providers and other staff can determine a consumer’s view of their experience before any care is actually delivered.
Cultural and strategic shifts that integrate experience from the top down into all operational facets of the health system will ultimately strengthen consumer loyalty, employee retention, and the financial health of the system.
The upheaval of the past few years has permanently changed the healthcare landscape, and while many sectors of the industry continue to endure financial hardship, there is reason for cautious optimism in 2024 as healthcare begins to see a return on investment in technology and a resurgence in dealmaking.
This year, BDO surveyed healthcare CFOs to discover their plans, priorities, and concerns heading into 2024.
In today’s newsletter, I’ve outlined the top research findings that every healthcare leader needs to know to prepare for the year ahead.
Top 3 Workforce Investment Areas
Clinician burnout and staffing shortages remain challenging in the healthcare industry, but BDO’s survey indicated that many CFOs are bullish that the worst is behind them, with 47% stating they feel that in 2024, the talent shortage will represent less of a risk than in 2023.
Investment in the workforce is crucial to addressing staffing challenges, and in the year ahead, healthcare CFOs intend to invest in the following ways:
1. Training: 48% of CFOs plan to spend more on training, in part to buttress ongoing investment in new technologies like AI that can help with predictive staffing and financial reporting.
2. Recruitment: 48% of CFOs will spend more on recruiting, as the talent shortfall tightens an already restricted pool of candidates.
3. Compensation & Benefits: Alongside greater spending on recruiting itself, 46% of CFOs intend to increase compensation and benefits as a means of attracting talent from competitors and retaining current staff.
Transaction Plans
Dealmaking turned a corner in 2023, with activity returning to pre-pandemic levels in Q2. Despite fluctuating interest rates and the volatility of an election year, we can expect more transactions in 2024, with 72% of CFOs planning some kind of deal, relative to their organization’s financial health and liquidity. An increase in antitrust activity, however, could impact the size and type of deals that see success. Healthcare CFOs planning a large deal should be prepared for heightened scrutiny.
While we expect to see a wide range of deals taking place over the next year, two specific deal types are worth calling out:
1. Carve-outs/Divestitures: We may see an uptick in enterprise sales, carve-outs, and divestitures, particularly for institutions that have been struggling financially — 31% of institutions that violated their bond or loan covenants in 2023 are planning to pursue deals of this kind.
2. Private Equity (PE) and Venture Capital (VC): Nearly one in five (19%) CFOs, particularly those working with physician groups, plan to explore PE and VC investment as avenues toward scaling, sharing services, and safeguarding succession planning.
Service Line Investment Plans
There are still many areas where CFOs are intending to increase investment, but changed market conditions mean that some core areas of healthcare may see decreased investment as the industry realigns:
1. Specialty Services: Fifty-two percent of CFOs plan to increase their investments in specialty services like cardiology, oncology, and dermatology, while 23% of CFOs intend to partner with a capital provider or operator.
2. Service Expansion: Home care (51%), virtual/telehealth (48%), and ambulatory service centers (49%) are also priority areas for investment as institutions continue to expand and maintain access to healthcare outside of traditional hospital and clinic settings.
3. Primary Care: Although primary care remains at the heart of the healthcare industry, many CFOs (42%) have in fact signaled an intent to reduce investment in this area, reassessing their primary care strategies due to significant cash flow pressures and ongoing realignment as the retail market gains ground.
Want to know more about healthcare leaders’ plans for the year ahead? Get more insights and data in BDO’s 2024 Healthcare CFO Outlook Survey.
Where are you planning on increasing investment in your organization this year? Let me know in the comments below.