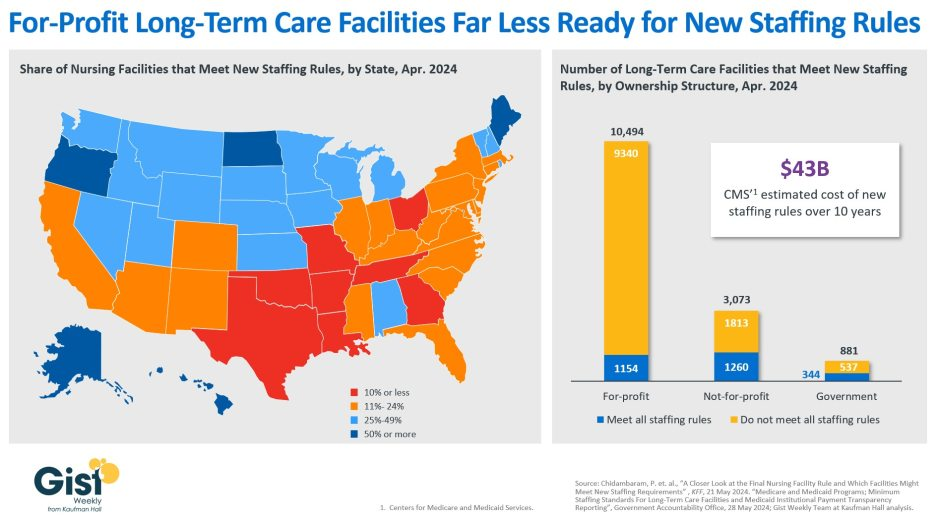
In late April, the Centers for Medicare & Medicaid Services (CMS) establishednew staffing standards for long-term care (LTC) facilities, mandating a minimum of 3.48 hours of nursing care per patient per day, with 33 minutes of that care from a registered nurse, at least one of whom must be always on site. The rule is slated to go into effect in two years for urban nursing homes and three years for rural nursing homes, with some facilities able to apply for hardship exemptions.
Although about one in five LTC facilities nationwide currently meet these staffing standards, staffing levels vary greatly by both state and facility ownership profile. In 28 states, fewer than a quarter of LTC facilities meet the new standards, and in eight states fewer than 10% of facilities are already in compliance.
Facilities in Texas are the least ready, with only 4% meeting the new staffing minimums. In terms of ownership structure, only 11% of for-profit facilities—which constitute nearly three quarters of all LTC facilities nationwide—have staffing levels that meet the new staffing minimums.
The Government Accountability Office projects this new rule will cost LTC facilities $43B over the first ten years, a significant expense at a time when recruiting and retaining nursing talent is already challenging.
Citing the risk of mass closures from facilities unable to comply, nursing home trade groups are suing to stop the mandate from going into effect, and there is also a bill advancing in the House that would repeal the staffing ratios.
That bill is backed by the American Hospital Association, which fears the mandate “would have serious negative, unintended consequences, not only for nursing home patients and facilities, but the entire health continuum.”
Hospitals in California are being warned not to violate state law on staffing levels or face fines. New state policy narrows the circumstances under which hospitals can claim “unpredictable circumstances” for violating the mandate.
The California Department of Public Health this week, in a notice to hospitals, warned that noncompliance can result in a $15,000 fine for a first violation and $30,000 for a second.
The state conducts periodic, unannounced inspections to enforce compliance.
New policy by Governor Newsom narrows the circumstances under which hospitals will not be penalized for violations due to “unpredictable circumstances,” requiring them to document efforts to maintain safe staffing and that such instances be truly unforeseen.
In an advisory letter to hospitals, the public health department said, “Situations that are not considered unpredictable, unknown or uncontrollable include consistent, ongoing patterns of understaffing. Facilities are expected to maintain required nurse-to-patient ratios at all times, including but not limited to, weekends, holidays, leaves of absences, among others.”
WHY THIS MATTERS
Minimum staffing ratios have been law in California since nurses and healthcare workers fought to pass AB 394, the nation’s first nurse-patient staffing ratio law in 1999.
In addition, SB 227, which passed in 2019, requires the state to assess administrative fines on hospitals that violate the safe staffing law. Law AB 1422 requires public comment before the public health department grants waivers to the critical care program flexibility requests.
THE LARGER TREND
Nurse staffing ratios are controversial and California remains the only state to have enacted them.
A study reportedly commissioned by the Centers for Medicare and Medicaid Services said there was “no single staffing level that would guarantee quality care.”
The NIH looked at survey data from 22,336 hospital staff nurses in California, Pennsylvania and New Jersey in 2006 and state hospital discharge databases. California hospital nurses cared for one less patient on average than nurses in the other states and two fewer patients in medical and surgical units, the NIH research said.
The study found that lower ratios were associated with significantly lower mortality. When nurses’ workloads were in line with California-mandated ratios in all three states, nurses’ burnout and job dissatisfaction were lower, and nurses reported consistently better quality of care, the NIH said.
Also, the hospital nurse staffing ratios in California were associated with better nurse retention than in the other states.
ON THE RECORD
“Patients in California are safer today because nurses and healthcare workers demanded that hospitals be held accountable for violating safe-staffing laws,” said Leo Pérez, RN and president of SEIU 121RN. “The COVID-19 pandemic taught us that our state’s health depends on supporting and listening to those who are on the front lines of patient care – a lesson we should never forget. Today’s action is the result of SEIU’s relentless vigilance. We applaud the step CDPH has taken to enforce laws that keep patients safe.”
The latest piece in the New York Times ’“Profits over Patients” series focuses on the staffing policies of Ascension, one of the nation’s largest nonprofit health systems, drawing a straight line from its cost-cutting practices over the last decade to its current staffing woes. Like previous articles in the series, the piece hones in on Ascension’s profit-seeking motives, pairing pre-pandemic accounts of Ascension executives boasting about savings from slashed labor costs with story after story of its frontline clinicians struggling to provide adequate patient care once COVID hit.
In responses included in the article, an Ascension spokesperson rejected the idea that the system’s workforce policies were responsible for its current staffing crisis, claiming that Ascension has maintained better staff-to-patient ratios than many of its peers.
The Gist: Yet again, the New York Times is shining a harsh light on a health system that has been engaged in management practices common across the industry.
While the piece omits some relevant information, such as the recent spike in labor costs, it’s useful to point out that many hospitals were so thinly staffed prior to COVID that they had virtually no slack in their labor pools, hindering their response to the crisis.
In our experience, the reasons for this have less to do with lining executives’ pockets, and more to do with the realities of dealing with a worsening payer mix and rising input costs. While future hospital workforce strategy is going to have to focus on reducing dependency on nurses—especially in the inpatient setting—any effort to that end must augment nurses with team-based care models and technology solutions, rather than pushing further on already-tight nurse-to-patient ratios.
An ICU nurse helps to prepare medicine for a covid patient in St. Cloud, Minn. Nurses in the state are planning to go on a three-day strike starting Sept. 12.
About 15,000 nurses in Minnesota walked off the job Monday to protest understaffing and overwork — marking the largest strike of private-sector nurses in U.S. history.
Slated to last three days, the strike spotlights nationwide nursing shortages exacerbated by the coronavirus pandemic that often result in patients not receiving adequate care. Tensions remain high between nurses and health-care administrators across the country, and there are signs that work stoppages could spread to other states.
Minnesota nurses charge that some units go without a lead nurse on duty and that nurses fresh out of school are delegated assignments typically held by more experienced nurses, across some 16 hospitals where strikes are expected.
The nurses are demanding a role in staffing plans, changes to shift scheduling practices and higher wages.
“I can’t give my patients the care they deserve,” said Chris Rubesch, the vice president of the Minnesota Nurses Association and a nurse at Essentia Health in Duluth. “Call lights go unanswered. Patients should only be waiting for a few seconds or minutes if they’ve soiled themselves or their oxygen came unplugged or they need to go to the bathroom, but that can take 10 minutes or more. Those are things that can’t wait.”
Paul Omodt, a spokesman for the Twin Cities Hospital Group, which represents four hospital systems where nurses are striking in the Minneapolis-St. Paul area, said that the nurses union did not do everything it could to avoid a strike.
“Nurses have steadfastly refused to go to mediation,” Omodt said. “Their choice is to strike. This strike is on the nurses.”
Conny Bergerson, a spokeswoman for Allina Health, another hospital system in the Twin Cities where nurses are on strike, said “rushing to a strike before exhausting all options such as engaging a neutral federal mediator does not benefit our employees, patients or the communities we serve.”
The Minnesota Nurses Association, the nurses union, said hospital administrators have continued to “refuse solutions” on understaffing and safety in contract negotiations. It said nurses have increasingly been asked to take on more patients for bedside care to make up for labor shortages, exacerbating burnout and high turnover.
Some hospitals have offered increased safety protocols for reporting security incidents in negotiations, but have not budged on other safety- and staffing-related demands.
The union has proposed new mechanisms for nurses to have a stronger say in how wards are staffed, including a committee made up of nurses and management at each hospital that would determine appropriate staffing levels. It has also proposed protections against retaliation for nurses who report understaffing. Striking nurses at some hospitals said their shifts are often short five to 10 nurses, forcing nurses to take on more patients than they can handle.
Omodt said that while there was a rise in understaffing reports during the height of covid, conditions have improved, and nurses have made contradictory claims when it comes to staffing at their hospitals since then.
In the lead-up to the strike, Minnesota hospital groups filed unfair labor practices charges against the union for refusing to go to mediation, and asked the National Labor Relations Board to block the strike for a failure to provide enough notice. The NLRB has thrown out at least some of those charges.
Hospitals facing strikes have been recruiting traveling nurses from across the region and plan to maintain staffing levels during the strike, though they are preparing for reduced operations, according to some of the hospital groups facing strike activity.
For years, hospitals in the United States have faced understaffing problems. A surge in demand and increased safety risks for nurses during the pandemic accelerated those trends. The number of health-care workers in the United States has still not recovered to its pre-pandemic levels, down 37,000 workers compared with February 2020.
At the same time, demand for health-care services has steadily increased during the pandemic, with a backlog of people who delayed care now seeking medical attention. During the covid wave that swept across the United States this summer, states such as New York and Florida reported the worst nursing shortages in decades. Research shows that patients are more likely to die because of preventable reasons when health-care providers are overworked.
Nurses, who risked their lives during the pandemic, are quitting and retiring early in droves, because of increased workloads caused by short staffing and demanding schedules that make finding child care and having a life outside of work exceedingly difficult. The understaffing crisis is pronounced in Minnesota in part because of its aging population and its record low unemployment rate.
There are some signs that nurse- and other health-care-worker strikes could spill over to other states in the coming weeks. Four thousand nurses with the Michigan Nurses Association voted earlier this month to authorize a strike related to understaffing concerns, and 7,000 health-care workers in Oregon have also authorized a work stoppage. University of Wisconsin nurses narrowly averted a strike this week. Therapists and clinicians in Hawaii and California are currently in the fourth week of what has become the longest-running mental health care strike, over inadequate staffing levels.
In Minnesota, the Minnesota Nurses Association recorded a 300 percent increase in nurses’ reports of unsafe staffing levels on their shifts since 2014, up to 7,857 reports in 2021.
Kelley Anaas, 37, a nurse who works in the ICU at Abbott Northwestern in Minneapolis said nurses in her unit have been forced to double up on patient assignments and work with lead nurses who have less than a year of experience.
“It eats away at you. If that was my family member in that bed, I wouldn’t want to leave their side,” said Anaas, adding that her workload has increased steadily over her 14 years at Abbott Northwestern.
While the nurses say their main impetus for striking is staffing levels and not pay, they are also at odds with hospitals over wages. The Minnesota Nurses Association has proposed a 30 percent pay increase over the next three years, noting inflation is at a 40-year high, while health-care groups have proposed a pay increase of 10 to 12 percent.
“The union’s wage demands remain at 29 and 30 percent increases over three years, which we’ve told them is unrealistic and unaffordable,” Omodt said, noting that the average Minnesota nurse makes $80,960 a year.
Contracts expired in May and June, and the union has been in negotiations since March.
Nurses said they are frustrated the strike is happening, but the stakes are high for them and their patients.
“We’re really sad and disappointed that it has come to a strike,” said Brianna Hnath, a nurse at North Memorial in Robbinsdale. “But we feel like this is the only thing we can do to show administration how incredibly important a strong nursing core is to a hospital. Hospitals tell us it’s our fault, but we’ve been actively involved and getting nowhere.”
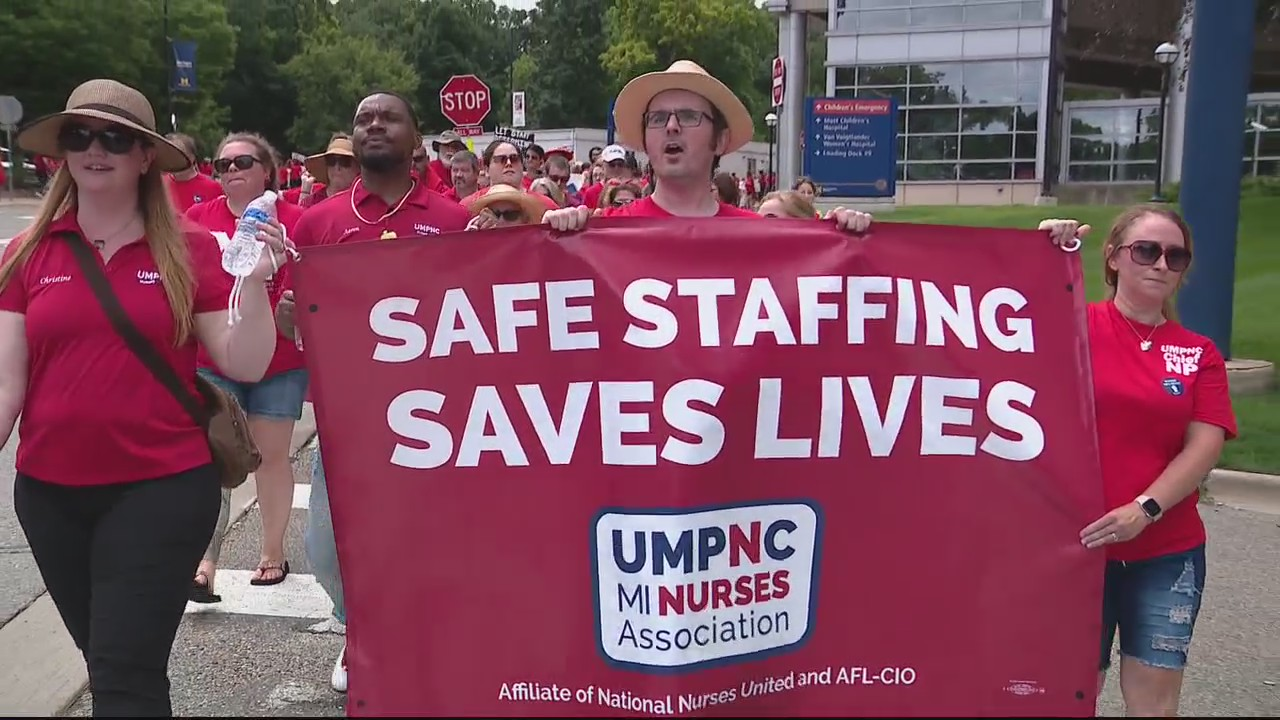
Members of the Michigan Nurses Association are accusing the University of Michigan of unlawfully refusing to negotiate over nurses’ workloads in its bargaining with the University of Michigan Professional Nurse Council.
The union, an affiliate of National Nurses United and AFL-CIO, represents about 13,000 registered nurses and healthcare professionals in Michigan, including workers employed by the University of Michigan. The University of Michigan regents hold the contract with the University of Michigan Professional Nurse Council, the largest bargaining unit of the Michigan Nurses Association.
A total of 6,200 University of Michigan Health nurses have been working without a new contract since July 1, and they are working under the terms of the expired agreement, according to hospital and union statements. The University of Michigan Health, the clinical division of Ann Arbor-based Michigan Medicine, told Becker’s in a statement that during negotiations, it has offered a 21 percent base pay increase for nurses over the life of the contract, as well as a new salary step program for nurse practitioners and the safe elimination of mandatory overtime.
The union contends the University of Michigan has refused to bargain over safe workloads regarding the number of patients assigned per nurse, which it says is tied directly to nurses’ patient safety concerns. As a result, it filed a lawsuit Aug. 15 in the Michigan Court of Claims.
“When nurses are forced to take care of too many people at once, patient care gets compromised and nurses are put in danger of injury or burnout, and that’s happening far too often at our hospital,” said Renee Curtis, RN, president of the University of Michigan Professional Nurse Council, said in a news release.
“University of Michigan Health makes staffing determinations with patient safety at the forefront of its decisions, and this has produced outstanding safety results,” the health system said in its statement. “The health system continuously receives recognition as Michigan’s safest hospital with recent recognitions by top agencies.”
University of Michigan Health also said it “plans to vigorously defend itself” against the union lawsuit.
As RNs struggle to work through staffing shortages, their job satisfaction has sharply declined, with 67% saying they plan to leave their jobs within the next few years, according to a survey from the American Association of Critical-Care Nurses (AACN) published in Critical Care Nurse.
RNs cite poor work environments
For the survey, AACN collected responses from 9,862 nurses, 9,335 of which met the study criteria of being currently practicing RNs, in October 2021. The mean age was 46.5 years, and the mean years of experience was 17.8 years.
Of the participants, 78.3% worked in direct care, and 19.4% worked in a Beacon unit, meaning that their unit had been recognized by an AACN Beacon Award for Excellence. Half of the participants said they spent 50% or less of their time caring for Covid-19 patients, while the other half said they spent 50% or more.
To measure the health of a work environment, AACN looked at six standards:
Skilled communication
True collaboration
Effective decision-making
Meaningful recognition
Authentic leadership
Appropriate staffing
Overall, AACN found that nurses’ perceptions of quality on these six measures had declined across the board since the organization’s 2018 survey.
In particular, appropriate staffing was the lowest rated of all the standards at 2.33 out of 4, which is the lowest rating the standard has received since AACN first began the survey in 2006. Only 24% of RNs said their units had the right number of nurses with the right knowledge and skills more than 75% of the time—down from 39% who said the same in 2018.
In addition, there was a significant decline in how RNs rated the quality of care in their organizations and their units. Only 16% rated their organizations’ quality of care as excellent (compared to 24% in 2018), and 30% rated their units’ quality of care as excellent (compared to 44% in 2018). Over 50% of nurses said quality of care in their organization or unit has gotten somewhat or much worse over the last year.
Many nurses also reported difficulties with their physical and psychological well-being in the survey. For example, less than 50% of RNs said they felt their organization values their health and safety, a significant decline from 68% who said the same in 2018.
In addition, 40% of participants reported that they were not emotionally healthy. The percentage of RNs who reported experiencing moral distress also doubled from 11% in 2018 to 22% in 2021.
A significant portion of RNs also reported experiencing verbal abuse, physical abuse, sexual harassment, or discrimination over the past year. Of the 7,399 RNs who answered this question, 72% said they had experienced at least one negative incident, with verbal abuse being the most common at 65%, followed by physical abuse at 28%.
RN job satisfaction
Only 40% of RNs said they were “very satisfied” with their job, down from 62% who said the same in 2018. Further, a significant number of RNs in the survey reported planning to leave their jobs within the next few years.
Overall, 67% of RNs said they planned to leave their current position within the next three years, compared to 54% in 2018. Of this group, 36% said they planned to leave within the next year, with 20% planning to leave within the next six months.
According to the respondents, the top factors that could lead them to reconsider their decision to leave their job were a higher salary and more benefits (63%), better staffing (57%), and more respect from administration (50%).
“Without improvements in the work environment, the results of this study indicate that nurses will continue to exit the workforce in search of more meaningful, rewarding, and sustainable work,” the survey’s authors wrote. “It is time for bold action, and this study shows the way.” (Firth, MedPage Today, 8/3; Ulrich et al., Critical Care Nurse, 8/1)
Hard truths on the current and future state of the nursing workforce
Concerns about an imbalance in supply and demand in the nursing workforce have been around for years. The number of nursing professionals nationally may be healthy, but many nurses are not in the local areas, sites of care, or roles where they’re needed most. And many of today’s nurses don’t have the specialized skills they need, widening the existing gap between nurse experience and job complexity.
As a result, gaping holes in staffing rosters, prolonged vacancies, unstable turnover rates, and unchecked use of premium labor are now common.
Health care leaders need to confront today’s challenges in the nursing workforce differently than past cyclical shortages. In this report, we present six hard truths about the nursing workforce. Then, we detail tactics for how leaders can successfully address these challenges—stabilizing the nursing workforce in the short term and preparing it for the future.
Health care workers nationwide are organizing and pushing for workplace changes like better pay or more favorable staffing ratios after waves of pandemic-fueled burnout and frustration.
Why it matters: COVID-19 and its aftereffects triggered an exodus of health care workers. Those who stayed are demanding more from health systems that claim to be reaching their own breaking points.
“The pandemic exacerbated a crisis that was already there,” Michelle Boyle, a Pittsburgh nurse told Axios. “It went from being a crisis to being a catastrophic freefall in staffing.”
Driving the news: About 1,400 resident physicians in public Los Angeles County hospitals have authorized a strike if their demands for pay parity with other local facilities aren’t met in contract negotiations this week.
Nurses demonstrated across Pennsylvania in early May, protesting one state lawmaker’s inaction on legislation that would have set nurse-to-patient ratios.
A fight is brewing in Minnesota as contracts covering 15,000 nurses in several hospital systems are expiring.
Some 2,000 resident physicians and interns at Stanford University and the University of Vermont Medical Center joined an affiliate of the SEIU for medical workers that claims more than 20,000 members nationwide.
In North Carolina, where union membership is low, staff at Mission Health in Asheville voted to unionize largely over staffing concerns.
Less than half of the of nearly 12,000 nurses polled by the American Nurses Association last year believe their employer cares about their concerns, and 52% of those surveyed said they intend to leave their jobs or are considering doing so.
The other side: Hospital operators generally oppose unionization efforts, as well as mandated staffing ratios.
“The last thing we need is requirements set by somebody in Washington as to exactly how many nurses ought to be providing service at any given time,” said Chip Kahn, CEO of the Federation of American Hospitals. “That ought to be a local decision based on the need in the hospital at the time.”
The American Organization for Nursing Leadership, an affiliate of the American Hospital Association, also opposes staffing ratios.
The industry says decisions on staffing and workplace rules are best left to local executives who need to be flexible to meet shifting demand for care.
“You’re basically taking away the flexibility of those on the scene to determine what it takes to provide the needed patient care,” Kahn said.
Go deeper: The pandemic drove up labor costs significantly for hospitals that were forced to pay travel nurses to fill workforce gaps during COVID surges.
April marked the fourth month in a row this year that major hospitals and health care systems reported negative margins, a Kaufman Hall report found. And executives say things could worsen amid inflation and stubborn supply chain woes.
And yet, some big hospital chains like Tenet reported strong earnings in the first quarter.
Between the lines: California is the only state to have set staffing ratios for nurses, but hospital unions in other states have fought for similar requirements in their contracts.
In California, every nurse on a general hospital floor has no more than five patients to care for at a time; nurses in ICUs should care for no more than two patients.
Nurses want look-alike standards in states like Pennsylvania, where only some hospitals have staffing ratios, saying short-staffing threatens patients’ well-being.
What we’re watching: While many legislative proposals failed this year, unions representing health care workers say their message is getting across.
Unions in Illinois, Pennsylvania and Washington state are redoubling efforts for staffing ratio legislation modeled on California’s.
In New York, nurses passed a law that took effect in January mandating staffing committees at hospitals.
The bottom line: The labor tension is a sobering coda to a health crisis that’s stretched health systems and workers alike in unprecedented ways.
“What you’re seeing is nurses finally saying enough is enough and this system is broken and we need it to be fixed,” said Denelle Korin, a nurse alliance coordinator with Nurses of Pennsylvania.
The US healthcare sector added 64K jobs in February, an increase from recent months, but the gains were concentrated in provider offices and home health companies. Hospitals and nursing facilities, which have both struggled with widespread staffing shortages, saw more anemic job growth. In particular, nursing homes have lost 15 percent of their workforce, remaining significantly understaffed even though resident occupancy rates still lag pre-pandemic levels. This week, nursing home groups pushed back against President Biden’s call for minimum staffing levels, calling them unrealistic without federal funding.
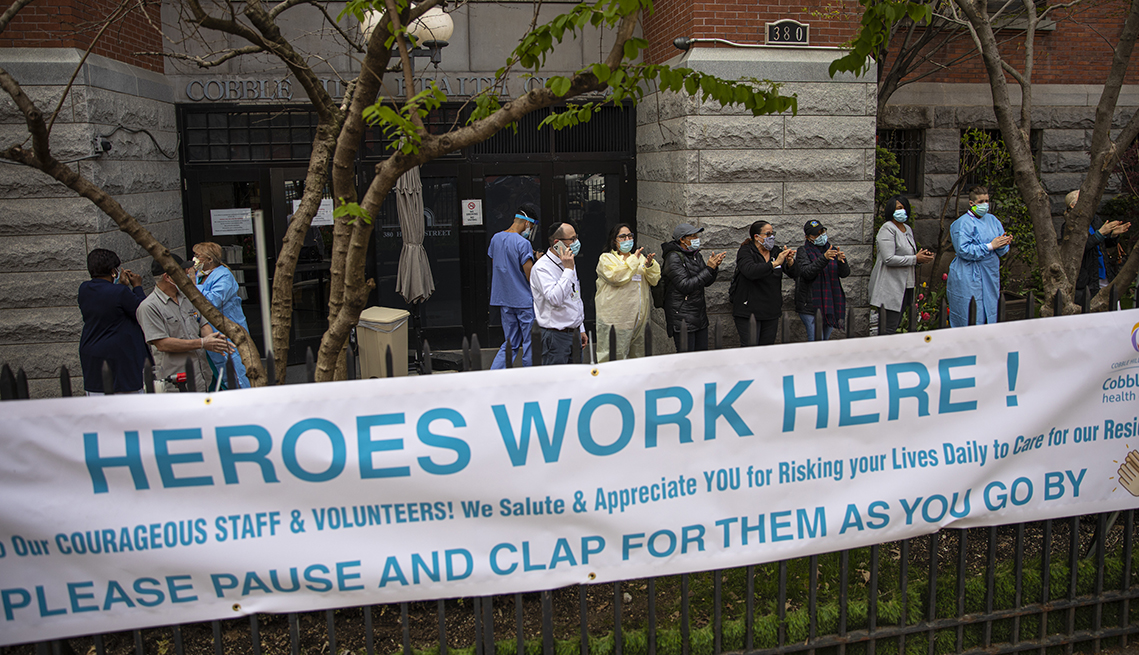
The Gist: Hospital and nursing facility workers have taken on some of the most taxing and dangerous jobs during the pandemic, caring for the sickest patients while personally risking COVID infection.
Healthcare workers are increasingly opting for safer, less intense jobs in outpatient care settings like physician offices, or are exiting direct patient care entirely. Even as the pandemic subsides, recruitment and retention of nurses and other caregivers will be of paramount importance, given rising vacancy rates and unabating staff shortages.
At the 390-bed Terrace View nursing home on the east side of Buffalo, 22 beds are shut down. There isn’t enough staff to care for a full house, safely or legally.
That means some fully recovered patients in the adjacent Erie County Medical Center must stay in their hospital rooms, waiting for a bed in the nursing home. Which means some patients in the emergency department, who should be admitted to the hospital, must stay there until a hospital bed opens up. The emergency department becomes stretched so thin that 10 to 20 percent of arrivals leave without seeing a caregiver — after an average wait of six to eight hours, according to the hospital’s data.
“We used to get upset when our ‘left without being seen’ went above 3 percent,” said Thomas Quatroche, president and chief executive of the Erie County Medical Center Corp., which runs the 590-bed public safety net hospital.
Nursing home bed and staff shortages were problems in the United States before the coronavirus pandemic. But the departure of 425,000 employees over the past two years has narrowed the bottleneck at nursing homes and other long-term care facilities at the same time that acute care hospitals are facing unending demand for services due to a persistent pandemic and staff shortages of their own.
With the omicron variant raising fears of even more hospitalizations, the problems faced by nursing homes are taking on even more importance. Several states have sent National Guard members to help with caregiving and other chores.
Hospitalizations, which peaked at higher than 142,000 in January, are rising again as well, reaching more than 71,000 nationally on Thursday, according to data tracked by The Washington Post. In some places, there is little room left in hospitals or ICUs.
About 58 percent of the nation’s 14,000 nursing homes are limiting admissions, according to a voluntary survey conducted by the American Health Care Association, which represents them. According to the U.S. Bureau of Labor Statistics, 425,000 employees, many of them low-paid certified nursing assistants who are the backbone of the nursing home workforce, have left since February 2020.
“What we’re seeing on the hospital side is a reflection of that,” said Rob Shipp, vice president for population health and clinical affairs at the Hospital Association of Pennsylvania, which represents medical providers in that state. The backups are not just for traditional medical inpatients ready for follow-up care, he said, but psychiatric and other patients as well.
A handful of developmentally disabled patients at Erie County Medical Center waited as long as a year for placement in a group setting, Quatroche said. Medical patients recovered from illness and surgery who cannot go home safely may wait days or weeks for a bed, he said.
“I don’t know if everyone understands how serious the situation is,” Quatroche said. “You really don’t know until you need care. And then you know immediately.”
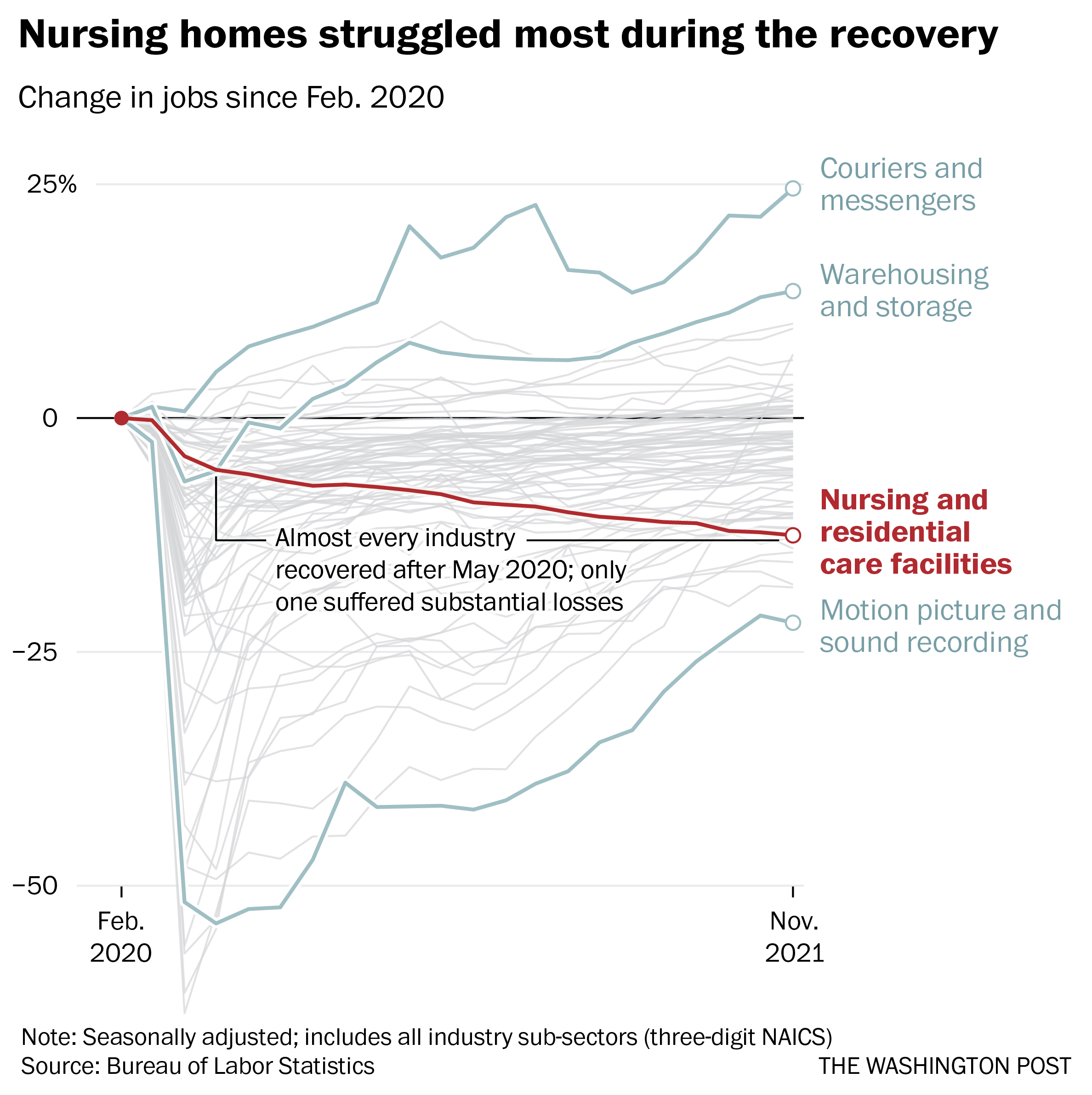
Nearly 237,000 workers left during the recovery, data through November show. No other industry suffered anything close to those losses over the same period, according to the Bureau of Labor Statistics.
Workers in the broader health-care industry have been quitting in record numbers for most of the pandemic, plagued by burnout, vulnerability to the coronavirus and poaching by competitors. Low-wage workers tend to quit at the highest rates, Labor Department data show, and nursing home workers are the lowest paid in the health sector, with nonmanagerial earnings averaging between $17.45 an hour for assisted living to $21.19 an hour for skilled nursing facilities, according to the BLS.
Nursing home occupancy fell sharply at the start of the pandemic, but inched back upward in 2021, according to the nonprofit National Investment Center for Seniors Housing and Care. One major force that held it back was worker shortages.
“Operators in the business have said we could admit more patients, but we cannot find the staff to allow that to happen,” said Bill Kauffman, senior principal at the organization.
Shortages have spawned fierce talent wars in the industry, Brookdale Senior Living Chief Executive Officer Cindy Baier said in a recent earnings call. When they don’t have enough workers, restaurants can reduce service hours and hospitals can cut elective surgeries, but nursing homes don’t have the option of eliminating critical services, she said. They must close beds.
“We are in the ‘people taking care of people’ business around-the-clock, 365 days a year,” she said.
Nursing homes tend to gain workers during a recession but can struggle to hire during expansions, according to an analysis of county-level data from the Great Recession recently published in the health care provision and financing journal Inquiry.
Steady income from their resident population and government programs such as Medicaid makes them recession-proof, and their low pay and challenging work conditions mean they’re chronically understaffed, said one of the study’s authors, Indiana University health-care economist Kosali Simon.
When recessions occur, nursing homes go on a hiring spree, filling holes in their staff with qualified workers laid off elsewhere.
“People during a recession may lose their construction jobs or jobs in retail sectors, and then look for entry-level positions at places like nursing homes where there is always demand,” Simon said.
Now, amid the “Great Resignation” and the hot job market, the opposite is happening. In sparsely populated areas and regions where pay is lower, the problem is even worse.
The Diakonos Group, which operates 26 nursing homes, assisted-living facilities and group homes in Oklahoma, closed an 84-bed location for seniors with mental health needs in May “simply because we couldn’t staff it any longer,” said Chief Executive Officer Scott Pilgrim. Patients were transferred elsewhere, including Tulsa and Oklahoma City, he said.
The home in rural Medford, which depended entirely on Medicaid payments, “was never easy to staff, but once we started through covid and everything, our staff was just burned out.”
Diakonos boosted certified nursing assistants’ pay from $12 an hour and licensed practical nurses’ pay from $20 an hour, used federal and state assistance to offer bonuses and employed overtime, but workers kept leaving for better health-care jobs and positions in other industries, he said.
“I’ve never been able to pay what we ought to pay,” Pilgrim said. Eventually he began to limit admissions and eventually was forced to close.
“The hospitals are backed up,” he said. “They’re trying to find anywhere to send people. We get referrals from states all around us. The hospitals are desperate to find places to send people.”
In south central Pennsylvania, SpiriTrust Lutheran is not filling 61 of its 344 beds in six facilities because of the worker shortage, said Carol Hess, the company’s senior vice president.
“I have nurses who went to become real estate agents,” she said. “They were just burned out.”
Pay raises of $1 to $1.50 an hour and bonuses brought the lowest-paid workers to about $15 an hour, Hess said, and the company is planning a recruiting drive after Jan. 1. But the prognosis is still grim.
“We’re competing with restaurants for our dining team members,” Hess said. “We’re competing with other folks for cleaning and laundry and others.” In the area around Harrisburg where SpiriTrust employees live, some schools that turned out certified nurse assistants closed during the pandemic and haven’t reopened.
The nursing homes have begun borrowing licensed practical nurses from WellSpan Health, the nearby hospital system that discharges many of its patients to SpriTrust after they recover. About 15 have began their orientations this month, she said, and the two systems are collaborating to pay them.
The bed shortage is causing backups that can average several days in the hospital, said Michael Seim, the hospital system’s chief quality officer. That gives the hospitals an interest in helping any way they can, he said.
“We have between 80 and 100 patients waiting for some type of skilled care,” Seim said this month. The hospital has begun caring for more people at home, enrolling 400 people so far in a program that sends clinicians to check on them there. More than 90 percent have said they are happy with the program.
“I think the future of hospital-based care is partnerships,” Seim said. “It’s going to be health systems partnering across their service areas … to disrupt the model we have.”
The healthcare industry’s staffing shortage crisis has had clear consequences for care delivery and efficiency, forcing some health systems to pause nonemergency surgeries or temporarily close facilities. Less understood is how these shortages are affecting care quality and patient safety.
A mix of high COVID-19 patient volume and staff departures amid the pandemic has put hospitals at the heart of a national staffing shortage, but there is little national data available to quantify the shortages’ effects on patient care.
The first hint came last month from a CDC report that found healthcare-associated infections increased significantly in 2020 after years of steady decline. Researchers attributed the increase to challenges related to the pandemic, including staffing shortages and high patient volumes, which limited hospitals’ ability to follow standard infection control practices.
“That’s probably one of the first real pieces of data — from a large scale dataset — that we’ve seen that gives us some sense of direction of where we’ve been headed with the impact of patient outcomes as a result of the pandemic,” Patricia McGaffigan, RN, vice president of safety programs for the Institute for Healthcare Improvement, told Becker’s. “I think we’re still trying to absorb much of what’s really happening with the impact on patients and families.”
An opaque view into national safety trends
Because of lags in data reporting and analysis, the healthcare industry lacks clear insights into the pandemic’s effect on national safety trends.
National data on safety and quality — such as surveys of patient safety culture from the Agency for Healthcare Research and Quality — can often lag by several quarters to a year, according to Ms. McGaffigan.
“There [have been] some declines in some of those scores more recently, but it does take a little while to be able to capture those changes and be able to put those changes in perspective,” she said. “One number higher or lower doesn’t necessarily indicate a trend, but it is worth really evaluating really closely.”
For example, 569 sentinel events were reported to the Joint Commission in the first six months of 2021, compared to 437 for the first six months of 2020. However, meaningful conclusions about the events’ frequency and long-term trends cannot be drawn from the dataset, as fewer than 2 percent of all sentinel events are reported to the Joint Commission, the organization estimates.
“We may never have as much data as we want,” said Leah Binder, president and CEO of the Leapfrog Group. She said a main area of concern is CMS withholding certain data amid the pandemic. Previously, the agency has suppressed data for individual hospitals during local crises, but never on such a wide scale, according to Ms. Binder.
CMS collects and publishes quality data for more than 4,000 hospitals nationwide. The data is refreshed quarterly, with the next update scheduled for October. This update will include additional data for the fourth quarter of 2020.
“It is important to note that CMS provided a blanket extraordinary circumstances exception for Q1 and Q2 2020 data due to the COVID-19 pandemic where data was not required nor reported,” a CMS spokesperson told Becker’s. “In addition, some current hospital data will not be publicly available until about July 2022, while other data will not be available until January 2023 due to data exceptions, different measure reporting periods and the way in which CMS posts data.”
Hospitals that closely monitor their own datasets in more near-term windows may have a better grasp of patient safety trends at a local level. However, their ability to monitor, analyze and interpret that data largely depends on the resources available, Ms. McGaffigan said. The pandemic may have sidelined some of that work for hospitals, as clinical or safety leaders had to shift their priorities and day-to-day activities.
“There are many other things besides COVID-19 that can harm patients,” Ms. Binder told Becker’s. “Health systems know this well, but given the pandemic, have taken their attention off these issues. Infection control and quality issues are not attended to at the level of seriousness we need them to be.”
What health systems should keep an eye on
While the industry is still waiting for definitive answers on how staffing shortages have affected patient safety, Ms. Binder and Ms. McGaffigan highlighted a few areas of concern they are watching closely.
The first is the effect limited visitation policies have had on families — and more than just the emotional toll. Family members and caregivers are a critical player missing in healthcare safety, according to Ms. Binder.
When hospitals don’t allow visitors, loved ones aren’t able to contribute to care, such as ensuring proper medication administration or communication. Many nurses have said they previously relied a lot on family support and vigilance. The lack of extra monitoring may contribute to the increasing stress healthcare providers are facing and open the door for more medical errors.
Which leads Ms. Binder to her second concern — a culture that doesn’t always respect and prioritize nurses. The pandemic has underscored how vital nurses are, as they are present at every step of the care journey, she continued.
To promote optimal care, hospitals “need a vibrant, engaged and safe nurse workforce,” Ms. Binder said. “We don’t have that. We don’t have a culture that respects nurses.”
Diagnostic accuracy is another important area to watch, Ms. McGaffigan said. Diagnostic errors — such as missed or delayed diagnoses, or diagnoses that are not effectively communicated to the patient — were already one of the most sizable care quality challenges hospitals were facing prior to the pandemic.
“It’s a little bit hard to play out what that crystal ball is going to show, but it is in particular an area that I think would be very, very important to watch,” she said.
Another area to monitor closely is delayed care and its potential consequences for patient outcomes, according to Ms. McGaffigan. Many Americans haven’t kept up with preventive care or have had delays in accessing care. Such delays could not only worsen patients’ health conditions, but also disengage them and prevent them from seeking care when it is available.
Reinvigorating safety work: Where to start
Ms. McGaffigan suggests healthcare organizations looking to reinvigorate their safety work go back to the basics. Leaders should ensure they have a clear understanding of what their organization’s baseline safety metrics are and how their safety reports have been trending over the past year and a half.
“Look at the foundational aspects of what makes care safe and high-quality,” she said. “Those are very much linked to a lot of the systems, behaviors and practices that need to be prioritized by leaders and effectively translated within and across organizations and care teams.”
She recommended healthcare organizations take a total systems approach to their safety work, by focusing on the following four, interconnected pillars:
Culture, leadership and governance
Patient and family engagement
Learning systems
Workforce safety
For example, evidence shows workforce safety is an integral part of patient safety, but it’s not an area that’s systematically measured or evaluated, according to Ms. McGaffigan. Leaders should be aware of this connection and consider whether their patient safety reporting systems address workforce safety concerns or, instead, add on extra work and stress for their staff.
Safety performance can slip when team members get busy or burdensome work is added to their plates, according to Ms. McGaffigan. She said leaders should be able to identify and prioritize the essential value-added work that must go on at an organization to ensure patients and families will have safe passage through the healthcare system and that care teams are able to operate in the safest and healthiest work environments.
In short, leaders should ask themselves: “What is the burdensome work people are being asked to absorb and what are the essential elements that are associated with safety that you want and need people to be able to stay on top of,” she said.
To improve both staffing shortages and quality of care, health systems must bring nurses higher up in leadership and into C-suite roles, Ms. Binder said. Giving nurses more authority in hospital decisions will make everything safer. Seattle-based Virginia Mason Hospital recently redesigned its operations around nurse priorities and subsequently saw its quality and safety scores go up, according to Ms. Binder.
“If it’s a good place for a nurse to go, it’s a good place for a patient to go,” Ms. Binder said, noting that the national nursing shortage isn’t just a numbers game; it requires a large culture shift.
Hospitals need to double down on quality improvement efforts, Ms. Binder said. “Many have done the opposite, for good reason, because they are so focused on COVID-19. Because of that, quality improvement efforts have been reduced.”
Ms. Binder urged hospitals not to cut quality improvement staff, noting that this is an extraordinarily dangerous time for patients, and hospitals need all the help they can get monitoring safety. Hospitals shouldn’t start to believe the notion that somehow withdrawing focus on quality will save money or effort.
“It’s important that the American public knows that we are fighting for healthcare quality and safety — and we have to fight for it, we all do,” Ms. Binder concluded. “We all have to be vigilant.”
Conclusion
The true consequences of healthcare’s labor shortage on patient safety and care quality will become clear once more national data is available. If the CDC’s report on rising HAI rates is any harbinger of what’s to come, it’s clear that health systems must place renewed focus and energy on safety work — even during something as unprecedented as a pandemic.
The irony isn’t lost on Ms. Binder: Amid a crisis driven by infectious disease, U.S. hospitals are seeing higher rates of other infections.
“A patient dies once,” she concluded. “They can die from COVID-19 or C. diff. It isn’t enough to prevent one.”