A surge in COVID-19 infections has swept the country this summer, upending travel plans and bringing fevers, coughs and general malaise. It shows no immediate sign of slowing.
While most of the country and the federal government has put the pandemic in the rearview mirror, the virus is mutating and new variants emerging.
Even though the Centers for Disease Control and Prevention (CDC) no longer tracks individual infection numbers, experts think it could be the biggest summer wave yet.
So far, the variants haven’t been proven to cause a more serious illness, and vaccines remain effective, but there’s no certainty about how the virus may yet change and what happens next.
The highest viral activity right now is in the West, according to wastewater data from the CDC, but a “high” or “very high” level of COVID-19 virus is being detected in wastewater in almost every state. And viral levels are much higher nationwide than they were this time last year and started increasing earlier in the summer.
Wastewater data is the most reliable method of tracking levels of viral activity because so few people test, but it can’t identify specific case numbers.
Part of the testing decline can be attributed to pandemic fatigue, but experts said it’s also an issue of access.Free at-home tests are increasingly hard to find. The government isn’t distributing them, and private insurance plans have not been required to cover them since the public health emergency ended in 2023.
COVID has spiked every summer since the start of the pandemic. Experts have said the surge is being driven by predictable trends like increased travel and extreme hot weather driving more people indoors, as well as by a trio of variants that account for nearly 70 percent of all infections.
Vaccines and antivirals can blunt the worst of the virus, and hospital are no longer being overwhelmed like in the earliest days of the pandemic.
But there remains a sizeable number of people who are not up-to-date on vaccinations. There are concerns that diminished testing and low vaccination rates could make it easier for more dangerous variants to take hold.
“One of the things that’s distinctive about this summer is that the variants out there are extraordinarily contagious, so they’re spreading very, very widely, and lots of people are getting mild infections, many more than know it, because testing is way down,” said William Schaffner, a professor of preventive medicine and infectious diseases at Vanderbilt University.
That contagiousness means the virus is more likely to find the people most vulnerable — people over 65, people with certain preexisting conditions, or those who are immunocompromised.
In a July interview with the editor-in-chief of MedPage Today, the country’s former top infectious diseases doctor, Anthony Fauci, said people in high-risk categories need to take the virus seriously, even if the rest of the public does not.
“You don’t have to immobilize what you do and just cut yourself off from society,” Fauci said. “But regardless of what the current recommendations are, when you are in a crowded, closed space and you are an 85-year-old person with chronic lung disease or a 55-year-old person who’s morbidly obese with diabetes and hypertension, then you should be wearing a mask when you’re in closed indoor spaces.”
Schaffner said hospitalizations have been increasing in his region for at least the past five weeks, which surprised him.
“I thought probably they had peaked last week. Wrong. They went up again this week. So at least locally, we haven’t seen the peak yet. I would have expected this summer increase … to have plateaued and perhaps start to ease down. But we haven’t seen that yet,” he said.
Still, much of the country has moved on from the pandemic and is reacting to the surge with a collective shrug. COVID-19 is being treated like any other respiratory virus, including by the White House.
President Biden was infected in July. After isolating at home for several days and taking a course of the antiviral Paxlovid, he returned to campaign trial.
Biden is 81, meaning he’s considered high risk for severe infection. He received an updated coronavirus vaccine in September, but it’s not clear if he got a second one, which the CDC recommends for older Americans.
Updated vaccines that target the current variants are expected to be rolled out later this fall, and the CDC recommends everyone ages 6 months and older should receive one.
As of May, only 22.5 percent of adults in the United States reported having received the updated 2023-2024 vaccine that was released last fall and tailored to the XBB variant dominant at that time.
The immunity from older vaccines wanes over time, and while it doesn’t mean people are totally unprotected, Schaffner said, the most vulnerable should be cautious. Many people being infected now have significantly reduced immunity to the current mutated virus, but reduced immunity is better than no immunity.
People with healthy immune systems and who have previously been vaccinated or infected are still less likely to experience the more severe infections that result in hospitalization or death.
Almost “none of us are naive to COVID, but the people where the protection wanes the most are the most frail, the immunodeficient, the people with chronic underlying illnesses,” Schaffner said.
Everybody is waiting for rent relief to help bring overall inflation down. It might take longer than conventional wisdom suggests.
Why it matters:
A surge in market rents in 2021 and 2022 still has a ways to go in fully working its way through the economy, despite moderation in market rents since then, a new paper from a Boston Fed economist finds.
As a result, rents are on track to exert upward pressure on overall inflation for quite a while to come, the paper argues, a headwind to bringing inflation down to the Fed’s 2% target.
The big picture:
Rents soared during and immediately after the pandemic as Americans sought bigger homes and were flush with higher paychecks and pent-up savings. But private-sector indicators of market rents rose much faster than the rent numbers calculated for the Consumer Price Index and other inflation indicators at that time.
That’s because market rent data only encompasses people signing new leases. Many existing tenants saw no immediate change — perhaps because they had long-term leases in place, or landlords were reluctant to raise rent on existing tenants, or local laws constrained rent hikes.
But over time, those leases turn over, with more renters paying the higher market prices. That process is still underway, even though market rents have risen less in 2023 and 2024, according to the analysis from the Boston Fed’s Christopher D. Cotton.
By the numbers:
Compared to 2019 levels, there is a 6 percentage point gap between rents on new leases and the shelter inflation shown in the CPI.
The process of higher market rents filtering through the inflation data is on track to add 0.7 percentage point to the core Consumer Price Index over the next year and 0.3 percentage points to core inflation using the Fed’s preferred gauge, Cotton finds.
“The fact that market rents remain 6% higher than CPI-shelter relative to pre-pandemic implies that CPI-shelter will grow more quickly than market rents for the foreseeable future,” Cotton tells Axios.
Of note:
Fed vice chair Philip Jefferson noted last month that “market rents adjust more quickly to economic conditions than what landlords charge their existing tenants.”
“This lag suggests that the large increase in market rents during the pandemic is still being passed through to existing rents and may keep housing services inflation elevated for a while longer,” Jefferson said.
The intrigue:
One risk to watch is that even once the pandemic-era rent inflation has worked its way through the data, there could be a new surge in market rents due to under-supply.
Construction of new multifamily housing has plunged below pre-pandemic levels in recent months as builders grapple with high interest rates.
“Incrementalism.” The word is perceived as the enemy of hope for universal health care in the United States.
Those who advocate for single-payer, expanded Medicare for all tend to be on the left side of the political spectrum, and we have advanced the movement while pushing back on incremental change. But the profit-taking health industry giants in what’s been called the medical-industrial complex are pursuing their own incremental agenda, designed to sustain the outrageously expensive and unfair status quo.
In recent years, as the financial sector of the U.S. economy has joined that unholy alliance, scholars have begun writing about the “financialization” of health care.
It has morphed into the medical-financial-industrial complex (MFIC) so vast and deeply entrenched in our economy that a single piece of legislation to achieve our goal–even with growing support in Congress–remains far short of enough votes to enact.
If we are to see the day when all Americans can access care without significant financial barriers, policy changes that move us closer to that goal must be pursued as aggressively as we fight against the changes that push universal health care into the distant future. Labeling all positive steps toward universal health care as unacceptable “incrementalism” could have the effect of aiding and abetting the MFIC and increase the chances of a worst-case scenario: Medicare Advantage for all, a goal of the giants in the private insurance business. But words matter. Instead of “incremental,” let’s call the essential positive steps forward as “foundational” and not undermine them.
The pandemic crisis exposed the weaknesses of our health system. When millions of emergencies in the form of COVID-19 infections overtook the system, most providers were ill-prepared and understaffed. More than 1.1 million U.S. citizens died of COVID-19-related illness, according to the Centers for Disease Control.
For years, the MFIC had been advancing its agenda, even as the U.S. was losing ground in life expectancy and major measures of health outcomes. While health care profits soared in the years leading up to and during the pandemic, those of us in the single-payer movement demanded improved, expanded Medicare for all. And we were right to do so. Progress came through almost every effort. The number of advocates grew, and more newly elected leaders supported a single-payer plan. Bernie Sanders’ 2016 presidential bid proved that millions of Americans were fed up with having to delay or avoid care altogether because it simply cost too much or because insurance companies refused to cover needed tests, treatments and medications.
But as the demand for systemic overhaul grew, the health care industry was making strategic political contributions and finding ways to gain even more control of health policy and the political process itself.
Over the years, many in the universal health care movement have opposed foundational change for strategic reasons. Some movement leaders believed that backing small changes or tweaks to the current system at best deflected from our ultimate goal. And when the Patient Protection and Affordable Care Act was passed, many on the left viewed it as a Band-Aid if not an outright gift to the MFIC. While many physicians in our movement knew that the law’s Medicaid expansion and the provisions making it illegal for insurers to refuse coverage to people with preexisting conditions would save many thousands of lives, they worried that the ACA would further empower big insurance companies. Both positions were valid.
After the passage of the ACA, more of us had insurance cards in our wallets and access to needed care for the first time, although high premiums and out-of-pocket costs have become insurmountable barriers for many. Meanwhile, industry profits soared.
The industry expanded its turf. Hospitals grew larger, stand-alone urgent care clinics, often owned by corporate conglomerates, opened on street corners in cities across the country, private insurance rolls grew, disease management schemes proliferated, and hospital and drug prices continued the march upward. The money flowing into the campaign coffers of political candidates made industry-favored incremental changes an easier lift.
To change this “system” would require an overhaul of the whole economy. Single-payer advocates must consider that herculean task as they continue their work. We must understand that the true system of universal health care we envision would also disrupt the financial industry – banks, collection agencies, investors – an often-forgotten but extraordinarily powerful segment of the corporate-run complex.
Even if the research and data show that improved, expanded Medicare for all would save money and lives (and they do show that), that is not motivating for the finance folks, who fear that without unfettered control of health care, they might profit less. Eliminating medical bills and debt would be marvelous for patients but not for a large segment of the financial community, including bankruptcy attorneys.
Following the money in U.S. health care means understanding how deep and far the tentacles of profit reach, and how embedded they are now.
We know the MFIC positioned itself to continue growing profits and building more capacity. The industry made steady, incremental progress toward that goal. There is no illusion that better overall health for Americans is the mission of the stockholders who drive this industry. No matter what the marketers tell us, patients are not their priority. If too many of us get healthier, we might not use as much care and generate as much money for the owners and providers. Private insurers want enough premiums and government perks to keep flowing their way to keep the C-Suite and Wall Street happy.
More than health insurers
Health insurers are far from the only rapidly expanding component of the MFIC. A recent documentary, “American Hospitals: Healing a Broken System,” for example, explores a segment of the U.S. health industry that is often overlooked by policymakers and the media. Though they were unprepared for the national health crisis, hospitals endured the pandemic in this country largely because the dedicated doctors, nurses and ancillary staff risked their own lives to keep caring for COVID-19 patients while everything from masks, gowns and gloves to thermometers and respirators were in short supply. But make no mistake, many hospitals were still making money through the pandemic. In fact, some boosted their already high profits, and private insurance companies had practically found profit-making nirvana. Patients put off everything from colonoscopies to knee replacements, physical therapy to MRIs. Procedures not done meant claims not submitted, while monthly insurance premiums kept right on coming and right on increasing.
The pandemic was a time of turmoil for most businesses and families, yet the MFIC took its share of profits. It was pure gold for many hospitals until staffing pressures and supply issues grew more dire, COVID patients were still in need of care, and more general patient care needs started to reemerge.
We might be forgiven for thinking there wasn’t much regulating or legislating done around health care during the pandemic years. We’d be wrong. There was a flurry of legislation at the state level as some states took on the abuses of the private insurance industry and hospital billing practices.
And the movement to improve and expand traditional Medicare to cover all of us stayed active, though somewhat muted. The bills before Congress that expanded access to Medicaid during the pandemic through a continuous enrollment provision offered access to care for millions of people. Yet as that COVID-era expansion ended, many of those patients were left without coverage or access to care. This might have been a chance to raise the issue loudly, but the social justice movement did not sufficiently activate national support for maintaining continuous enrollment in Medicaid. Is that the kind of foundational change worth fighting for? I would argue it most certainly is.
As those previously covered by Medicaid enter this “unwinding” phase, many will be unable to secure equivalent or adequate health insurance coverage. The money folks began to worry as coverage waned. After all, sick people will show up needing care and they will not be able to pay for it. As of this writing, patient advocacy groups are largely on the sidelines.
But Allina Health took action. The hospital chain announced it would no longer treat patients with medical debt. After days of negative press, the company did an about-face.
Throughout the country, even as the pandemic loomed, the universal, single-payer movement focused on explaining to candidates and elected officials why improving and expanding Medicare to cover all of us not only is a moral imperative but also makes economic sense. In many ways, the movement has been tremendously effective: More than 130 city and county governing bodies have passed resolutions in support of Medicare for all, including in Seattle, Denver, Cincinnati, Washington, D.C., Tampa, Sacramento, Los Angeles, St. Louis, Atlanta, Duluth, Baltimore, and Cook County (Chicago).
The Medicare for All Act, sponsored by Rep Pramila Jayapal (D-Wash.) and Sanders (I-Vt.) has 113 co-sponsors in the House and 14 in the Senate. Another bill allowing states to establish their own universal health care programs has been introduced in the House and will be introduced soon in the Senate.
Moving us closer
The late Dr. Quentin Young was a young Barack Obama’s doctor in Chicago. Young spoke to his president-in-the-making patient about universal health care and Obama, then a state legislator, famously answered that he would support a single-payer plan if we were starting from scratch. Many in the Medicare–for-all movement dismissed that statement as accepting corporate control of health care.
But Young would steadfastly advocate for single-payer health care for years to come and as one of the founding forces behind Physicians for a National Health Program. Once Dr. Young was asked if the movement should support incremental changes. He answered, “If a measure makes it easier and moves us closer to achieving health care for all of us, we should support that wholeheartedly. And if a measure makes it harder to get to single-payer, we need to oppose it and work to defeat that measure.” Many people liked that response. Others were not persuaded.
But in recent years, PHNP has become a national leader in a broad-based effort to halt the privatization of Medicare through so-called Medicare Advantage plans and other means. A case can be made that those are incremental/foundational but essential steps to achieving the ultimate goal.
We must fight incrementally sometimes, for instance when traditional Medicare is threatened with further privatization. Bit by painful bit, a program that has served this nation so well for more than 50 years will be carved up and given over to the private insurance industry unless the foundational steps taken by the industry are met with resistance and facts at every turn. We can achieve our goal by playing the short game as well as the long game. Foundational change can be and has been powerful. It just has to be focused on the health and well-being of every person.
Two pioneers of mRNA research — the technology that helped the world tame the virus behind the Covid-19 pandemic — won the 2023 Nobel Prize in medicine or physiology on Monday.
Overcoming a lack of broader interest in their work and scientific challenges, Katalin Karikó and Drew Weissman made key discoveries about messenger RNA that enabled scientific teams to start developing the tool into therapies, immunizations, and — as the pandemic spread in 2020 — vaccines targeting the SARS-CoV-2 coronavirus. Moderna and the Pfizer-BioNTech partnership unveiled their mRNA-based Covid-19 shots in record time thanks to the foundational work of Karikó and Weissman, helping save millions of lives.
Karikó, a biochemist, and Weissman, an immunologist, performed their world-changing research on the interaction between mRNA and the immune system at the University of Pennsylvania, where Weissman, 64, remains a professor in vaccine research. Karikó, 68, who later went to work at BioNTech, is now a professor at Szeged University in her native Hungary, and is an adjunct professor at Penn’s Perelman School of Medicine.
The duo will receive 11 million Swedish kronor, or just over $1 million. Their names are added to a list of medicine or physiology Nobel winners that prior to this year included 213 men and 12 women.
The award was announced by Thomas Perlmann, secretary general of Nobel Assembly, in Stockholm. Perlmann said he had spoken to both laureates, describing them as grateful and surprised even though the pair has won numerous awards seen as precursors and had been tipped as likely Nobel recipients at some point.
Every year, the committee considers hundreds of nominations from former Nobel laureates, medical school deans, and prominent scientists from fields including microbiology, immunology, and oncology. Members try to identify a discovery that has altered scientists’ understanding of a subject. And according to the criteria laid out in Alfred Nobel’s will, that paradigm-shifting discovery also has to have benefited humankind.
The Nobel committee framed Karikó and Weissman’s work as a prime example of complementary expertise, with Karikó focused on RNA-based therapies and Weissman bringing a deep knowledge about immune responses to vaccines.
But it was not an easy road for the scientists. Karikó encountered rejection after rejection in the 1990s while applying for grants. She was even demoted while working at Penn, as she toiled away on the lower rungs of academia.
But the scientists persisted, and made a monumental discovery published in 2005 based on simply swapping out some of the components of mRNA.
With instructions from DNA, our cells make strands of mRNA that are then “read” to make proteins. The idea underlying an mRNA vaccine then is to take a piece of mRNA from a pathogen and slip it into our bodies. The mRNA will lead to the production of a protein from the virus, which our bodies learn to recognize and fight should we encounter it again in the form of the actual virus.
It’s an idea that goes back to the 1980s, as scientific advances allowed researchers to make mRNA easily in their labs. But there was a problem: The synthetic mRNA not only produced smaller amounts of protein than the natural version in our cells, it also elicited a potentially dangerous inflammatory immune response, and was often destroyed before it could reach target cells.
Karikó and Weissman’s breakthrough focused on how to overcome that problem. mRNA is made up of four nucleosides, or “letters”: A, U, G, and C. But the version our bodies make includes some nucleosides that are chemically modified — something the synthetic version didn’t, at least until Karikó and Weissman came along. They showed that subbing out some of the building blocks for modified versions allowed their strands of mRNA to sneak past the body’s immune defenses.
While the research did not gain wide attention at the time, it did catch the attention of scientists who would go on to found Moderna and BioNTech. And now, nearly 20 years later, billions of doses of mRNA vaccines have been administered.
For now, the only authorized mRNA products are the Covid-19 shots. But academic researchers and companies are exploring the technology as a potential therapeutic platform for an array of diseases and are using it to develop cancer vaccines as well as immunizations against other infectious diseases, from flu to mpox to HIV. An mRNA vaccine is highly adaptable compared to earlier methods, which makes it easier to alter the underlying recipe of the shot to keep up with viral evolution.
As she gained global fame, Karikó has been open about the barriers she encountered in her scientific career, which raised broader issues about the challenges women and immigrants can face in academia. But she’s said she always believed in the potential of her RNA research.
“I thought of going somewhere else, or doing something else,” Karikó told STAT in 2020, recalling the moment she was demoted. “I also thought maybe I’m not good enough, not smart enough. I tried to imagine: Everything is here, and I just have to do better experiments.”
Pent-up demand for delayed healthcare during the COVID-19 pandemic is pressuring medical costs for health insurers that had a financial windfall during the pandemic amid low utilization.
UnitedHealth, the parent company of the largest private payer in the U.S., expects its medical loss ratio — the share of premiums spent on member’s healthcare costs — to be higher than previously expected in the second quarter of 2023, due to a surge in outpatient care utilization among seniors, CFO John Rex said Tuesday during Goldman Sachs’ investor conference.
The news sent UnitedHealth’s stock down 7% in morning trade Wednesday, and affected other Medicare-focused health insurers as well. Humana, CVS and Centene — the three largest MA insurers by enrollee after UnitedHealth — dropped 13%, 6% and 8%, respectively.
Dive Insight:
The early days of COVID saw widespread halts in nonessential services, causing visits to plunge with an estimated one-third of U.S. adults delaying or foregoing medical care in the pandemic’s first year. By 2022, the sizable rebound in deferred care that many predicted had yet to materialize.
Now, early signs suggest utilization may again be increasing, with the cost of rebounding care coming around to hit payers. UnitedHealth now expects its MLR for the second quarter to reach or exceed its full-year target of 82.1% to 83.1%.
“As you look at a Q2, you would expect Q2 medical care ratio to be somewhere in the zone of probably the upper bound or moderately above the upper bound of our full-year outlook,” Rex said. “I would expect at this distance that the full year would probably settle in in the upper half of the existing range we set up.”
In comparison, the insurer reported an MLR of 82.2% in the first quarter of 2023. UnitedHealth’s MLR was 82% in 2022.
UnitedHealth said the MLR increase is because medical activity is normalizing after COVID kept seniors away from non-essential care.
“We’re seeing as behaviors kind of normalize across the country in a lot of different ways and mask mandates are dropped, especially in physician offices, we’re seeing that more seniors are just more comfortable accessing services for things that they might have pushed off a bit like knees and hips,” said Tim Noel, UnitedHealth’s chief executive for Medicare and retirement.
The Minnetonka, Minnesota-based insurer has seen strong outpatient demand through April, May and June, particularly in hips and knees with high volumes at its owned ambulatory surgical centers and within its Medicare business, executives said.
Inpatient volumes have remained consistent, and while outpatient utilization has increased, patient acuity has remained the same. Optum Health’s behavioral businesses are also seeing higher utilization in the second quarter, said Patrick Conway, CEO of Care Solutions at Optum, UnitedHealth’s health services division.
UnitedHealth doesn’t expect this higher activity to let up anytime soon. As a result, the payer incorporated higher outpatient utilization into its Medicare Advantage plan bids for 2024, which were placed in early June. The move attests to the longer duration of the trend, SVB Securities analyst Whit Mayo wrote in a note.
“Assuming it is going to end quickly wouldn’t be prudent on our part,” Rex said. “We’ll see how this progresses here.”
Headlines recently blared about the new review that looked at how effective masks are at preventing the transmission of flu-like disease. Cochrane reviews are well respected, and the media coverage about the recent review has been hard to parse. So is that it, end of story on masks? Not if you skip the media headlines and read the actual review!
While hospitals, payers, and private equity firms have long been competing to acquire independent physician groups, theCOVID pandemic spurred a marked acceleration of the physician employment trend, with non-hospital corporate entities leading the charge.
The graphic above uses data released by consulting firm Avalere Health and the nonprofit Physicians Advocacy Institute to show that nearly three quarters of American physicians were employed by a larger entity as of January 2022, up from 62 percent just three years prior.
While hospitals employ a majority of those physicians, corporate entities (a group that includes payers, private equity groups, and non-provider umbrella organizations) have been increasing their physician rolls at a much faster rate.
Corporate entities employed over 40 percent more physicians in 2022 than in 2019, and in the southern part of the country—a hotspot for growth of Medicare Advantage—corporate physician employment grew by over 50 percent.
We expect the move away from private practice, accelerated by the pandemic, will only continue as physicians seek financial returns, secure a path to retirement, and look to access capital for necessary investments to help grow and manage the increasing complexities of running a practice.
Published this week in the Washington Post, this sobering article surveys the dismantling of our nation’s patchwork public health infrastructure, driven by a backlash to COVID pandemic restrictions. Positioning themselves as defenders of freedom, a coalition of conservative and libertarian activists, legislators, and judges have neutered many of the nation’s public health authorities. State health officials and governors in over half the country are now unable to issue mask mandates or order school closures without the permission of their state legislatures.
While the implications for a hypothetical “next COVID” are dire, we’re already seeing the consequences today: officials in Columbus, OH can no longer, for example, quarantine a child with measles, or shut down a restaurant experiencing a hepatitis A outbreak.
The Gist: The anti-public health backlash in the wake of COVID has now been codified, with far reaching consequences for future disease outbreaks. COVID protections for hospital-based healthcare providers are winding down, even in states like California which quickly embraced masking.
But now in over half the country, many reasonable responses to unknown future health threats won’t even be on the table, or will involve debate and legislative action, wasting precious response time.
In his second State of the Union speech on Feb. 7, President Joe Biden made it clear that the Administration is moving into the next phase of the COVID-19 pandemic—one in which the threats of disease and death are considerably diminished, and therefore no longer require the resources and urgent allocation of funds that the previous two years have.
“While the virus is not gone…we have broken COVID’s grip on us,” Biden said. “And soon we’ll end the public health emergency.”
The President outlined his reasons for not renewing the COVID-19 national and public health emergencies when they expire on May 11, which have been extended every 90 days since they were established in 2020. The decision represents a de-escalation in the way the government is treating the pandemic.
But health experts say now is not the time to let down our collective guard on SARS-CoV-2. “I don’t believe the virus has gotten the memo that the pandemic is winding down,” says Dr. Jeffrey Glenn, director of the Stanford Biosecurity and Pandemic Preparedness Initiative.
“There is a disconnect between the broad perception that the pandemic is behind us, and focusing on getting back to life as it was pre-pandemic,” says Wafaa El-Sadr, founder and director of the International Center for AIDS Care and Treatment Programs (ICAP) at Columbia University’s Mailman School of Public Health. “But the reality is that we still continue to have substantial transmission and deaths due to COVID in the U.S., and we are in a situation where the virus will be with us for a long time.”
Even when the emergency states end, therefore, the pandemic will not be over, they and others say.
One reason is that the definition of a “pandemic” is primarily based on the breadth and speed of a virus’ spread, and the amount of the world affected by a pathogen. It’s only partially related to the severity of disease caused by a virus like SARS-CoV-2, or even the amount of immunity a population may have against it.
By that main criterion, COVID-19 is still very much with us, with around 200,000 new cases and 1,000 deaths a day globally. The latest Omicron variants quashed any hope of the pandemic ending any time soon. While they do not cause more serious infections than past variants, they have mastered the challenge of hopping more efficiently from one infected person to another.
Even though the pandemic is far from over, many health experts agree that ending the U.S. national emergencies is justified at this point. When these measures were first implemented in 2020, most people were immunological sitting ducks for the virus. The declarations were designed to devote financial resources and personnel to controlling the impact of infections on the population’s health as much as possible by shoring up the health care system and later by providing free vaccinations. U.S. officials decided to end the national and public health emergencies in May primarily because most people have either been vaccinated or have recovered from an infection (or both), so the population’s immunity stands at a higher level. COVID-19 cases—both overall and the severe kind—have declined considerably since those early days.
But the continuing stream of infections means that the virus is still reproducing and churning out mutations. So far, those variants haven’t caused more serious disease—but that’s purely by chance, which makes public health experts uncomfortable with declaring victory just yet. Even though COVID-19 cases are no longer inundating most hospitals, that means it’s time to rethink the COVID-19 response, not abandon it.
The best way forward at this point is to refine and target COVID-19 services to optimize the chances of controlling the virus where it may be causing the most health problems. “I think we need to move away from universal guidance on vaccines and boosters and mitigation measures where everybody gets the same guidance, to a more differentiated and tailored approach based on the different characteristics—both socioeconomic and clinical—of different groups of people,” says El-Sadr. “We are at a different moment in the pandemic, so the moment is now for a different message.”
That message isn’t to put COVID-19 completely behind us, but to move forward armed with the lessons we’ve learned from our experience—the most important of which is never to underestimate SARS-CoV-2.
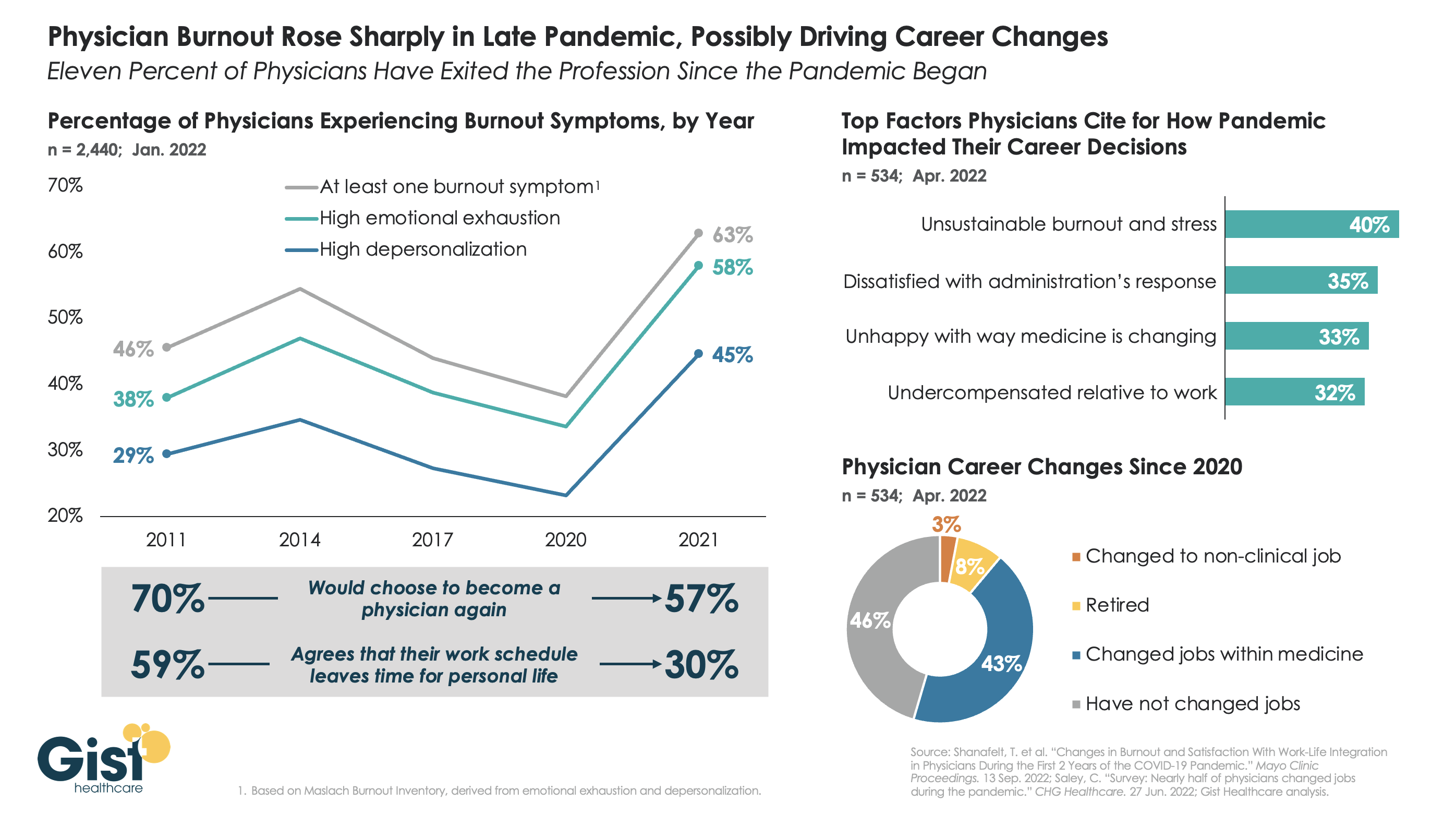
The long hours, stressful conditions, and labor shortages brought on by the pandemic have done serious harm to the physician workforce. The graphic above tracks physician burnout, a combination of emotional exhaustion, loss of agency, and depersonalization that has become the primary measure of the pandemic’s toll on workers, to reveal that physicians are demoralized like never before.
Physician burnout levels had been decreasing since 2014, in part due to practice consolidation and the expansion of team-based care models. Burnout reached its lowest levels in 2020—perhaps explained by a pandemic-induced sense of purpose—but 2021 then saw a dramatic spike in every measure of physician dissatisfaction, as the heroic glow of the early pandemic faded, and an overtaxed and understaffed delivery system became the new norm.
In explaining how the pandemic has impacted their career decisions, surveyed physicians list unsustainable burnout and stress as their top concern, and 11 percent say they have exited the profession, either for retirement or a non-clinical job, in the past two years.Four in ten surveyed physicians report changing jobs since 2020, mainly within similar or different practice settings, citing a desire for better work-life balance as their primary motivation. (It should be caveated that these data are from a smaller survey of 534 physicians, 40 percent of whom identified as “early career”.)
While the solutions here aren’t new, they are challenging: we must continue to implement team-based care models that provide physicians top-of-license practice and improved work-life balance, remove administrative tasks wherever possible, and ensure that we are communicating and engaging physicians—employed and independent alike—in organizational strategy and decision-making.