China is facing an increasingly precarious situation as new COVID cases soar and the population seems to be hitting a breaking point with the government’s stringent zero-tolerance policies.
Why it matters: The world’s most populous nation has massive vulnerabilities heading into this winter, starting with the fact the vast majority of its population has yet to be exposed to the virus and has little ‘natural immunity.’
China’s vaccines didn’t work well compared to those distributed in the West, and the government refused to approve foreign vaccines and doesn’t have a version to combat Omicron.
Vaccine uptake was particularly low among the elderly.
And now, public outrage over new COVID lockdown restrictions has fueled rare protests, Axios’ Herb Scribner writes, with residents demanding the government to lift restrictions quickly and some calling for President Xi Jinping’s resignation.
State of play: Overall, China’s number of reported COVID cases and COVID deaths are far lower than other nations, but there have been recent reported spikes in overall numbers of cases and some new deaths.
It came after the Chinese government announced some easing of its zero-COVID policy, such as reducing mass testing and quarantine requirements, earlier this month.
Reality check: China’s doctors have warned that the health care system isn’t prepared for the huge outbreak likely to follow any easing of public health measures, Axios’ Bethany Allen-Ebrahimian writes.
That includes worries the nation doesn’t have enough ICU bed capacity to handle such outbreaks, according to the Financial Times.
Between the lines: Another concern is the potential evolution of a new, more dangerous variant if there’s a huge surge of infections, Christian Drosten, Germany’s most prominent virologist, told Bloomberg.
“Xi Jinping knows very well that he can’t simply let the virus loose,” Drosten said. “The Chinese population first needs to be as well vaccinated as we are.”
Be smart: China’s officials are scrambling to address the vaccine problem.
For instance, they are launching more aggressive vaccine drives and limiting movement among at-risk groups, including the elderly, the Washington Post reports.
But they have yet to open up the availability of mRNA vaccines from Pfizer-BioNTech and Moderna, opting to focus on their own, per the Post.
The bottom line: China’s zero-COVID policy has kept cases in China relatively low compared to the rest of the world.
But even as the societal and economic consequences of shutdowns become apparent, it faces a very difficult path ahead in unwinding strict public health policies.
Even as new omicron strains take over, Covid is no longer driving a majority of patients into the hospital. Still, doctors worry the virus could re-emerge as immunity wanes.
As the flu and RSV (respiratory syncytial virus) have spread rapidly this fall — inundating and overwhelming hospitals and their staff across the country — Covid has not.
In fact, Covid-related deaths and hospitalizations have fallen in recent months,despite the emergence of new omicron subvariants that evade immunity from previous infections and vaccination.
According to NBC News data, Covid deaths have fallen consistently since Aug. 31, when the seven-day average of daily Covid deaths was at 571. A month later, on Sept. 30, the number fell to 475. By Halloween, 365 were dying per day, on average, from Covid.
As of Nov. 14, the number had fallen to 316.
This week, the Centers for Disease Control and Prevention is expected to release new data on Covid-related mortality, finding that death rates began to decline in March 2022.
The overall hopeful sign of declining deaths could indicate yet another new Covid phase, doctors suggest. Fewer people sick enough to be hospitalized with Covid means that fewer people are dying of the illness.
The average number of Covid hospitalizations per day has decreased by 27.9% since Aug. 28, according to NBC News data.
Even better, Covid, it seems, is no longer sending a majority of patients into intensive care units.
“There has not been an increase in patients admitted to the hospital specific for Covid-related disease,” said Dr. Hugh Cassiere, director of critical care services at Sandra Atlas Bass Heart Hospital at North Shore University Hospital, part of Northwell Health in New York City.
Patients in his ICU with Covid were admitted with unrelated medical issues, and were subsequently found to be Covid-positive, Cassiere said.
“Not to say that it’s gone, but Covid has become a coincidental disease,” he said.
Dr. Vin Gupta, a pulmonologist and an affiliate faculty member at the University of Washington in Seattle, attributes the decline in deaths and severe Covid cases to a level of “baked-in immunity,” including vaccination, prior infection or a combination of the two.
While Covid-related hospitalizations are not currently increasing, Gupta warns that they could during the winter as immunity, especially from previous infection, diminishes.
“If you had Covid, say six to four months ago, you’re going to have less protection against hospitalization than if you were vaccinated,” Gupta said. “The duration and the robustness of protection wanes a lot more quickly if all you rely on is natural immunity.”
With that in mind, data from the Institute for Health Metrics and Evaluation, a research center within the University of Washington, suggest that Covid hospitalizations and deaths could tick up again in “mid-January at the earliest,” said Gupta, a medical analyst for NBC News and MSNBC.
Despite the encouraging decline in Covid deaths, another school of thought suggests that Covid has simply morphed into a new kind of fatal illness.
“Before everyone was vaccinated or had been infected, 80 or 90% of Covid looked exactly same. They had terrible pneumonia. They were in the ICU on respiratory support,” said Dr. Jeremy Faust, an emergency medicine physician at Brigham and Women’s Hospital and an instructor at Harvard Medical School in Boston.
Now, he said, “Covid deaths don’t all look the same.” While “baked-in immunity” may keep the most severe cases at a minimum, it is clear that Covid can wreak havoc on the body long after the infection has cleared.
“Somebody could have Covid and have a heart attack, and the primary cause of death is listed as a heart attack because that’s what really brought them to the hospital,” Faust said.
But, he added, “we’ll never know to what degree Covid triggered that heart attack.”
Hospitals in the future will look far more tech-enabled and consumer-focused — when patients are actually even getting care in a hospital building itself.
Why it matters: Hospitals were already pushing morecare outside their four walls before the pandemic. COVID accelerated that shift, forcing hospitals to reimagine what’s possible to deliver in patients’ homes, experts say.
The big picture: One way to picture what hospitals of the future will look like is to look at two brand new hospital buildings opened this fall by competing Pennsylvania health systems.
The buildings, by Penn Medicine and Highmark Health both offer hotel-like amenities such as better food, streaming services, and better-positioned outlets for cell phone charging. They’ve also made medical records more accessible to patients, executives say.
But they were also designed with the belief that, in the future, only the most complex care might be delivered in them.
State of play: Every medical room in Penn Medicine’s new $1.6 billion health pavilion can be turned into an ICU-capable room when needed.
It added 7% in costs to the project, but made sense considering the ICU demands of the pandemic and “not knowing what the future will be,” CEO Kevin Mahoney told Axios.
The hospital also offers patients bedside tablets that allow patients to control the light and temperature of the room, and to activate frosted privacy glass on the doors of their rooms.
The benefits are two-fold: patients really like it and it can help free up staff to focus on more critical tasks, Mahoney said.
“The pandemic was an amplifier for natural trends that were already starting to develop,” Highmark CEO David Holmberg told Axios. “The complexity of medical procedures [in hospitals] is going to be significantly higher.”
The bottom line: Tech advances will change the entire hospital experience no matter where the care is delivered.
Wearables will provide digital biomarkers to allow better patient monitoring from the home. “Smart” infrastructure will help patients find parking and navigate massive hospital campuses when they need to go into the hospital.
And 5G will allow doctors to pull up massive amounts of personalized data on a wireless screen in seconds, Hon Pak, chief medical officer at Samsung Electronics told Axios.
“The perspective we want to bring to the smart hospital is it’s not just about caring for the condition or the disease, but it’s about caring for the whole,” Pak said.
The Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
RemoteICU, a telemedicine provider group, is suing the Department of Health and Human Services and the Centers for Medicare and Medicaid Services for not reimbursing telehealth services provided by physicians who are located outside the United States, according to a federal lawsuit filed last week in Washington.
RICU wants reimbursement for telehealth services provided within the U.S., but not necessarily by a physician who lives within its borders.
The company employs physicians who live outside the country, but are U.S. board-certified critical-care specialists and licensed in one or more U.S. jurisdictions. With RICU’s telecommunications system, these physicians can provide critical-care services in U.S. hospital ICUs, the lawsuit said.
“Although RICU’s physicians live abroad, they serve as full-time, permanent staff members of the U.S. hospitals at which they serve patients,” the company said in the court filing.
“By employing U.S.-licensed intensivists who live overseas, RICU has enabled the American healthcare system to recapture talent that would otherwise be lost to it – and this has helped to alleviate the ongoing shortage of intensivists in American hospitals.“
When CMS expanded the list of telehealth services for which it reimbursed in December 2020 to include critical care services, RICU began offering its physicians to hospitals that couldn’t afford ICU telehealth without Medicare reimbursement, the court filing said.
However, after the company reached out to several officials from HHS and CMS, it was notified that Medicare could not reimburse the client hospitals for RICU’s services, because the Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
The company is seeking a preliminary injunction to stop HHS and CMS from denying Medicare reimbursement for telehealth services on the basis of a provider’s physical location outside of the United States at the time of service.
WHAT’S THE IMPACT?
RICU claims that, by failing to reimburse for the critical care telehealth services provided by its physicians, HHS and CMS are causing “immediate harm both to RICU and to the public.”
It argues that it’s filling a gap in critical care that has been exacerbated by the pandemic.
“There remains [a] significant unmet need for critical care services, as desperately sick patients have overwhelmed ICU resources across the country,” RICU said in the court filing.
“In some cases, lack of adequate care can mean the difference between life or death. And one of the groups most at risk from death and serious illness due to COVID-19 is the elderly – the very same population that relies upon Medicare.”
Without reimbursement, RICU says that some of its current clients, as well as potential customers, will not be able to offer its services.
The company argues that this causes “significant, unrecoverable monetary damages” because tele-ICU providers that use physicians located within the U.S. are eligible for reimbursement and therefore have a competitive edge over RICU.
Further, it says that it has already begun losing business because of hospitals’ inability to receive Medicare reimbursement.
THE LARGER TREND
CMS has widely expanded the list of telehealth services it will reimburse for during the pandemic to include services such as emergency department visits, initial inpatient and nursing facility visits, and discharge-day management.
While only 14 states currently have true “payment parity” for telehealth, 43 states and D.C. have implemented a telemedicine coverage law, according to Foley & Lardner report.
That report, among others, claims telehealth will continue to grow as an integral part of healthcare as time goes on.
Last year, Geisinger health system in Danville, Pennsylvania, implemented telehealth ICU technology in several of its hospitals to support its in-person clinical staff.
ON THE RECORD
“The Critical Care Ban is causing irreparable harm to RICU, which is suffering ongoing financial and reputational harms that cannot be remedied in the future,” the court filing said.
“The balance of the equities favors an injunction, because Defendants have already admitted that there is a desperate medical need for the critical care that RICU would provide but for the Critical Care Ban.
“And, finally, preliminary injunction would be in the public interest because, across the United States, Americans stricken by the COVID-19 pandemic are in desperate need of critical care – a need that RICU can help meet. It is not hyperbole to say that the requested injunctive relief is in the public interest because it could save lives.”
Additional evidence continued to suggest blood type may not only play a role in COVID-19 susceptibility, but also severity of infection, according to two retrospective studies.
In Denmark, blood type O was associated with reduced risk of developing COVID-19 (RR 0.87, 95% CI 0.83-0.91), based on the proportion of those with type O blood who tested positive for SARS-CoV-2 compared with a reference population, reported Torben Barington, MD, of Odense University Hospital, and colleagues.
However, there was no increased risk for COVID-19 hospitalization or death associated with blood type, the authors wrote in Blood Advances.
Limitations to the data include that ABO blood group information was only available for 62% of individuals, and that the sex of the testing population was skewed, with women accounting for 71% who tested negative and 67% who tested positive.
They pointed to the recent research that blood type plays a role in infection, noting the lower than expected prevalence of blood group O individuals among COVID-19 patients. Researchers also observed how blood groups are “increasingly recognized to influence susceptibility to certain viruses,” among them SARS-CoV-1 and norovirus, adding that individuals with A, B, and AB blood types may be at “increased risk for thrombosis and cardiovascular diseases,” which are important comorbidities among patients hospitalized with COVID-19.
ABO and RhD blood group information was available for 473,654 individuals who were tested for SARS-CoV-2 from February 27 to July 30, as well as for 2,204,742 individuals not tested for SARS-CoV-2 as a reference.
Of the individuals tested, 7,422 tested positive for SARS-CoV-2. About a third of both those who tested positive and negative were men, and those with positive tests were slightly older (52 vs 50, respectively).
Among individuals testing positive for SARS-CoV-2, about 38% (95% CI 37.5-39.5%) belonged to blood group O versus about 42% of those in the reference population. There were significantly more group A and AB individuals in the positive testing group versus the reference population, though the difference was non-significant for group B. When group O individuals were removed, there was no difference between the remaining groups.
Blood Type Linked to COVID-19 Severity?
Meanwhile, a second, smaller study in Blood Advances did report a connection between blood type and COVID-19 severity.
Blood types A or AB in COVID-19 patients were associated with increased risk for mechanical ventilation, continuous renal replacement therapy, and prolonged ICU admission versus patients with blood type O or B, according to Mypinder Sekhon, MD, of the University of British Columbia in Vancouver, and colleagues. Inflammatory cytokines did not differ between groups, however.
These authors also cited research that found that blood groups were linked to virus susceptibility, but that the relationship between SARS-CoV-2 infection severity and blood groups remains “unresolved.” However, COVID-19 appears to be a multisystem disease with renal and hepatic manifestations.
“If ABO blood groups play a role in determining disease severity, these differences would be expected to manifest within multiple organ systems and hold relevance for multiple resource-intensive treatments, such as mechanical ventilation and continuous renal replacement therapy,” Sekhon and colleagues wrote.
They collected data from six metropolitan Vancouver hospitals from Feb. 21 to April 28, identifying 95 COVID-19 patients admitted to an ICU with known ABO blood type.
Among these patients, 57 were group O or B, while 38 were group A or AB. A significantly higher proportion of A/AB patients required mechanical ventilation versus O/B patients (84% vs 61%, respectively, P=0.02). Similar figures were seen for patients requiring continuous renal replacement therapy (32% vs 9%, P=0.04). Median ICU stay length was also longer for A or AB patients compared with O or B patients (13.5 days vs 9 days, P=0.03).
There was no difference in probability of ICU discharge, and eight patients died in the O/B group versus nine patients in the A/AB group. Not surprisingly, biomarkers of renal and hepatic dysfunction were higher in the A/AB group, as well.
“The unique part of our study is our focus on the severity effect of blood type on COVID-19. We observed this lung and kidney damage, and in future studies, we will want to tease out the effect of blood group and COVID-19 on other vital organs,” Sekhon said in a statement.
About 25% of patients were missing data on blood group, and the nature of the study makes it impossible to infer causality, the authors acknowledged. Ethnic ancestry and outcomes in patients with COVID-19 could be an unaddressed confounder. Additionally, anti-A antibody titers may affect COVID-19 severity, and these were not measured.
Hospitals in Southern California will need to start rationing care if more action isn’t taken by the community to mitigate the spread of COVID-19, Chris Van Gorder, president and CEO of Scripps Health, wrote in a Dec. 28 op-ed for The San Diego Union-Tribune.
As of Dec. 29, 20,642 California residents were hospitalized with COVID-19. The state’s hospital bed capacity is 72,511. In San Diego County, where Scripps is headquartered, 18 intensive care unit beds were available as of Dec. 28, “not even enough to handle a single mass casualty incident,” Mr. Van Gorder wrote. Out of Scripps’ 173 ICU beds, seven staffed beds were available as of Dec. 28.
“This past weekend, one of our community hospitals ran out of room in their morgue. We are nearing the point where we have to make the decision of who gets care and who does not,” Mr. Van Gorder wrote.
He pleaded with the San Diego and California community to adhere to mask-wearing and social distancing guidelines, especially as the New Year’s Day holiday approaches. He called on residents to stay home for New Year’s, wear a mask, wash their hands, and not eat or drink with people who aren’t in their immediate family household.
Mr. Van Gorder’s commentary comes as Kaiser Permanente hospitals in Northern California are suspending elective, non-urgent procedures through Jan. 4 as they continue to face a surge in COVID-19 hospitalizations. The Oakland, Calif.-based system announced the suspension Dec. 26, days after Chair and CEO Greg Adams said during a news conference, “We simply will not be able to keep up if the COVID surge continues to increase. We’re at or near capacity everywhere.”
But first, we have a difficult period to get through. This week again saw record-breaking numbers of cases, hospitalizations, and deaths from COVID-19, with Thursday alone bringing more than 238,000 new cases—and a staggering 3,293 fatalities.
Nearly 115,000 Americans are currently hospitalized with COVID, a rise of 16 percent from just two weeks ago, and in many places a precarious capacity situation has turned perilous. Conditions have worsened precipitously in California, with only Tennessee, Oklahoma, and Rhode Island registering more daily COVID cases per 100,000 population than the Golden State, although cases are still on the rise across 80 percent of states and territories.
Intensive care availability in Southern California hit zero, with ICU volume there expected to double or triple by this time next month. The same stresses are playing out in dozens of markets across the country, leading to a staffing sustainability crisis that can’t be solved through paying overtime, cancelling vacations or looking to travel nurses to fill the gaps in a now nationwide crisis. With the Christmas and New Year’s holidays still ahead, experts predictCOVID cases won’t peak until sometime in mid-January, with a peak in hospitalizations and deaths following several weeks after.
Several states and cities tightened restrictions on gatherings and issued new stay-at-home orders, in an effort to keep new cases at a level that allows hospitals to manage through the next several weeks and maintain care quality and access for COVID and non-COVID patients alike. The coming weeks will require every American to take greater precautions than at any time during the course of this pandemic.
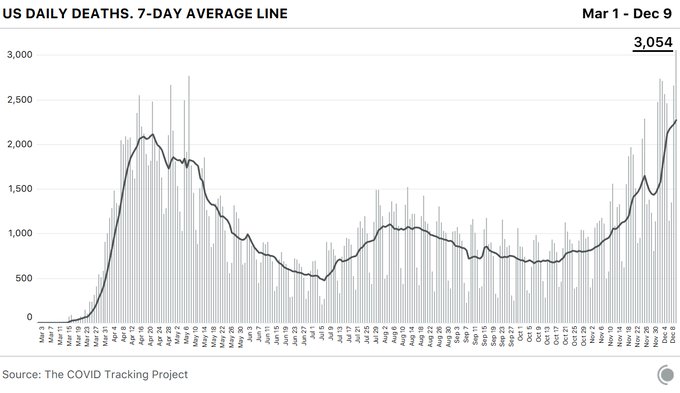
The coronavirus pandemic pushed the U.S. past another dire milestone Wednesday, the highest daily death toll to date, even while the mortality rate has decreased as health experts learn more about the disease.
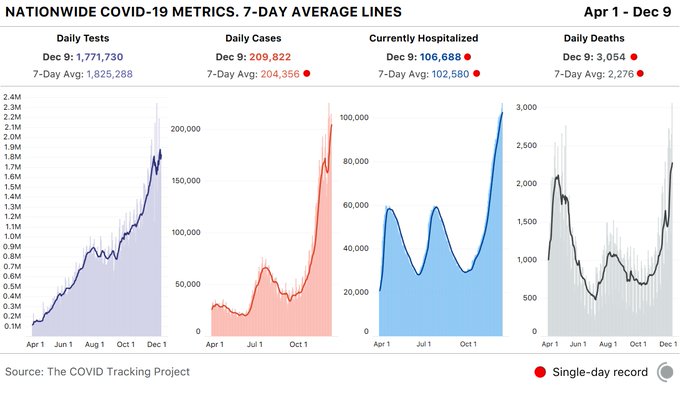
The Covid Tracking Project, which tracks state-level coronavirus data, reported 3,054 COVID-19 related deaths — a significant jump from the previous single-day record of 2,769 on May 7.
The spread of the disease has shattered another record with 106,688 COVID-19 patients in U.S. hospitals. And overall, states reported 1.8 million tests and 210,000 cases. According to the group, the spike represents more than a 10% increase in cases over the last 7 days.
Additionally, California nearly topped its single-day case record at 30,851. It is the second highest case count since December 6, the organization reported.
The staggering spike in fatalities and infections has overwhelmed hospitals and intensive care units across the nation, an increase attributed by many experts to people relaxing their precautions at Thanksgiving.
They have been at this for almost a year. While politicians argued about masks, superspreader weddings made the news, a presidential election came and went, and at least 281,000 Americans died, nurses reported for work. The Post asked seven ICU nurses what it’s been like to care for the sickest covid patients. This is what they want you to know.
As of Dec. 7, Idaho has seen 110,510 total confirmed cases, 1,035 deaths, and 477 people are currently hospitalized with the virus.
Kori Albi, 31
Covid unit intensive care nurse and unit supervisor, Saint Alphonsus Regional Medical Center
Our staff are getting sick. Our physicians are getting sick. And they’re not getting it from the hospital. They’re getting it from the community. We are almost lucky to care for the covid patients because we know who they are. Anytime we go into these rooms, we know exactly what we need to do. We have all the PPE we need. And as long as we are diligent and follow all the processes that are in place, we can keep ourselves safe. That’s not what worries me at all. Going out into the community is scarier than coming into work every day. Because you don’t know who has it.
This virus has caused this feeling, this sense of isolation. The covid unit is an isolated desert. Every door is shut. Every room has negative airflow. By the time you put your N95 mask on and then your surgical mask over the top of that, then you put your isolation gown on and your face shield on top of that, you can’t tell who is who. So much of health care is about that personal touch — now, our patients can’t even see our name badges because they are on under our gowns. All they see are our eyes through our face mask.
A lot of families are hesitant to have Zoom calls with patients because it can be uncomfortable and awkward. Especially if these patients are sedated and intubated. There’s always that awkwardness of: Can they hear you? Can they not hear you? Even as nurses, we feel like we’re talking to the wall. But we talk to them just as if they were awake. Allowing families to play their music that they like or pray with them or just talk to them can absolutely help. You see vital signs change.
One patient, all she wanted to do was have her son sing her a song. I think I spent over an hour in the room listening to him play the guitar and sing her a song. He sang her mostly hymns.
Death is a very intimate event that normally involves a lot of family members that help bring closure and that helps everyone process. In normal circumstances, health care providers form these relationships with the family at the bedside. All of that has been removed. And we now have to try to form those relationships over the telephone. It’s a traumatic experience. And it’s a long drawn-out process. A lot of people don’t make it out of here. It’s a slow, lonely death.
The amount of death with covid is profound. As nurses, we have learned to process death, but the amount of death has happened in such a short span of time — that’s what’s been overwhelming. I had a patient that we did a Zoom call with. His four-year-old granddaughter lived with him. And she brought tears to the room. The naivete of a four-year-old. Her grandfather was intubated so he couldn’t talk. But he could kind of look around the room. But the innocence of her, saying, “Come home, Pa. I miss you, Pa. I love you Pa,” all through a video screen. The 14-year-old that also lived with them couldn’t formulate words to say anything, and he didn’t know what to do or say in that video. But the four-year-old was telling Pa to come home.
JACKSON, MISS.
As of Dec. 7, Mississippi has seen 166,194 total confirmed cases, 3,961 deaths, and 1,157 people are currently hospitalized with the virus.
Catie Carrigan, 28
ICU, University of Mississippi Medical Center
There are some patients who have been in their younger 20s and their younger 30s, and I think maybe those are the hardest cases. They have families and they have kids just like I do, and it’s hard coming into work and taking care of them. Knowing they’re supposed to be going to college, they’re supposed to be getting married, they’re supposed to be having kids and, instead, they’re laying in a hospital bed on a ventilator fighting for their life.
They have their whole entire lives ahead of them, and then they get hit with this disease that everybody thinks is a hoax and then they die.
I worked in the ER a month ago, so I know exactly what’s going on down there, and now I work in the ICU, so I know exactly what’s going on on both sides of it. There are no ICU beds in the hospital. None. When there are no ICU beds, we hold them in the ER, or we hold them in the PACU (post-anesthesia care unit). The ER still has to treat our trauma patients, our car accidents, our gunshot victims. So when we have those ICU holds in the ER, it obviously makes the jobs of nurses and doctors in the ER way more difficult than it needs to be. We are treating patients in the hallway. They’re just trying to do the best they can with the resources that we have.
There is no room left, essentially, and I think that’s really what people don’t seem to understand. And I get it, when you’re not in health care you don’t really see our side of it, but we’re seeing the worst of it. It’s hard for us to convey that to the public because they don’t seem to want to take our word for it — but take our word for it. Take our word for it.
IOWA CITY
As of Dec. 7, Iowa has seen 244,844 total confirmed cases, 2,717 deaths, and 898 people are currently hospitalized with the virus.
Allison Wynes, 39
Medical intensive care unit, University of Iowa Hospitals and Clinics
I cry every day when I walk in to work, and I cry every day when I walk to my car after work.
You get it out of your system before you show up and you do your job and you’re fine. Then, you go home and you cry before you get home. And then you go home and be mom.
My 9-year-old daughter asks frequently, “Mommy, how many patients were there today? Mommy, how many sick ones were there today? Were you safe? Was everything okay? Do you have to go to work again? How many patients?” She gets it.
I think one thing that people do not appreciate is it’s not only the number or volume of patients that comes through — it’s the level of care that they require, which is so much greater than a standard patient in the ICU or a standard patient in the floor, because they can get very, very sick very quickly.
We were walking a patient who was on ECMO, which is extracorporeal membrane oxygenation, and it took five people to walk her. That’s not normal.
I work in the MICU, so it’s never like a party up in here, but it used to at least be, nine times out of ten, calm and controlled and tidy and clean. Occasionally stuff would go bad and we would all run and help, and then we would all go about our days. Now it just feels like, especially of late, there is equipment everywhere. There are gowns everywhere. There are gloves everywhere, there are people everywhere, and there are fires everywhere.
I’m actually scared, and I’ve never been scared at work before. I am scared that we will lose control.
It’s the human resources we are running low on. We can make a bed, we can find a ventilator, we have PPE. But it’s the human cost of caring for these patients that has been keeping me up at night the past couple of weeks and really making me nauseous every day.
I didn’t think it would be over by now, but I didn’t think we’d be getting hit this hard this late. I thought we’d still just be smoldering. I didn’t know that we would just be a raging fire at this point in time. We’re not prepared for that, but here we are.
After this, I’m going to take my kids to a beach or somewhere.
GLENVIEW, ILL.
As of Dec. 7, Illinois has seen 796,264 total confirmed cases, 14,216 deaths, and 5,190 people are currently hospitalized with the virus.
Luisa Alog Penepacker, 51
ICU, Glenbrook Hospital
I’ve taken care of a lot of husband-wife patients, unfortunately. One of the cases was one in which the husband had tested positive for covid first, but he was a mild case. She was a little bit more serious. She ended up on our unit.
The husband ended up in the hospital the next day, but he was on the step-down unit. When I admitted her, she was terrified, especially knowing that her husband was upstairs in another unit. She was having a hard time breathing, and she grabbed onto my hand and looked at me. She goes, “Am I gonna die?” I mean, I didn’t know what to say. And I just told her, “Not on my watch.” So we just kept on going. But unfortunately, she got intubated the next day.
Then I was sent to work upstairs on the step-down unit. I had her husband that next day, and he was actually quite happy that I saw her. He goes, “You took care of my wife, how is she? I heard that she’s not doing well.” I didn’t know what to say to him, either. I just said, “You know, she’s in the best of care. We’ll take really good care of her.” And he looked really relieved. He goes, “I’m just so glad that someone who had seen her is here now to talk to me.” And my heart broke with that.
She ended up passing. A few days after, he went home, and I didn’t see him, so I don’t know how he took it. He wasn’t able to see her before she passed.
We wear personal air purification respirators on our heads — these big white domes over our heads with a respirator hose going to a machine strapped around our waist, and we look like astronauts walking through the unit, going in and out of patients’ rooms with our plastic gowns and gloves.
It can be frightening to family members if they’re allowed to come to visit and definitely for patients because we’re kind of scary-looking. It can be frantic at times. You walk through the hall, and you see a lot of patients on ventilators. You hear a lot of beeping. People are rounding constantly to check on patients. It’s a busy place.
You don’t know what to tell family members when you see them. What can you say? You just say, “I’m sorry.” You can’t even hug them. I used to be able to hug family members, but you can’t with all the gear.
When patients are scared, I will hold their hand even though I’m wearing gloves. I look them in the eyes as much as I can because really, that’s all you can see. You can’t see our faces. You can barely even hear past the mask. So I’ll make sure to look at them. I try to make an effort to smile with my eyes and to just hold their hand if they need it.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Tammy Kocherhans, 41
Respiratory ICU, Intermountain Healthcare
These patients are different than the typical patient. They’re very complex. They can change in the blink of an eye. And it’s very hard as a nurse when you wrap your heart and soul into taking care of these patients. I started noticing that I was emotionally tired. I was physically completely exhausted. And I was beginning to question whether or not I could continue forward being a nurse at all. I was past my physical capacity.
I happened to be working a day where another health care worker who was a veteran said that this was like a combat zone, and for some reason in my head, that validated the way that I was feeling. So I reached out to one of my best friends who is a veteran, a flight medic, and he said, “I meditate and do yoga.”
Once I started doing that, I was able to handle the emotional crises, the physical pain of working so, so many long, hard hours. We do something called proning, where you take patients and flip them over onto their bellies. And that sounds really easy, but it takes a team of a minimum of five people. It is extremely taxing on your body. It hurts. And I lift weights! The meditation and yoga really has saved my life, my mental capacity, my spiritual capacity, my physical capacity, everything that is required to give to these patients.
Hopefully by 8 p.m., I’m out in the parking lot and spend a minute in my car to unload from my day. It’s all about taking a moment to breathe for myself and then going through whatever came up that day that I need to let go of. It depends on how complicated my patient was that day, whether I can let my whole day go or if I have to spend time to go through each piece and work it down to: What did I do right? Did I miss something? Sometimes I just can’t let some details go quickly, and I have to work them down to allow myself to say I did everything that I possibly could for this individual this day, in this time, in this situation. And whatever the outcome was or is, I followed protocol. I did everything that I knew how to do. And it’s going to be OK.
I find it very frustrating when I go out and about on my days off and I see people very blatantly not wearing masks or trying to tell me how come they don’t work or telling me that this pandemic isn’t real. I find it completely disrespectful to the work we do to save people’s lives, to have people think that this pandemic isn’t real, to show utter disregard for people around them, not trying to do their part.
And I really wish that I could take people on a day with me so that they can see what I see. So that they can feel your feet ache so bad that you wish they’d just fall off, because you’re on that concrete for so many hours. Your back aches because you’re wearing equipment to save your life — so that you can save somebody else’s life. And your head hurts. I’ve never had so many headaches in my life because part of the equipment sits on your head, and after 12 hours, it starts to exert so much pressure that you start to have a headache, and you’re dehydrated.
Early in the pandemic, I remember walking into this room, and this young patient was crying and asked me if they were going to die. And I’m a mom of teenagers. For me, that was awful because this patient was all alone, and we as staff were minimizing contact because we didn’t want to get the virus.
This patient started physically trembling in the bed. I couldn’t take it anymore, and I went over and just held this patient because that’s what I’d want somebody to do for my children. That was my first patient that I held like that. And there have been many since.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Nate Smithson, 28
Respiratory ICU, IntermountainHealthcare
A few weeks ago, my wife and I were on a date at a restaurant. And in the middle of nowhere, I had this panic attack and went and hid in the bathroom stall for half an hour. I have no idea what brought it on. I just couldn’t handle being there right then, which was weird for me. That’s the first time anything like that has happened. But since then, it’s happened multiple times, where the anxiety and stress is overwhelming, and I can’t handle it. So I have to go and excuse myself for a little bit.
Balancing work and life is something that used to seem possible. Now it doesn’t seem like there is any difference between the two. I fall asleep and I dream about my patients.
When we got our first covid patient in February in the hospital, in the ICU, we all kind of thought it was a little bit of a joke, to be honest. I had this patient, and he was sitting there with minimal amounts of oxygen in the room just watching TV. He’s like, “I’m fine. I don’t know why everyone’s freaking out about this.” And I thought the same thing. And then a few hours later, he stands to go pee, and I’m looking at his monitor. And it drops down to the low 90s. Ninety-two is about as low as you want to go. And then it starts dropping down lower, to about the 70s. Then it gets down into the 60s and 50s. And that’s dangerous territory. That’s where brain cells start dying and you start having some serious problems.
I run into the room. We get him back into bed and throw all the oxygen that we have in the room on him, crank everything up, and he’s not recovering from it. We had to intubate right then and there. And about an hour later, he finally starts recovering a little bit. But at this point, he’s sedated, he’s on the ventilator. Everything is worse. And that’s the first time where it’s like: Oh, crap, this is serious. This is something else. I’ve never seen anything like that before.
If a patient’s heart stops or if they stop breathing, we call a code blue, and that’s when the doctor, respiratory therapist, nurses, everybody comes into the room. We start chest compressions or CPR or that kind of stuff. This one patient’s heart is not working. So I call the code blue. We all get in there. We start doing the chest compressions. Five minutes later, we get the patient back. We all go back about our work. Twenty minutes later, same thing happens again. We start doing the chest compressions. We start pushing medications as fast as we can to get the patient back again.
The spouse comes into the hospital. I explain: “Just so you know, this is what happened before. It could possibly happen again. If it does, I’m going to need you to step outside of the room.” And as I’m explaining this, sure enough, it happens again. We lose the pulse. We lose the heartbeat. So I ask her to leave the room. Everyone gets in there, and we start going for it. We went for almost two hours: chest compressions, pushing medications, shocking the patient’s heart.
The doctor is ultimately the one who makes the decision about when we stop, and they call time of death. But typically in situations like that, where it’s unexpected and sudden, they want to make sure that everybody can go home that night feeling OK about what they did, knowing that they did everything. And after an hour, he stops, turns to the room and asks: Does anyone have a problem with us stopping?
I didn’t have a problem, but then as he’s saying that, I look out the window, and the patient’s wife is just watching us. She’s been sitting out there watching us for an hour, and no one’s saying anything.
And I ask them to keep going.
So we did. We went almost for another hour after that, and we didn’t get the patient back. He ended up dying.
But I think for me, that was important — to keep going. Not because we thought we would get them back, but so that his wife would know that we did everything we could.
I still go to bed with her face kind of burned into my mind, of just seeing her sitting out there watching us, and that’s what kills me.
COLUMBUS, OHIO
As of Dec. 7, Ohio has seen 475,024 total confirmed cases and 6,959 deaths.
Kahlia Anderson, 32
ICU, Ohio State University Wexner Medical Center
I graduated from nursing school in May 2019. I started here at the Wexner in August. Our orientation is a 20-week program, and so I came out on my own Jan. 12, 2020. The pandemic hit us at the end of February.
In nursing school, I think your biggest fears are making med errors, or harming your patient in some way, or just not knowing how to do everything. Did I check my patient’s blood pressure before I gave this blood pressure medication, or did I give the correct dose of a specific medication? I had heard stories about that on the unit, like make sure you’re careful with the needle stick, or make sure you’re careful with this medication. And I don’t even think about those kinds of things anymore.
Now it’s the fear of the unknown. It’s the fear that anything could happen because of this virus and my patient could die regardless of what I do.
When I got my first covid-positive patient, I remember thinking: Somebody did the assignment wrong because there’s no way that they believe that I should be taking care of this patient. I can remember the feeling. I can remember the day. It was a weekend. I was on a day shift. And I was thinking to myself: Who trusted me, the new nurse to take care of a covid-positive patient? How am I going to do this? How am I going to keep this patient safe? How am I going to keep myself safe? Am I safe? Wait, who cares about me? Let’s get back to the patient. What do they need?
At the time, I didn’t even understand some of the ventilator settings because I was still that new, and it was still that fresh to me. And I thought: This machine is doing that much work for them, and I don’t know enough about it, but I’m going to make sure that I get it done and I’m going to figure it out today to make sure that this patient gets everything that they need. And I’m going to call their family and double check with them and check in with them and call them.
That patient is alive. That patient is no longer in the hospital. As far as I know, that patient is home and safe with family.
I would feel like: There’s someone more experienced. There’s someone more adequate to deal with this. And I was like — oh, it’s me. This is me, I’m doing this, and I’ve been doing it ever since.
I saw new nurses come out of orientation, and I saw the type of assignments that they would get. So my mind fixated on like: I’m going to get patients that are ready to transfer out. They can talk, they can eat. They’re just waiting for a bed on another unit. Or maybe it’s a patient who needs long-term care. So they’re waiting to go to a facility to be discharged. And so I was thinking to myself: I’m going to get my feet wet. It’s going to be great. I’m going to build up this experience, and then I’m going to start getting sicker patients, and I’m going to be ready.
Once covid hit, there was no room for those types of patients anymore. Everyone had covid, everyone was sick, everyone was intubated or approaching intubation.
And for me, I just wanted my first experience. I wanted to have the simple experience of building and getting better. But that’s not what was in store. And I can’t say that I’m upset about it today. I’m grateful for this experience. I don’t wish this pandemic on anyone. I wish it was not here. I wish that it was different. But as a nurse, as a new nurse, these experiences are unique to me. It’s making me a better nurse. It’s made me a better person, and I can only continue to just be.
We did cry in the beginning, and now not so much. I think we all struggled when we had a young death. Someone in their 20s was very difficult for us. Because you think: That was a young life. What a young life that was, and they’re not here anymore. Because of a virus. That’s hard. It’s very hard.