Published this week in the Washington Post, this unsparing article packages a year of investigative reporting into a thorough accounting of why US life expectancy is undergoing a rapid decline.
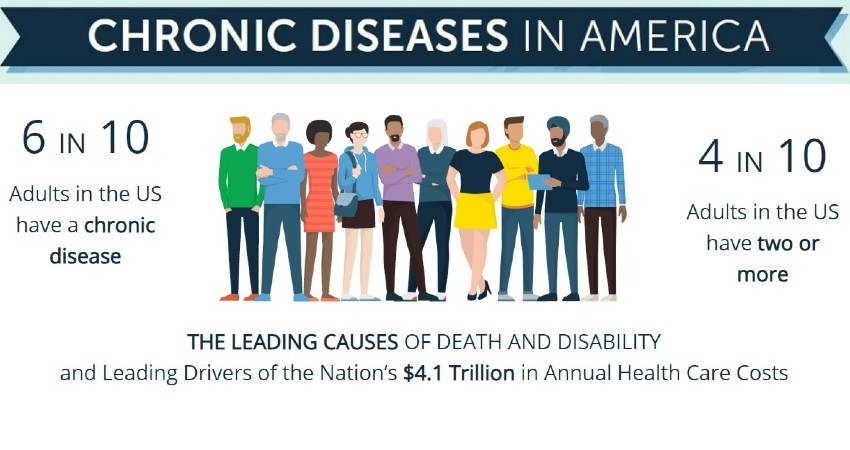
After peaking in 2014, US life expectancy has declined each subsequent year, trending far worse than peer countries. In a quarter of US counties, working-age Americans are dying at the highest rates in 40 years, reversing decades of progress. While deaths from firearms and opioids play a role, chronic diseases remain our nation’s greatest killer, erasing more than double the years of life as all overdoses, homicides, suicides, and car accidents combined.
The drivers of this trend are too numerous to list, but experts suggest targeting “the causes of the causes”, namely social factors, as the death rate gap between the rich and poor has grown almost 15x faster than the income gap since 1980.
The Gist: This reporting is a sobering reminder of the responsibilities—and failures—borne by our nation’s healthcare system.
The massive death toll of chronic disease in this country is not an indictment of the care Americans receive, but of the care and other resources they cannot access or afford.
While it’s not the mandate of health systems to reduce systemic issues like poverty, there is no solution to the problem without health systems playing a key role in increasing access to care, while convening community resources in service of these larger goals.
Saturday, Congress voted overwhelming (House 335-91, Senate 88-9) to keep the government funded until Nov. 17 at 2023 levels. No surprise. Congress is supposed to pass all 12 appropriations bills before the start of each fiscal year but has done that 4 times since 1970—the last in 1997. So, while this chess game plays out, the health system will soldier on against growing recognition it needs fixing.
In Wednesday night’s debate, GOP Presidential aspirant Nicki Haley was asked what she would do to address the spike in personal bankruptcies due to medical debt. Her reply:
“We will break all of it [down], from the insurance company, to the hospitals, to the doctors’ offices, to the PBMs [pharmacy benefit managers], to the pharmaceutical companies. We will make it all transparent because when you do that, you will realize that’s what the problem is…we need to bring competition back into the healthcare space by eliminating certificate of need systems… Once we give the patient the ability to decide their healthcare, deciding which plan they want, that is when we will see magic happen, but we’re going to have to make every part of the industry open up and show us where their warts are because they all have them”
It’s a sentiment widely held across partisan aisles and in varied degrees among taxpayers, employers and beyond. It’s a system flaw and each sector is complicit.
What seems improbable is a solution that rises above the politics of healthcare where who wins and loses is more important than the solutions themselves.
Perhaps as improbable as the European team’s dominating performance in the 44th Ryder Cup Championship played in Rome last week especially given pre-tournament hype about the US team.
While in Rome last week, I queried hotel employees, restaurant and coffee shop owners, taxi drivers and locals at the tournament about the Italian health system. I saw no outdoor signage for hospitals and clinics nor TV ads for prescriptions and OTC remedies. Its pharmacies, clinics and hospitals are non-descript, modest and understated. Yet groups like the World Health Organization (WHO) and the Organization for Economic Cooperation Development (OECD) rank Servizio Sanitario Nazionale (SSN), the national system authorized in December 1978, in the top 10 in the world (The WHO ranks it second overall behind France).
“It covers all Italian citizens and legal foreign residents providing a full range of healthcare services with a free choice of providers. The service is free of charge at the point of service and is guided by the principles of universal coverage, solidarity, human dignity, and health. In principle, it serves as Italy’s public healthcare system.” Like U.S. ratings for hospitals, rankings for the Italian system vary but consistently place it in the top 15 based on methodologies comparing access, quality, and affordability.
The U.S., by contrast, ranks only first in certain high-end specialties and last among developed systems in access and affordability.
Like many systems of the world, SSN is governed by a national authority that sets operating principles and objectives administered thru 19 regions and two provinces that deliver health services under an appointed general manager. Each has significant independence and the flexibility to determine its own priorities and goals, and each is capitated based on a federal formula reflecting the unique needs and expected costs for that population’s health.
It is funded throughnational and regional taxes, supplemented by private expenditure and insurance plans and regions are allowed to generate their own additional revenue to meet their needs. 74% of funding is public; 26% is private composed primarily of consumer out-of-pocket costs. By contrast, the U.S. system’s funding is 49% public (Medicare, Medicaid et al), 24% private (employer-based, misc.) and 27% OOP by consumers.
Italians enjoy the 6th highest life expectancy in the world, as well as very low levels of infant mortality. It’s not a perfect system: 10% of the population choose private insurance coverage to get access to care quicker along with dental care and other benefits. Its facilities are older, pharmacies small with limited hours and hospitals non-descript.
But Italians seem satisfied with their system reasoning it a right, not a privilege, and its absence from daily news critiques a non-concern.
Issues confronting its system—like caring for its elderly population in tandem with declining population growth, modernizing its emergency services and improving its preventive health programs are understood but not debilitating in a country one-fifth the size of the U.S. population.
My take:
Italy spends 9% of its overall GDP on its health system; the $4.6 trillion U.S spends 18% in its GDP on healthcare, and outcomes are comparable. Our’s is better known but their’s appears functional and in many ways better.
Should the U.S.copy and paste the Italian system as its own? No. Our societies, social determinants and expectations vary widely. Might the U.S. health system learn from countries like Italy? Yes.
Questions like these merit consideration:
Might the U.S. system perform better if states had more authority and accountability for Medicare, CMS, Veterans’ health et al?
Might global budgets for states be an answer?
Might more spending on public health and social services be the answer to reduced costs and demand?
Might strict primary care gatekeeping be an answer to specialty and hospital care?
Might private insurance be unnecessary to a majority satisfied with a public system?
Might prices for prescription drugs, hospital services and insurance premiums be regulated or advertising limited?
Might employers play an expanded role in the system’s accountability?
Can we afford the system long-term, given other social needs in a changing global market?
Comparisons are constructive for insights to be learned. It’s true in healthcare and professional golf. The European team was better prepared for the Ryder Cup competition. From changes to the format of the matches, to pin placements and second shot distances requiring precision from 180-200 yards out on approach shots: advantage Europe. Still, it was execution as a team that made the difference in its dominating 16 1/2- 11 1/2 win —not the celebrity of any member.
The time to ask and answer tough questions about the sustainability of the U.S. system and chart a path forward. A prepared, selfless effort by a cross-sector Team Healthcare USA is our system’s most urgent need. No single sector has all the answers, and all are at risk of losing.
Team USA lost the Ryder Cup because it was out-performed by Team Europe: its data, preparation and teamwork made the difference.
Today, there is no Team Healthcare USA: each sector has its stars but winning the competition for the health and wellbeing of the U.S. populations requires more.
Albert Einstein determined that time is relative. And when it comes to healthcare, five years can be both a long and a short amount of time.
In August 2018, I launched the Fixing Healthcare podcast. At the time, the medium felt like the perfect auditory companion to the books and articles I’d been writing. By bringing on world-renowned guests and engaging in difficult but meaningful discussions, I hoped the show would have a positive impact on American medicine. After five years and 100 episodes, now is an opportune time to look back and examine how healthcare has improved and in what ways American medicine has become more problematic.
Here’s a look at the good, the bad and the ugly since episode one of Fixing Healthcare:
The Good
Drug breakthroughs and government actions headline medicine’s biggest wins over the past five years.
At first, health experts expressed doubts that Pfizer, Moderna and others could create a safe and effective Covid-19 vaccine with messenger RNA (mRNA) technology. After all, no one had succeeded in more than two decades of trying.
Thanks in part to Operation Warp Speed, the government-funded springboard for research, our nation produced multiple vaccines within less than a year. Previously, the quickest vaccine took four years to develop (mumps). All others required a minimum of five years.
The vaccines were pivotal in ending the coronavirus pandemic, and their success has opened the door to other life-saving drugs, including those that might prevent or fight cancer. And, of course, our world is now better prepared for when the next viral pandemic strikes.
Weight-Loss Drugs
Originally designed to help patients manage Type 2 diabetes, drugs like Ozempic have been helping people reverse obesity—a condition closely correlated with diabetes, heart disease and cancer.
For decades, America’s $150 billion a year diet industry has failed to curb the nation’s continued weight gain. So too have calls for increased exercise and proper nutrition, including restrictions on sugary sodas and fast foods.
In contrast, these GLP-1 medications are highly effective. They help overweight and obese people lose 15 to 25 pounds on average with side effects that are manageable for nearly all users.
The biggest stumbling block to their widespread use is the drug’s exorbitant price (upwards of $16,000 for a year’s supply).
Drug-Pricing Laws
With the Inflation Reduction Act of 2022, Congress took meaningful action to lower drug prices, a move the CBO estimates would reduce the federal deficit by $237 billion over 10 years.
It’s a good start. Americans today pay twice as much for the same medications as people in Europe largely because of Congressional legislation passed in 2003.
That law, the Medicare Prescription Drug Price Negotiation Act, made it illegal for Health and Human Services (HHS) to negotiate drug prices with manufacturers—even for the individuals publicly insured through Medicare and Medicaid.
Now, under provisions of the new Inflation Reduction Act, the government will be able to negotiate the prices of 10 widely prescribed medications based on how much Medicare’s Part D program spends. The lineup is expected to include prescription treatments for arthritis, cancer, asthma and cardiovascular disease. Unfortunately, the program won’t take effect until 2026. And as of now, several legal challenges from both drug manufacturers and the U.S. Chamber of Commerce are pending.
The Bad
Spiking costs, ongoing racial inequalities and millions of Americans without health insurance make up three disappointing healthcare failures of the past five years.
Cost And Quality
The U.S. spends nearly twice as much on healthcare per citizen as other countries, yet our nation lags 10 of the wealthiest countries in medical performance and clinical outcomes. As a result, Americans die younger and experience more complications from chronic diseases than people in peer nations.
As prices climb ever-higher, at least half of Americans can’t afford to pay their out-of-pocket medical bills, which remain the leading cause of U.S. bankruptcy. And with rising insurance premiums alongside growing out-of-pocket expenses, more people are delaying their medical care and rationing their medications, including life-essential drugs like insulin. This creates a vicious cycle that will likely prolong today’s healthcare problems well into the future.
Health Disparities
Inequalities in American medicine persist along racial lines—despite action-oriented words from health officials that date back decades.
Today, patients in minority populations receive unequal and inequitable medical treatment when compared to white patients. That’s true even when adjusting for differences in geography, insurance status and socioeconomics.
Racism in medical care has been well-documented throughout history. But the early days of the Covid-19 pandemic provided several recent and deadly examples. From testing to treatment, Black and Latino patients received both poorer quality and less medical care, doubling and even tripling their chances of dying from the disease.
The problems can be observed across the medical spectrum. Studies show Black women are still less likely to be offered breast reconstruction after mastectomy than white women. Research also finds that Black patients are 40% less likely to receive pain medication after surgery. Although technology could have helped to mitigate health disparities, our nation’s unwillingness to acknowledge the severity of the problem has made the problem worse.
Uninsurance
Although there are now more than 90 million Americans enrolled in Medicaid, there are still 30 million people without any health insurance. This disturbing reality comes a full decade after the passage of the Affordable Care Act.
On Capitol Hill, there is no plan in place to reduce the number of uninsured.
Moreover, many states are looking to significantly rollback their Medicaid enrollment in the post-Covid era. Kaiser Family Foundation estimates that between 8 million and 24 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provisions implemented during the pandemic. Without coverage, people have a harder time obtaining the preventive services they need and, as a result, they suffer more chronic diseases and die younger.
The Ugly
An overall decrease in longevity, along with higher maternal mortality and a worsening mental-health crisis, comprise the greatest failures of U.S. healthcare over the past five years.
Life Expectancy
Despite radical advances in medical science over the past five years, American life expectancy is back to where it was at the turn of the 20th century, according to CDC data.
Alongside environmental and social factors are a number of medical causes for the nation’s dip in longevity. Research demonstrated that many of the 1 million-plus Covid-19 deaths were preventable. So, too, was the nation’s rise in opioid deaths and teen suicides.
Regardless of exact causation, Americans are living two years less on average than when we started the Fixing Healthcare podcast five years ago.
Maternal Mortality
Compared to peer nations, the United States is the only country with a growing rate of mothers dying from childbirth. The U.S. experiences 17.4 maternal deaths per 100,000 live births. In contrast, Norway is at 1.8 and the Netherlands at 3.0.
The risk of dying during delivery or in the post-partum period is dramatically higher for Black women in the United States. Even when controlling for economic factors, Black mothers still suffer twice as many deaths from childbirth as white women.
And with growing restrictions on a woman’s right to choose, the maternal mortality rate will likely continue to rise in the United States going forward.
Mental Health
Finally, the mental health of our country is in decline with rates of anxiety, depression and suicide on the rise.
These problems were bad prior to Covid-19, but years of isolation and social distancing only aggravated the problem. Suicide is now a leading cause of death for teenagers. Now, more than 1 in every 1,000 youths take their own lives each year. The newest data show that suicides across the U.S. have reached an all-time high and now exceed homicides.
Even with the expanded use of telemedicine, mental health in our nation is likely to become worse as Americans struggle to access and afford the services they require.
The Future
In looking at the three lists, I’m reminded of a baseball slugger who can occasionally hit awe-inspiring home runs but strikes out most of the time. The crowd may love the big hitter and celebrate the long ball, but in both baseball and healthcare, failing at the basics consistently results in more losses than wins.
Over the past five years, American medicine has produced a losing record. New drugs and surgical breakthroughs have made headlines, but the deeper, more systemic failures of American healthcare have rarely penetrated the news cycle.
If our nation wants to make the next five years better and healthier than the last five, elected officials and healthcare leaders will need to make major improvements. The steps required to do so will be the focus of my next article.
After 18 years as CEO in Kaiser Permanente, I set my sights on improving the heatlh of the nation, hoping to find a way to achieve the same quality, technology and affordability our medical group delivered to 5 million patients on both coasts.
That quest launched the Fixing Healthcare podcast in 2018, and it inspired interviews with dozens of leaders, thinkers and doers, both in and around medicine. These experts shared innovative ideas and proven solutions for achieving (a) superior quality, (b) improved patient access, (c) lower overall costs, and (d) greater patient and clinician satisfaction.
Which of the hundreds of ideas presented remain most promising?
Why, after five years and so many excellent solutions, has our nation experienced such limited improvements in healthcare?
And finally, how will these great ideas become reality?
To answer the first question, I offer 15 of the best Fixing Healthcare recommendations so far. Some quotes have been modified for clarity with links to all original episodes (and transcripts) included.
Fixing the business of medicine
1. Malcolm Gladwell, journalist and five-time bestselling author: “In other professions, when people break rules and bring greater economic efficiency or value, we reward them. In medicine, we need to demonstrate a consistent pattern of rewarding the person who does things better.”
2. Richard Pollack, CEO of the American Hospital Association (AHA): “I hope in 10 years we have more integrated delivery systems providing care, not bouncing people around from one unconnected facility to the next. I would hope that we’re in a position where there’s a real focus on ensuring that people get care in a very convenient way.”
Eliminating burnout
3. Zubin Damania, aka ZDoggMD, hospitalist and healthcare satirist: “In the culture of medicine, specialists view primary care as the weak medical students, the people who couldn’t get the board scores or rotation honors to become a specialist. Because why would you do primary care? It’s miserable. You don’t get paid enough. It’s drudgery. We must change these perceptions.”
4. Devi Shetty, India’s leading heart surgeon and founder of Narayana Health: “When you strive to work for a purpose, which is not about profiting yourself, the purpose of our action is to help society, mankind on a large scale. When that happens, cosmic forces ensure that all the required components come in place and your dream becomes a reality.”
5. Jonathan Fisher, cardiologist and clinician advocate: “The problem we’re facing in healthcare is that clinicians are all siloed. We may be siloed in our own institution thinking that we’re doing it best. We may be siloed in our own specialty thinking that we’re better than others. All of these divides need to be bridged. We need to begin the bridging.”
Making medicine equitable
6. Jen Gunter, women’s health advocate and “the internet’s OB-GYN”: “Women are not listened to by doctors in the way that men are. They have a harder time navigating the system because of that. Many times, they’re told their pain isn’t that serious or their bleeding isn’t that heavy. We must do better at teaching women’s health in medicine.”
7. Amanda Calhoun, activist, researcher and anti-racism educator: “A 2015 survey showed that white residents and medical students still thought Black people feel less pain, which is wild to me because Black is a race. It’s not biological. This is actually an historical belief that persists. One of the biggest things we can do as the medical system is work on rebuilding trust with the Black community.”
Addressing social determinants of health
8. Don Berwick, former CMS administrator and head of 100,000 Lives campaign: “We know where the money should go if we really want to be a healthy nation: early childhood development, workplaces that thrive, support to the lonely, to elders, to community infrastructures like food security and transportation security and housing security, to anti-racism and criminal-justice reform. But we starve the infrastructures that could produce health to support the massive architecture of intervention.”
9. David T. Feinberg, chairman of Oracle Health: “Twenty percent of whether we live or die, whether we have life in our years and years in our life, is based on going to good doctors and good hospitals. We should put the majority of effort on the stuff that really impacts your health: your genetic code, your zip code, your social environment, your access to clean food, your access to transportation, how much loneliness you have or don’t have.”
Empowering patients
10. Elisabeth Rosenthal, physician, author and editor-in-chief of KHN: “To patients, I say write about your surprise medical bills. Write to a journalist, write to your local newspaper. Hospitals today are very sensitive about their reputations and they do not want to be shamed by some of these charges.”
11. Gordon Chen, ChenMed CMO: “If you think about what leadership really is, it’s influence. Nothing more, nothing less. And the only way to achieve better health in patients is to get them to change their behaviors in a positive way. That behavior change takes influence. It requires primary care physicians to build relationship and earn trust with patients. That is how both doctors and patients can drive better health outcomes.”
Utilizing technology
12. Vinod Khosla, entrepreneur, investor, technologist: “The most expensive part of the U.S. healthcare system is expertise, and expertise can relatively be tamed with technology and AI. We can capture some of that expertise, so each oncologist can do 10 times more patient care than they would on their own without that help.”
13. Rod Rohrich, influential plastic surgeon and social media proponent: “Doctors, use social media to empower your audience, to educate them, and not to overwhelm them. If you approach social media by educating patients about their own health, how they can be better, how can they do things better, how they can find doctors better, that’s a good thing.”
Rethinking medical education
14. Marty Makary, surgeon and public policy researcher: “I would get rid of all the useless sh*t we teach our medical students and residents and fellows. In the 16 years of education that I went through, I learned stuff that has nothing to do with patient care, stuff that nobody needs to memorize.”
15. Eric Topol, cardiologist, scientist and AI expert: “It’s pretty embarrassing. If you go across 150 medical schools, not one has AI as a core curriculum. Patients will get well versed in AI. It’s important that physicians stay ahead, as well.”
Great ideas, but little progress
Since 2018, our nation has spent $20 trillion on medical care, navigated the largest global pandemic in a century and developed an effective mRNA vaccine, nearly from scratch. And yet, despite all this spending and scientific innovation, American medicine has lost ground.
American life expectancy has dropped while maternal mortality rates have worsened. Clinician burnout has accelerated amid a growing shortage of primary care and emergency medicine physicians. And compared to 12 of its wealthiest global peers, the United States spends nearly twice as much per person on medical care, but ranks last in clinical outcomes.
Guests on Fixing Healthcare generally agree on the causes of stagnating national progress.
Healthcare system giants, including those in the drug, insurance and hospital industries, find it easier to drive up prices than to prevent disease or make care-delivery more efficient. Over the past decade, they’ve formed a conglomerate of monopolies that prosper from the existing rules, leaving them little incentive to innovate on behalf of patients. And in this era of deep partisan divide, meaningful healthcare reforms have not (and won’t) come from Congress.
Then who will lead the way?
Industry change never happens because it should. It happens when demand and opportunity collide, creating space for new entrants and outsiders to push past the established incumbents. In healthcare, I see two possibilities:
1. Providers will rally and reform healthcare
Doctors and hospitals are struggling. They’re struggling with declining morale and decreasing revenue. Clinicians are exiting the profession and hospitals are shuttering their doors. As the pain intensifies, medical group leaders may be the ones who decide to begin the process of change.
The first step would be to demand payment reform.
Today’s reimbursement model, fee-for-service, pays doctors and hospitals based on the quantity of care they provide—not the quality of care. This methodology pushes physicians to see more patients, spend less time with them, and perform ever-more administrative (billing) tasks. Physicians liken it to being in a hamster wheel: running faster and faster just to stay in place.
Instead, providers of care could be paid by insurers, the government and self-funded businesses directly, through a model called “capitation.” With capitation, groups of providers receive a fixed amount of money per year. That sum depends on the number of enrollees they care for and the amount of care those individuals are expected to need based on their age and underlying diseases.
This model puts most of the financial risk on providers, encouraging them to deliver high-quality, effective medical care. With capitation, doctors and hospitals have strong financial incentives to prevent illnesses through timely and recommended preventive screenings and a focus on lifestyle-medicine (which includes diet, exercise and stress reduction). They’re rewarded for managing patients’ health and helping them avoid costly complications from chronic diseases, such as heart attacks, strokes and cancer.
Capitation encourages doctors from all specialties to collaborate and work together on behalf of patients, thus reducing the isolation physicians experience while ensuring fewer patients fall through the cracks of our dysfunctional healthcare system. The payment methodology aligns the needs of patients with the interests of providers, which has the power to restore the sense of mission and purpose medicine has lost.
Capitation at the delivery-system level eliminates the need for prior authorization from insurers (a key cause of clinician burnout) and elevates the esteem accorded to primary care doctors (who focus on disease prevention and care coordination). And because the financial benefits are tied to better health outcomes, the capitated model rewards clinicians who eliminate racial and gender disparities in medical care and organizations that take steps to address the social determinants of health.
2. Major retailers will take over
If clinicians don’t lead the way, corporate behemoths like Amazon, CVS and Walmart will disrupt the healthcare system as we know it. These retailers are acquiring the insurance, pharmacy and direct-patient-care pieces needed to squeeze out the incumbents and take over American healthcare.
Each is investing in new ways to empower patients, provide in-home care and radically improve access to both in-person and virtual medicine. Once generative AI solutions like ChatGPT gain enough computing power and users, tech-savvy retailers will apply this tool to monitor patients, enable healthier lifestyles and improve the quality of medical care compared to today.
When Fixing Healthcare debuted five years ago, none of the show’s guests could have foreseen a pandemic that left more than a million dead. But, had our nation embraced their ideas from the outset, many of those lives would have been saved. The pandemic rocked an already unstable and underperforming healthcare system. Our nation’s failure to prevent and control chronic disease resulted in hundreds of thousands of unnecessary deaths from Covid-19. Outdated information technology systems, medical errors and disparities in care caused hundreds of thousands more. As a nation, we could have done much better.
With the cracks in the system widening and the foundation eroding, disruption in healthcare is inevitable. What remains to be seen is whether it will come from inside or outside the U.S. healthcare system.
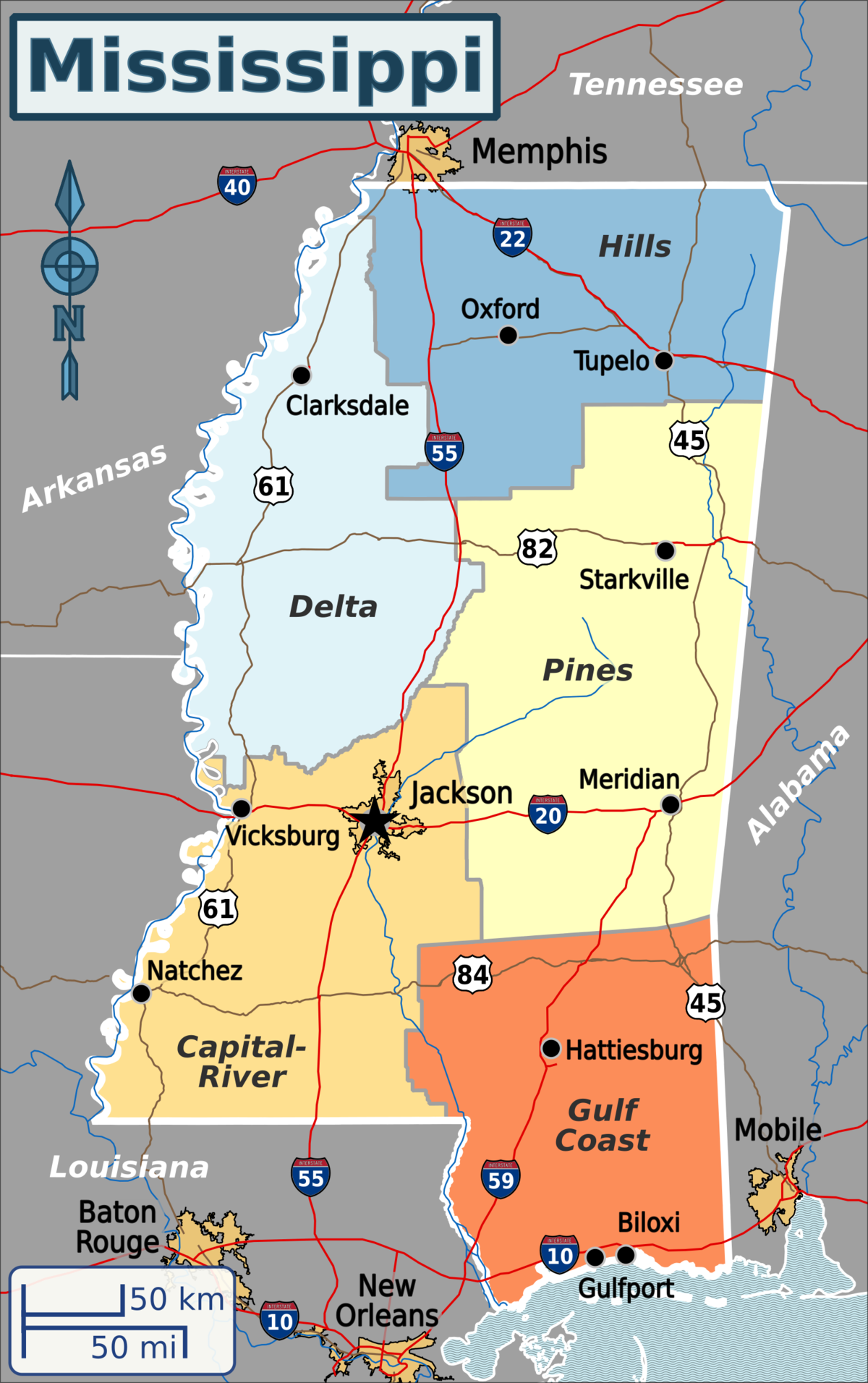
Published this week in the New York Times, this article describes the decaying state of Greenwood Leflore Hospital, a 117 year-old facility in the Mississippi Delta that may be within months of closure. While rural hospitals across the country are struggling, Mississippi’s firm opposition to Medicaid expansion has exacerbated the problem in that state, by depriving providers of an additional $1.4B per year in federal funds. Instead, only a few of the state’s 100-plus hospitals actually turn an annual profit, and uncompensated care costs are almost 10 percent of the average hospital’s operating costs.
Despite a dozen or more hospitals at imminent risk of closure, Mississippi officials would rather use the state’s $3.9B budget surplus to lower or eliminate the state income tax.
The Gist:Expanding Medicaid doesn’t just reduce rates of uncompensated care provided by hospitals, it changes the volume and type of care they provide.
Further, Medicaid expansion has been found to result in significant reductions in all-cause mortality.
Ensuring that low-income residents in Mississippi and other non-expansion states have access to Medicaid would allow providers to administer more preventive care and manage chronic diseases more effectively, before costly exacerbations require hospitalization.
Even as new omicron strains take over, Covid is no longer driving a majority of patients into the hospital. Still, doctors worry the virus could re-emerge as immunity wanes.
As the flu and RSV (respiratory syncytial virus) have spread rapidly this fall — inundating and overwhelming hospitals and their staff across the country — Covid has not.
In fact, Covid-related deaths and hospitalizations have fallen in recent months,despite the emergence of new omicron subvariants that evade immunity from previous infections and vaccination.
According to NBC News data, Covid deaths have fallen consistently since Aug. 31, when the seven-day average of daily Covid deaths was at 571. A month later, on Sept. 30, the number fell to 475. By Halloween, 365 were dying per day, on average, from Covid.
As of Nov. 14, the number had fallen to 316.
This week, the Centers for Disease Control and Prevention is expected to release new data on Covid-related mortality, finding that death rates began to decline in March 2022.
The overall hopeful sign of declining deaths could indicate yet another new Covid phase, doctors suggest. Fewer people sick enough to be hospitalized with Covid means that fewer people are dying of the illness.
The average number of Covid hospitalizations per day has decreased by 27.9% since Aug. 28, according to NBC News data.
Even better, Covid, it seems, is no longer sending a majority of patients into intensive care units.
“There has not been an increase in patients admitted to the hospital specific for Covid-related disease,” said Dr. Hugh Cassiere, director of critical care services at Sandra Atlas Bass Heart Hospital at North Shore University Hospital, part of Northwell Health in New York City.
Patients in his ICU with Covid were admitted with unrelated medical issues, and were subsequently found to be Covid-positive, Cassiere said.
“Not to say that it’s gone, but Covid has become a coincidental disease,” he said.
Dr. Vin Gupta, a pulmonologist and an affiliate faculty member at the University of Washington in Seattle, attributes the decline in deaths and severe Covid cases to a level of “baked-in immunity,” including vaccination, prior infection or a combination of the two.
While Covid-related hospitalizations are not currently increasing, Gupta warns that they could during the winter as immunity, especially from previous infection, diminishes.
“If you had Covid, say six to four months ago, you’re going to have less protection against hospitalization than if you were vaccinated,” Gupta said. “The duration and the robustness of protection wanes a lot more quickly if all you rely on is natural immunity.”
With that in mind, data from the Institute for Health Metrics and Evaluation, a research center within the University of Washington, suggest that Covid hospitalizations and deaths could tick up again in “mid-January at the earliest,” said Gupta, a medical analyst for NBC News and MSNBC.
Despite the encouraging decline in Covid deaths, another school of thought suggests that Covid has simply morphed into a new kind of fatal illness.
“Before everyone was vaccinated or had been infected, 80 or 90% of Covid looked exactly same. They had terrible pneumonia. They were in the ICU on respiratory support,” said Dr. Jeremy Faust, an emergency medicine physician at Brigham and Women’s Hospital and an instructor at Harvard Medical School in Boston.
Now, he said, “Covid deaths don’t all look the same.” While “baked-in immunity” may keep the most severe cases at a minimum, it is clear that Covid can wreak havoc on the body long after the infection has cleared.
“Somebody could have Covid and have a heart attack, and the primary cause of death is listed as a heart attack because that’s what really brought them to the hospital,” Faust said.
But, he added, “we’ll never know to what degree Covid triggered that heart attack.”
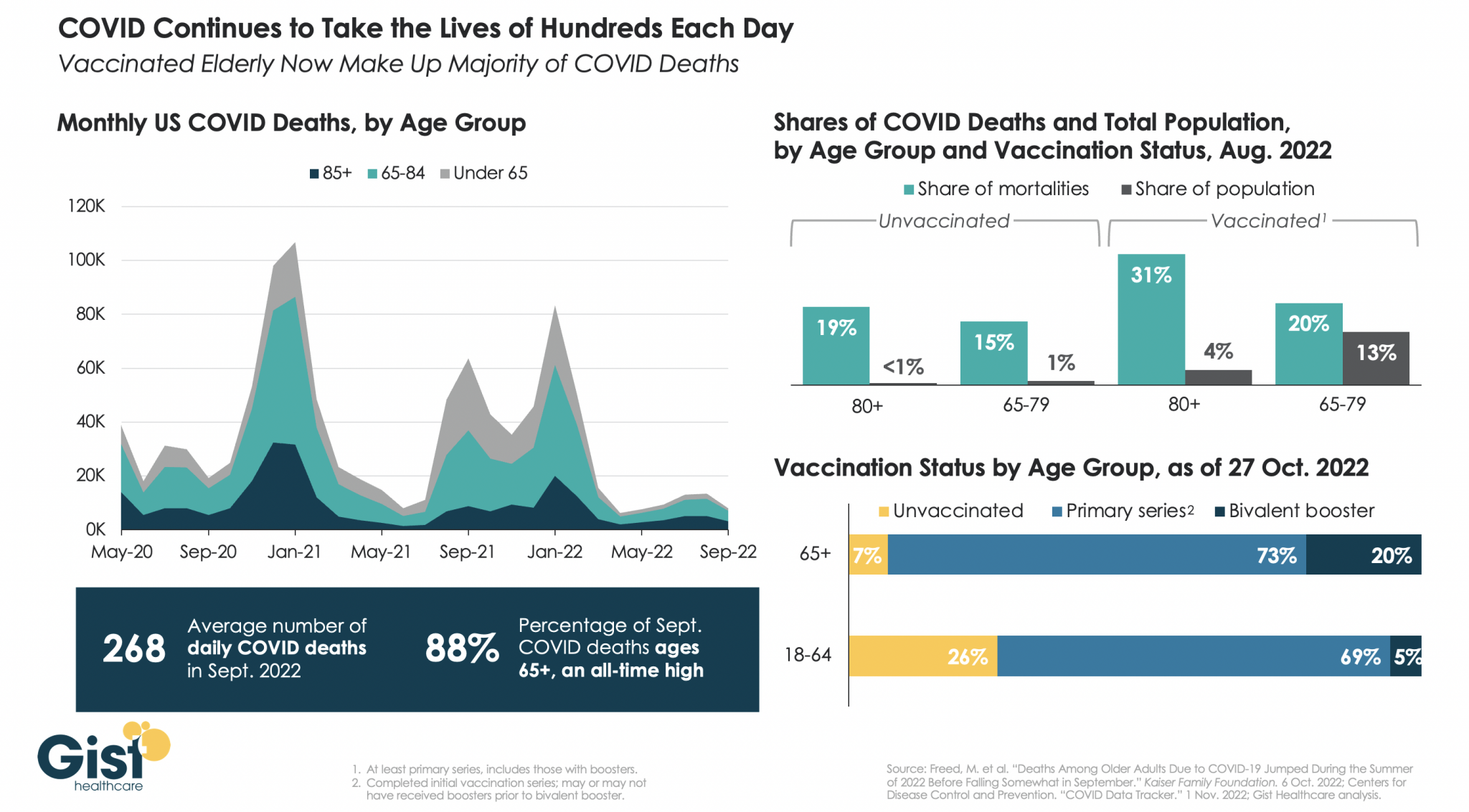
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
Figure. Excess deaths in the U.S. relative to other wealthy nations, 1933-2021. Source: Human Mortality Database. Note: Figure shows the difference between the number of deaths that occurred in the U.S. each year and the number of deaths that would have occurred if the U.S. had age-specific mortality rates equal to the average of other wealthy nations. The comparison set includes Austria, Belgium, Canada, Denmark, Finland, France, Germany, Iceland, Italy, Japan, Luxembourg, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the United Kingdom. The average of other wealthy nations excludes Portugal prior to 1940, Austria and Japan prior to 1947, Germany prior to 1956, and Luxembourg prior to 1960. From 1960, all countries are represented (solid dots).
COVID-19 led to a large increase in U.S. deaths. However, even before the pandemic, the U.S. had higher death rates than other wealthy nations. How many deaths could be avoided if the U.S. had the same mortality rates as its peers?
In a new study, we quantify the annual number of U.S. deaths that would have been averted over nearly a century if the U.S. had age-specific mortality rates equal to the average of 18 similarly wealthy nations. We refer to these excess U.S. deaths as “missing Americans.”
The annual number of “missing Americans” increased steadily beginning in the late 1970s, reaching 626,353 in 2019 (Figure). Excess U.S. deaths jumped sharply to 991,868 in 2020 and 1,092,293 in 2021 during the COVID-19 pandemic.
In 2021, nearly 1 out of every 3 U.S. deaths would have been averted if U.S. mortality rates had equaled those of its peer nations. Half of these excess deaths were among U.S. residents under 65 years. We estimate that the 1.1M excess deaths in 2021 were associated with 25M years of life lost, accounting for the number of years the deceased would otherwise be expected to live.
We also compared mortality rates of U.S. racial and ethnic groups with the international benchmark. Black and Native Americans accounted for a disproportionate share of the “missing Americans.” However, the majority of “missing Americans” were White non-Hispanic persons.
Our findings are consistent with recent reports that the life expectancy gap between the U.S. and peer nations widened during the pandemic, with U.S. life expectancy falling from 78.9 to 76.6 years. Life expectancy is widely reported, but it is a complex measure and may be misinterpreted as reflecting small differences in mortality at advanced ages.
In fact, the greatest relative differences in mortality between the U.S. and peer countries occur before age 65. In 2021, half of all deaths to U.S. residents under 65 years – and 90% of the increase in under-65 mortality since 2019 – would have been avoided if the U.S. had the mortality rates of other wealthy nations. In addition to the loss of life, these early deaths often leave behind child (and elder) dependents without key social and economic support.
Our calculations were based on recently released mortality data, obtained from the U.S. Centers for Disease Control and Prevention WONDER Database and the Human Mortality Database. The international comparison group included all available countries with relatively complete mortality data starting in 1960 or earlier, after excluding former communist countries. Our paper builds on prior analyses of excess deaths by our study team and byothers.
We find a very large increase in excess U.S. deaths during the COVID-19 pandemic. However, this spike occurred on top of a growing trend that reached 600,000 excess deaths in 2019. Future COVID-19 deaths could be reduced with broader vaccine uptake, worker protections, and masking during surges. Even if COVID-19 mortality were eliminated, however, the U.S. would likely suffer hundreds of thousands of excess deaths each year, with many linked to firearms, opioids, and obesity.
Addressing excess deaths in the U.S. will require public health and social policies that target the root causes of U.S. health malaise, including fading economic opportunities and rising financial insecurity, structural racism, and failures of institutions at all levels of government to invest adequately in population health.
IBM Watson Health, in partnership with Fortune, has released its top 15 health systems, which they find set an example for health systems and hospitals across the nation. With its data, the report will continue to stand as a resource for these groups to improve their quality of care and efficiency.
In its 14th year of publishing this study, IBM Watson Health found that the top 15 health systems had better survival rates, fewer patient complications, fewer healthcare-associated infections, better long-term outcomes, better 30-day mortality/revisitation rates and more. The study also found that patients revered the top 15 hospitals more than peer system hospitals.
Fortune/IBM Watson Health divides its top 100 hospitals into three main categories listed below. It is noted that each system in the table is featured in alphabetical order and does not reflect performance rating. The full report, which includes further details on the methodology of rankings, can be found here.
Top 5 large health systems
Allina Health (Minneapolis)
Baylor Scott & White Health (Dallas)
Mayo Clinic (Rochester, Minn.)
Penn Medicine (Philadelphia)
Rush University System for Health (Chicago)
Top 5 medium health systems
Cone Health (Greensboro, N.C.)
Edward-Elmhurst Health (Naperville, Ill.)
PIH Health (Whittier, Calif.)
Scripps Health (San Diego)
St. Luke’s Health System (Boise, Idaho)
Top 5 small health systems
Asante (Medford, Ore.)
CHI Memorial (Chattanooga, Tenn.)
CHI St. Vincent (Little Rock, Ark.)
Franciscan Sisters of Christian Charity Sponsored Ministries (Manitowoc, Wis.)
Gun violence is a public health problem, but we don’t approach it like one. The debate often gets framed as “guns or no guns” when it isn’t that black and white. In this episode we break down how and why to approach gun violence as a public health problem, what the current research has to say, and what we need to move forward.