

Vaccine Research vs Anti-Vax Research
https://mailchi.mp/ad2d38fe8ab3/the-weekly-gist-january-6-2023?e=d1e747d2d8
Surging from less than 5 percent of cases in the first week of December, XBB.1.5 now makes up over 40 percent of all COVID infections in the US. The new variant appears to demonstrate a high level of immune evasion, and is around 40 percent more contagious than the next most virulent strain, though illnesses caused by XBB.1.5 do not seem to be more severe. Weekly rates for new COVID-related hospital admissions are now higher than at any point since February 2022, despite case counts remaining lower than the peak of the summer wave in July 2022 (although it is likely that the vast majority of cases are now identified through home testing, and not reported, making the data unreliable).
The Gist: While the new variant seems to be less likely to create a COVID spike of the magnitude we experienced last winter, hospitalizations rising faster than case counts bears watching. That’s especially true given the current staffing situation in most hospitals, which makes each COVID admission and each caregiver call-out for illness a cause for concern.
Only 15 percent of eligible Americans have received the most recent bivalent booster, leaving the population more vulnerable to this and future variants. Plus, additional funding to support the fight against COVID does not seem to be forthcoming from the new Congress. Beset with surges of COVID, flu, and RSV admissions, hospitals must hope that the end of the holiday season brings some relief.
https://mailchi.mp/0622acf09daa/the-weekly-gist-december-2-2022?e=d1e747d2d8
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.

Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8
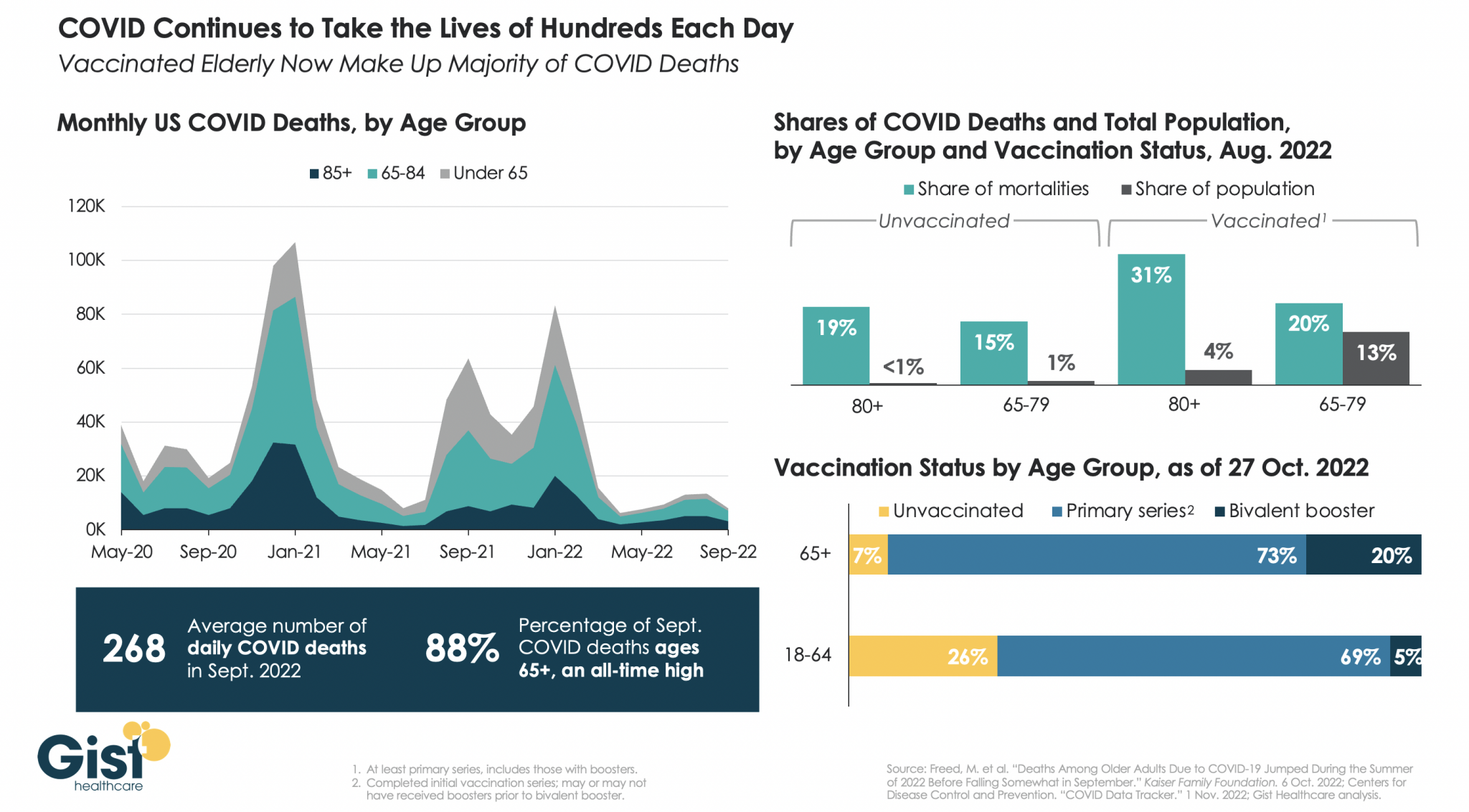
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
https://www.advisory.com/daily-briefing/2022/10/10/covid-resurgence

While infections, hospitalizations, and deaths from Covid-19 have been steadily declining in the United States in recent months, experts warn that rising cases in Europe may be “a harbinger for what’s about to happen in the United States,” Rob Stein writes for NPR’s “Shots.”
Currently, several models project that U.S. Covid-19 infections will continue to decline at least until the end of 2022. However, researchers caution that there are multiple variables that could change current projections, including whether more infectious strains start circulating around the nation.
According to Stein, “[t]he first hint of what could be in store is what’s happening in Europe.” Recently, many European countries, including the U.K., France, and Italy, have seen an increase in Covid-19 infections.
“In the past, what’s happened in Europe often has been a harbinger for what’s about to happen in the United States,” said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota. “So I think the bottom line message for us in this country is: We have to be prepared for what they are beginning to see in Europe.”
“We look around the world and see countries such as Germany and France are seeing increases as we speak,” said Lauren Ancel Meyers, director of the UT COVID-19 Modeling Consortium at the University of Texas at Austin. “That gives me pause. It adds uncertainty about what we can expect in the coming weeks and the coming months.”
However, Justin Lessler, an epidemiologist at the University of North Carolina who helps run the COVID-19 Scenario Modeling Hub, noted that the United States may not have the same experience as Europe, largely because it is unclear whether Europe’s increase is related to individuals’ vulnerability to new strains.
“If it is mostly just behavioral changes and climate, we might be able to avoid similar upticks if there is broad uptake of the bivalent vaccine,” Lessler added. “If it is immune escape across several variants with convergent evolution, the outlook for the U.S. may be more concerning.”
Some researchers believe the United States is already experiencing early signs of this. “For example, the levels of virus being detected in wastewater is up in some parts of the country, such in Pennsylvania, Connecticut, Vermont and other parts of Northeast,” Stein writes. “That could an early-warning sign of what’s coming, though overall the virus is declining nationally.”
“It’s really too early to say something big is happening, but it’s something that we’re keeping an eye on,” said Amy Kirby, national wastewater surveillance program lead at CDC.
According to David Rubin, the director of the PolicyLab at Children’s Hospital of Philadelphia, which tracks the pandemic, Covid-19 infections and hospitalizations are already rising in some parts of New England, and other northern regions, including the Pacific Northwest.
“We’re seeing the northern rim of the country beginning to show some evidence of increasing transmission,” Rubin said. “The winter resurgence is beginning.”
Unless a “dramatically different new variant emerges,” it is “highly unlikely this year’s surge would get as severe as the last two years in terms of severe disease and deaths,” Stein writes.
“We have a lot more immunity in the population than we did last winter,” said Jennifer Nuzzo, who leads the Pandemic Center at the Brown University School of Public Health.
“Not only have people gotten vaccinated, but a lot of people have now gotten this virus. In fact, some people have gotten it multiple times. And that does build up [immunity] in the population and reduce overall over risk of severe illness,” Nuzzo said.
Another factor that could affect the severity of the impact of rising infections is the number of people who receive updated Covid-19 vaccines, which help boost waning immunity from previous infections or shots.
However, the United States’ booster uptake has been slow. “Nearly 50% of people who are eligible for a booster have not gotten one,” said William Hanage, an associate professor of epidemiology at the Harvard T.H. Chan School of Public Health. “It’s wild. It’s really crazy.”
Since updated boosters became available in September, less than 8 million of the over 200 million people who are eligible have received one.
According to Nuzzo, it is critical for people to stay up to date on their vaccines, especially with the high likelihood of another Covid-19 surge. “The most important thing that we could do is to take off the table that this virus can cause severe illness and death,” Nuzzo said.
“There are a lot of people who could really benefit from getting boosted but have not done so,” she added.

Some good news: The world had its lowest COVID death toll last week since March 2020, the World Health Organization said.
Zoom out: Last summer’s Delta variant demolished the first sense of relief after vaccines.
The bottom line: The next surge could come by surprise.
The fact that poliovirus was detected in New York City wastewater samples as far back as April of this year shouldn’t be surprising, as the virus likely has been circulating for longer and more widely than previously believed, several experts told MedPage Today.
“I think you’re gonna see over the next weeks more and more reports of poliovirus in wastewater elsewhere,” said Vincent Racaniello, PhD, a virologist at Columbia University in New York City.
Poliovirus probably still circulated in the U.S. after 2000, when officials stopped giving the oral polio vaccine, he said. That version protects against paralysis and provides short-term protection against intestinal infection from poliovirus.
The transition to injectable polio vaccine, which is equally as effective against paralysis but not against intestinal infection, meant that the U.S. population was more susceptible to transmitting vaccine-associated poliovirus, he explained.
This circulation is likely occasional and sporadic, he said, but the threat to vulnerable populations is still high.
“Here’s the thing: polio is here in the U.S. It’s not gone,” Racaniello said. “It’s in the wastewater. It could contaminate you, so if you’re not vaccinated, that could be a problem.”
Calls for Nationwide Surveillance
Racaniello said there’s value in learning more about the circulation of the virus, especially for communities with low vaccination rates.
The first step to understanding how long and how broadly poliovirus is circulating, he said, is to start testing wastewater everywhere. The CDC used stored wastewater from April to confirm that the virus had been circulating then, but it is just as possible to conduct nationwide surveillance for poliovirus now, he noted.
In fact, Racaniello said, he has long believed that this kind of surveillance should be done routinely to provide an early detection system for poliovirus.
“Ten years ago, I said to the CDC, you should really be looking in the sewage for poliovirus because of this issue where it could come in from overseas and be in our sewage,” he said. “If someone is unvaccinated, that would be a threat to them, but [the CDC] never did it.”
Davida Smyth, PhD, of Texas A&M University-San Antonio, pointed out that the National Wastewater Surveillance System (NWSS) was established to detect COVID-19 in 2020, so the infrastructure to conduct a wide search for the spread of polio is available.
The primary issue, she said, is that the collaboration that academic researchers have enjoyed with the CDC in surveillance of COVID-19 is so far absent with poliovirus.
“I imagine the CDC is testing those samples for polio, even as we speak, given the nature of what has happened,” Smyth said.
Better coordination with academia and better surveillance, she said, is crucial for finding any potential pockets of poliovirus circulating in other communities around the U.S.
In fact, she said, she is “absolutely convinced” that more polio will be found in the coming weeks.
MedPage Today contacted the CDC to ask whether there are plans to use the NWSS to look for polio around the U.S., but as of press time had not received a response.
Smyth noted that most areas in the country have high rates of polio vaccination, but she is concerned about pockets of rural America where vaccination has dipped in recent years. Most states boast polio vaccination rates over 90%, but Smyth said in some regions, the percentages may be as low as the mid-30s.
“[In] the vast majority of the United States, the vaccination rates are quite high, but the COVID pandemic has led to a decrease in vaccination rates,” Smyth told MedPage Today. “The rates are going down. They’re dipping below 90%, which is shocking, frankly.”
Smyth said the decline is largely due to a lack of opportunity or access to healthcare in some areas, but vaccine hesitancy around the COVID-19 vaccine might be affecting polio vaccinations as well.
“There’s a variety of reasons why people don’t get vaccinated,” she said. “The problem is children are very vulnerable. So if you have a population where the vaccination rates drop, those are exactly the kinds of areas where we need to do this surveillance.”
Racaniello echoed the importance of polio vaccination in adults as well. If patients don’t have a record of their shot, “just vaccinate them,” he said, “because there’s no downside to getting vaccinated again.”
Re-evaluating the Polio Endgame
The recent case of paralytic polio infection and concerns over the wider circulation of poliovirus have also altered some of the thinking around the goal of polio eradication.
In fact, William Schaffner, MD, of Vanderbilt University Medical Center in Nashville, highlighted the unique difficulty of preventing the spread of poliovirus.
“As you can imagine, we’ve gotten into polio endgame,” he told MedPage Today. “I think the notion has now been modified. Eradication isn’t going to be as neat and clean and quick as we once thought. Once we get rid of all paralytic disease, we will have to keep vaccinating for a long time, because there will still be circulating vaccine-associated viruses — some of which will mutate back.”
Schaffner compared the final push to eradicate polio with the successful eradication of smallpox. When the last case of smallpox ended, he explained, public health officials were able to end smallpox vaccination campaigns. For polio, however, he said, it will likely not be that simple, and it will be necessary “to keep vaccinating for quite a long time.”
He said that as public health officials in the U.S. and globally continue to grapple with the nuances of eradicating poliovirus, healthcare providers and their patients will have to come to terms with the simple fact that polio is a real health concern.
“[It’s] the reverse of the old saying, ‘it’s gone, but not forgotten,'” Schaffner said. “Polio is forgotten, but it’s not gone.”

The U.S. may see a “pretty sizable wave” of COVID-19 infections this fall and winter as the virus continues to evolve and immunity wanes, White House Covid-19 Response Coordinator Ashish Jha, MD, said May 8 on ABC News‘ “This Week.”
Federal health officials are looking at a range of disease forecasting models, which suggest the U.S. could experience a large surge in late 2022, similar to the last two winters, according to Dr. Jha. On May 6, the White House projected 100 million COVID-19 infections could occur this fall and winter, according to The Washington Post.
“If we don’t get ahead of this thing … we may see a pretty sizable wave of infections, hospitalizations and deaths this fall and winter,” he said. “Whether that happens or not is largely up to us as a country. If we can prepare and if we can act, we can prevent that.”
More funding to purchase COVID-19 vaccines and therapeutics will be crucial to stave off a potential surge, according to Dr. Jha. The Biden administration is asking Congress for an additional $22.5 billion in emergency aid to support these efforts.
“If Congress does not do that now, we will go into this fall and winter with none of the capabilities that we have developed over the last two years,” Dr. Jha said.

Unvaccinated people accounted for the overwhelming majority of deaths in the United States throughout much of the coronavirus pandemic. But that has changed in recent months, according to a Washington Post analysis of state and federal data.
The pandemic’s toll is no longer falling almost exclusively on those who chose not to or could not get shots, with vaccine protection waning over time and the elderly and immunocompromised — who are at greatest risk of succumbing to covid-19, even if vaccinated — having a harder time dodging increasingly contagious strains.
The vaccinated made up 42 percent of fatalities in January and February during the highly contagious omicron variant’s surge, compared with 23 percent of the dead in September, the peak of the delta wave, according to nationwide data from the Centers for Disease Control and Prevention analyzed by The Post. The data is based on the date of infection and limited to a sampling of cases in which vaccination status was known.
As a group, the unvaccinated remain far more vulnerable to the worst consequences of infection — and are far more likely to die — than people who are vaccinated, and they are especially more at risk than people who have received a booster shot.
“It’s still absolutely more dangerous to be unvaccinated than vaccinated,” said Andrew Noymer, a public health professor at the University of California at Irvine who studies covid-19 mortality.“A pandemic of — and by — the unvaccinated is not correct. People still need to take care in terms of prevention and action if they became symptomatic.”
A key explanation for the rise in deaths among the vaccinated is that covid-19 fatalities are again concentrated among the elderly.
Nearly two-thirds of the people who died during the omicron surge were 75 and older, according to a Post analysis, compared with a third during the delta wave. Seniors are overwhelmingly immunized, but vaccines are less effective and their potency wanes over time in older age groups.
Experts say they are not surprised that vaccinated seniors are making up a greater share of the dead, even as vaccine holdouts died far more often than the vaccinated during the omicron surge, according to the CDC. As more people are infected with the virus, the more people it will kill, including a greater number who are vaccinated but among the most vulnerable.
The bulk of vaccinated deaths are among people who did not get a booster shot, according to state data provided to The Post. In two of the states, California and Mississippi, three-quarters of the vaccinated senior citizens who died in January and February did not have booster doses. Regulators in recent weeks have authorized second booster doses for people over the age of 50, but administration of first booster doses has stagnated.
Even though the death rates for the vaccinated elderly and immunocompromised are low, their losses numbered in the thousands when cases exploded, leaving behind blindsided families. But experts say the rising number of vaccinated people dying should not cause panic in those who got shots, the vast majority of whom will survive infections. Instead, they say, these deaths serve as a reminder that vaccines are not foolproof and that those in high-risk groups should consider getting boosted and taking extra precautions during surges.
“Vaccines are one of the most important and longest-lasting tools we have to protect ourselves,” said California State Epidemiologist Erica Pan, citing state estimates showing vaccines have shown to be 85 percent effective in preventing death.
“Unfortunately, that does leave another 15,” she said.
Arianne Bennett recalled her husband, Scott Bennett, saying, “But I’m vaxxed. But I’m vaxxed,” from the D.C. hospital bed where he struggled to fight off covid-19 this winter.
Friends had a hard time believing Bennett, co-founder of the D.C.-based chain Amsterdam Falafelshop, was 70. The adventurous longtime entrepreneur hoped to buy a bar and planned to resume scuba-diving trips and 40-mile bike rides to George Washington’s Mount Vernon estate.
Bennett went to get his booster in early December after returning to D.C. from a lodge he owned in the Poconos, where he and his wife hunkered down for fall. Just a few days after his shot, Bennett began experiencing covid-19 symptoms, meaning he was probably exposed before the extra dose of immunity could kick in. His wife suspects he was infected at a dinner where he and his server were unmasked at times.
A fever-stricken Bennett limped into the hospital alongside his wife, who was also infected, a week before Christmas. He died Jan. 13, among the 125,000 Americans who succumbed to covid-19 in January and February.
“He was absolutely shocked. He did not expect to be sick. He really thought he was safe,’” Arianne Bennett recalled. “And I’m like, ‘But baby, you’ve got to wear the mask all the time. All the time. Up over your nose.’”


Jason Salemi, an epidemiologist at the University of South Florida College of Public Health, said the deaths of vaccinated people are among the consequences of a pandemic response that emphasizes individuals protecting themselves.
“When we are not taking this collective effort to curb community spread of the virus, the virus has proven time and time again it’s really good at finding that subset of vulnerable people,” Salemi said.
While experts say even the medically vulnerable should feel assured that a vaccine will probably save their lives, they should remain vigilant for signs of infection. As more therapeutics become available, early detection and treatment is key.
When Wayne Perkey, 84, first started sneezing and feeling other cold symptoms in early February, he resisted his physician daughter’s plea to get tested for the coronavirus.
The legendary former morning radio host in Louisville had been boosted in October. He diligently wore a mask and kept his social engagements to a minimum. It must have been the common cold or allergies, he believed. Even the physician who ordered a chest X-ray and had no coronavirus tests on hand thought so.
Perkey relented, and the test came back positive. He didn’t think he needed to go to the hospital, even as his oxygen levels declined.
“In his last voice conversation with me, he said, ‘I thought I was doing everything right,’” recalled Lady Booth Olson, another daughter, who lives in Virginia. “I believe society is getting complacent, and clearly somebody he was around was carrying the virus. … We’ll never know.”
From his hospital bed, Perkey resumed a familiar role as a high-profile proponent for vaccines and coronavirus precautions. He was familiar to many Kentuckians who grew up hearing his voice on the radio and watched him host the televised annual Crusade for Children fundraiser. He spent much of the pandemic as a caregiver to his ex-wife who struggled with chronic fatigue and other long-haul covid symptoms.
“It’s the 7th day of my Covid battle, the worst day so far, and my anger boils when I hear deniers talk about banning masks or social distancing,” Perkey wrote on Facebook on Feb. 16, almost exactly one year after he posted about getting his first shot. “I remember times we cared about our neighbors.”
In messages to a family group chat, he struck an optimistic note. “Thanks for all the love and positive energy,” he texted on Feb. 23. “Wear your mask.”
As is often the case for covid-19 patients, his condition rapidly turned for the worse. His daughter Rebecca Booth, the physician, suspects a previous bout with leukemia made it harder for his immune system to fight off the virus. He died March 6.
“Really and truly his final days were about, ‘This virus is bad news.’ He basically was saying: ‘Get vaccinated. Be careful. But there is no guarantee,’” Rebecca Booth said. “And, ‘If you think this isn’t a really bad virus, look at me.’ And it is.”
Hospitals, particularly in highly vaccinated areas, have also seen a shift from covid wards filled predominantly with the unvaccinated. Many who end up in the hospital have other conditions that weakens the shield afforded by the vaccine.
Vaccinated people made up slightly less than half the patients in the intensive care units of Kaiser Permanente’s Northern California hospital system in December and January, according to a spokesman.
Gregory Marelich, chair of critical care for the 21 hospitals in that system, said most of the vaccinated and boosted people he saw in ICUs were immunosuppressed, usually after organ transplants or because of medications for diseases such as lupus or rheumatoid arthritis.
“I’ve cared for patients who are vaccinated and immunosuppressed and are in disbelief when they come down with covid,” Marelich said.
Jessica Estep, 41, rang a bell celebrating her last treatment for follicular lymphoma in September. The single mother of two teenagers had settled into a new home in Michigan, near the Indiana border. After her first marriage ended, she found love again and got married in a zoo in November.
As an asthmatic cancer survivor, Estep knew she faced a heightened risk from covid-19, relatives said. She saw only a tight circle of friends and worked in her own office in her electronics repair job. She lived in an area where around 1 in 4 residents are fully vaccinated. She planned to get a booster shot in the winter.
“She was the most nonjudgmental person I know,” said her mother, Vickie Estep. “It was okay with her if people didn’t mask up or get vaccinated. It was okay with her that they exercised their right of choice, but she just wanted them to do that away from her so that she could be safe.”
With Michigan battling back-to-back surges of the delta and omicron variants, Jessica Estep wasn’t able to dodge the virus any longer — she fell ill in mid-December. After surviving a cancer doctors described as incurable, Estep died Jan. 27. Physicians said the coronavirus essentially turned her lungs into concrete, her mother said.
Estep’s 14-year-old daughter now lives with her grandparents. Her widower returned to Indianapolis just months after he moved to Michigan to be with his new wife.
Her family shared her story with a local television station in hopes of inspiring others to get vaccinated, to protect people such as Estep who could not rely on their own vaccination as a foolproof shield. In response to the station’s Facebook post about the story, several commenters shrugged off their pleas and insinuated it was the vaccines rather than covid causing deaths.
Immunocompromised people and those with other underlying conditions are worth protecting, Vickie Estep said. “There’s life potential in those people.”
As Arianne Bennett navigates life without her husband, she hopes the lesson people heed from his death is to take advantage of all tools available to mitigate a virus that still finds and kills the vulnerable, including by getting boosters.
Bennett wore a music festival shirt her husband gave her as she walked into a grocery store to get her third shot in March. Her husband urged her to get one when they returned to D.C., but she became sick at the same time he did. She scheduled the appointment for the earliest she could get the shot: 90 days after receiving monoclonal antibodies to treat the disease.
“My booster! Yay!” Bennett exclaimed in her chair as the pharmacist presented an updated vaccine card.
“It’s been challenging, but we got through it,” the pharmacist said, unaware of Scott Bennett’s death.
Tears welled in Bennett’s eyes as the needle went in her left arm, just over a year after she and her husband received their first shots.
“Last time we got it, we took selfies: ‘Look, we had vaccines,’” Bennett said, beginning to sob. “This one leaves me crying, missing him so much.”
The pharmacist leaned over and gave Bennett a hug in her chair.
“He would want you to do this,” the pharmacist said. “You have to know.”
Death rates compare the number of deaths in various groups with an adjustment for the number of people in each group. The death rates listed for the fully vaccinated, the unvaccinated and those vaccinated with boosters were calculated by the CDC using a sample of deaths from 23 health departments in the country that record vaccine status, including boosters, for deaths related to covid-19. The CDC study assigns deaths to the month when a patient contracted covid-19, not the month of death. The latest data published in April reflected deaths of people who contracted covid as of February. The CDC study of deaths among the vaccinated is online, and the data can be downloaded.
The death rates for fully vaccinated people, unvaccinated people and fully vaccinated people who received an additional booster are expressed as deaths per 100,000 people. The death rates are also called incidence rates. The CDC estimated the population sizes from census data and vaccination records. The study does not include partially vaccinated people in the deaths or population. The CDC adjusted the population sizes for inaccuracies in the vaccination data. The death data is provisional and subject to change. The study sample includes the population eligible for boosters, which was originally 18 and older, and now is 12 and older.
To compare death rates between groups with different vaccination status, the CDC uses incidence rate ratios. For example, if one group has a rate of 10 deaths per 100,000 people, the death incidence rate would be 10. Another group may have a death incidence rate of 2.5. The ratio between the first group and the second group is the rate of 10 divided by the rate of 2.5, so the incidence rate ratio would be 4 (10÷2.5=4). That means the first group dies at a rate four times that of the second group.
The CDC calculates the death incidence rates and incidence rate ratios by age groups. It also calculates a value for the entire population adjusted for the size of the population in each age group. The Post used those age-adjusted total death incidence rates and incidence rate ratios.
The Post calculated the share of deaths by vaccine status from the sample of death records the CDC used to calculate death incidence rates by vaccine status. As of April, that data included 44,000 deaths of people who contracted covid in January and February.
The share of deaths for each vaccine status does not include deaths for partially vaccinated people because they are not included in the CDC data.
The Post calculated the share of deaths in each age group from provisional covid-19 death records that have age details from the CDC’s National Center for Health Statistics. That data assigns deaths by the date of death, not the date on which the person contracted covid-19. That data does not include any information on vaccine status of the people who died.
