Virus activity is picking up again as millions of Americans crisscross the country for Thanksgiving, taking fewer precautions to protect themselves against illness as concerns about COVID-19 fade away.
Why it matters:
Indoor holiday gatherings are expected to fuel a spike in cases of COVID-19, RSV and the flu — and with vaccinations against all three respiratory viruses lagging, health experts worry hospitals could be slammed again this winter.
What they’re saying:
“The concern here with this vaccination gap is: Could this get worse as the number of transmissions increases from November, December, into January?” Marc Watkins, chief medical officer for Kroger Health, told Axios.
State of play:
Health officials are urging vaccinations to head off a repeat of last winter’s “tripledemic,” when particularly nasty RSV and flu seasons collided with a COVID surge.
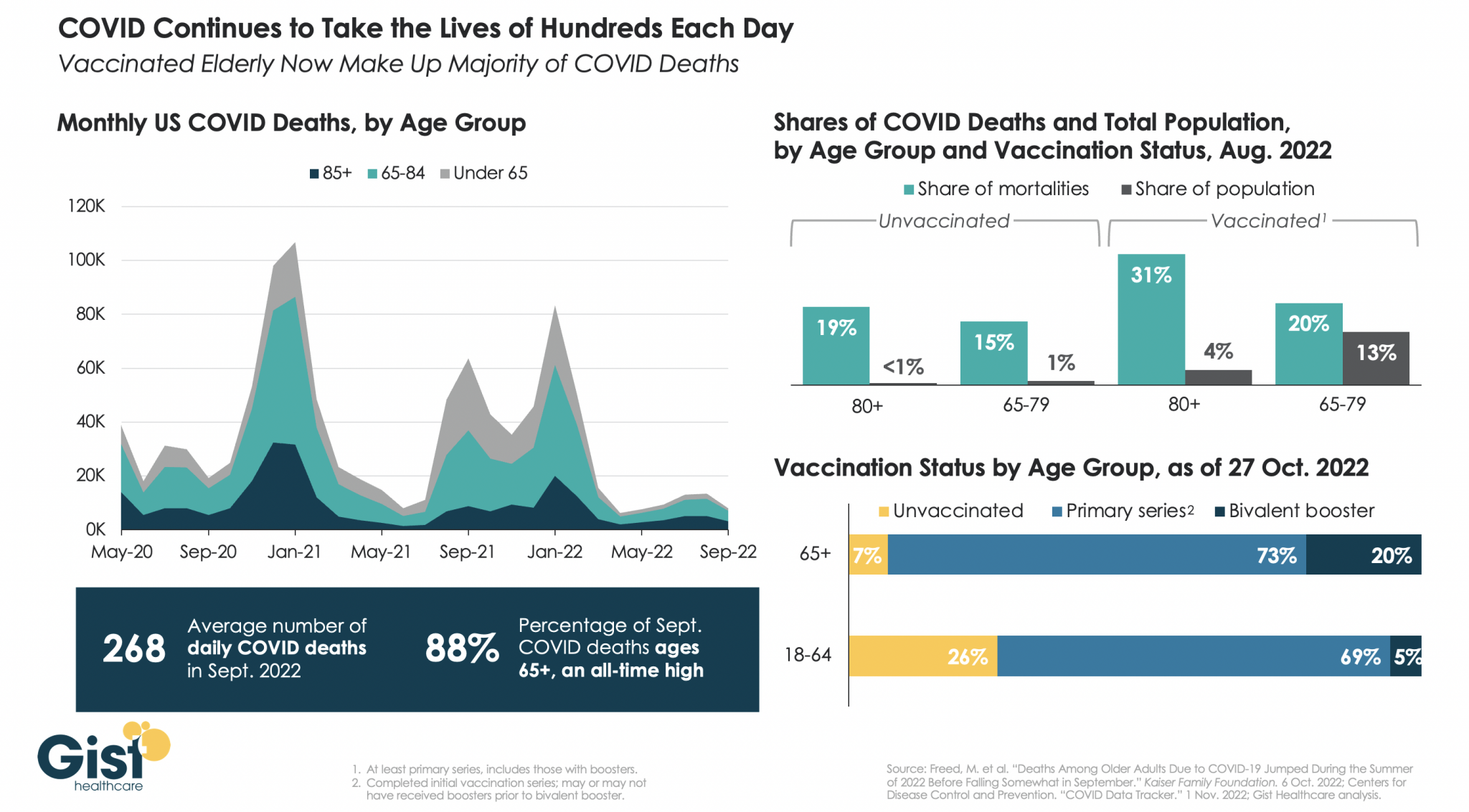
- About 15% of adults have received the updated COVID vaccine two months after it became available, according to the Centers for Disease Control and Prevention. That includes about a third of seniors, who are at highest risk from COVID.
- Most adults aren’t planning to get the updated COVID shot, according to a recent KFF survey that also found small shares were worried about COVID affecting their holiday plans.
- About half said they would take at least one precaution this fall and winter to limit their risk of getting COVID, such as avoiding large gatherings (35%) or masking in crowded places (30%).
- The vast majority of Americans have some form of immunity against COVID — from past infection, vaccination or both — but the updated shots can help protect against the latest circulating variants.
Meanwhile, flu vaccinations for adults and kids are slightly behind last year’s pace.
- Experts are hoping that new shots protecting older adults and infants against RSV will help keep patients out of the hospital. However, supplies have been limited, and some patients have run into hurdles getting insurers to pay for them.
- To help ease the supply strain, the CDC last week announced the release of 77,000 additional doses of a monoclonal antibody that protects against RSV in infants.
- 14% of adults 60 and older have received an RSV shot so far, according to the CDC. There isn’t yet data on pediatric vaccination rates.
Zoom in:
Texas is among the states that have been hit particularly hard by RSV early on, as emergency departments filled up with young patients in recent weeks.
- “We really were hoping that after two years of getting hit harder again with these viruses, it would kind of naturally be a milder season,” said Victoria Regan, a pediatrician at Children’s Memorial Hermann Hospital in Houston. “But it hasn’t happened yet.”
- There’s been a sharp rise in RSV cases in the last two weeks, according to CDC data.
- Flu cases rose 4% last week, and there’s high flu activity in several Southeastern states, as well as Washington, D.C., and Puerto Rico, according to CDC tracking.
- Though COVID isn’t being tracked as intensely since the pandemic ended, Midwestern and Western states have recently seen the highest rates of positive tests.
- And nationwide, COVID hospitalizations were up 8.6% in the most recent week for which the CDC has data, but still far below pandemic levels.
Be smart:
Those who are traveling should mask up in crowded areas like airports, have a game plan for getting tested or treated, and skip gatherings if feeling sick, recommended Mary Jacobson, chief medical officer at primary care company Alpha Medical.
The bottom line:
Expect a post-Thanksgiving spike in illness as respiratory virus season picks up and fewer people take precautions.
- “I think people are just fatigued you know, and they just want to go back to pre-COVID,” Jacobson said. “But this is here to stay.”