The Supreme Court on Friday upheld a key Affordable Care Act requirement that insurance companies cover certain preventative measures recommended by an expert panel.
Justices upheld the constitutionality of the provision in a 6-3 decision and protected access to preventative care for about 150 million Americans.
The justices found that the secretary of the Department of Health and Human Services has the power to appoint and fire members of the U.S. Preventative Services Task Force (USPSTF).
The cases started when a small business in Texas and some individuals filed a lawsuit against the panel’s recommendation that pre-exposure prophylaxis (PreP) for HIV be included as a preventative care service.
They argued that covering PreP went against their religious beliefs and would “encourage homosexual behavior, intravenous drug use, and sexual activity outside of marriage between one man and one woman.”
The plaintiffs further argued that the USPSTF mandates are unconstitutional because panel members are “inferior officers” who are not appointed by the president or confirmed by the Senate.
While the panel is independent, they said that since their decisions impact millions of people members should be confirmed.
A U.S. district judge in 2023 ruled that all preventative-care coverage imposed since the ACA was signed into law areinvalid and a federal appeals court judge ruled in agreement last year.
The Biden administration appealed the rulings to the Supreme Court, and the Trump administration chose to defend the law despite its long history of disparaging Obamacare.
Though public health groups celebrated the ruling Friday, some noted another potential outcome.
“While this is a foundational victory for patients, patients have reason to be concerned that the decision reaffirms the ability of the HHS secretary, including our current one, to control the membership and recommendations of the US Preventive Services Task Force that determines which preventive services are covered,” Anthony Wright, executive director of Families USA, said in a statement.
“We must be vigilant to ensure Secretary Kennedy does not undo coverage of preventive services by taking actions such as his recent firing of qualified health experts from the CDC’s independent vaccine advisory committee and replacing them with his personal allies.”
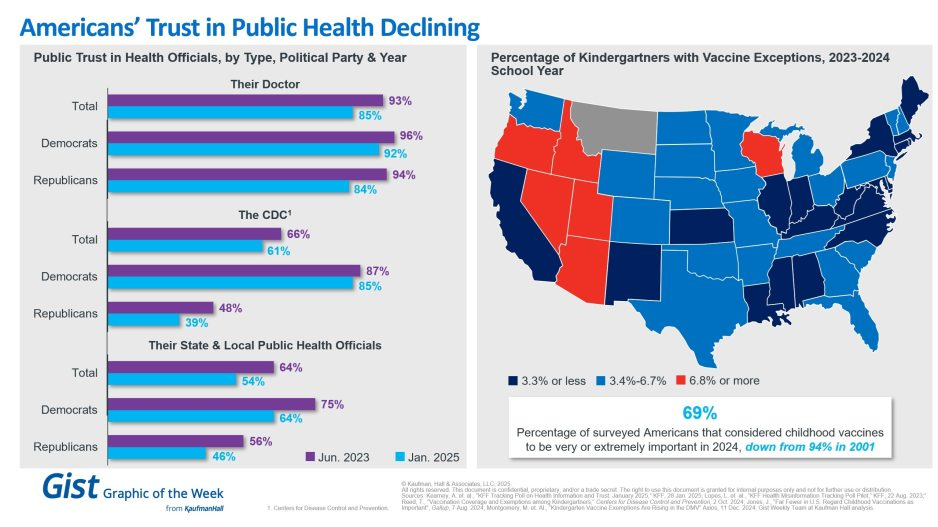
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
As seasonal virus activity surges across the United States, experts stress the importance of preventive measures – such as masking and vaccination – and the value of treatment for those who do get sick.
Tens of thousands of people have been admitted to hospitals for respiratory illness each week this season. During the week ending December 23, there were more than 29,000 patients admitted with Covid-19, about 15,000 admitted with the flu and thousands more with respiratory syncytial virus, or RSV, according to data from the US Centers for Disease Control and Prevention.
Nationally, Covid-19 levels in wastewater, a leading measure of viral transmission, are very high – higher than they were at this time last year in every region, CDC data shows. Weekly emergency department visits rose 12%, and hospitalizations jumped about 17% in the most recent week.
And while Covid-19 remains the leading driver of respiratory virus hospitalizations, flu activity is rising rapidly. The CDC estimates that there have been more than 7 million illnesses, 73,000 hospitalizations and 4,500 deaths related to the flu this season, and multiple indicators are high and rising.
RSV activity is showing signs of slowing in some parts of the US, but many measures, including hospitalization rates, remain elevated. Overall, young children and older adults are most affected.
“It’s a wave of winter respiratory pathogens, especially respiratory viruses. So it’s Covid, it’s flu, and we can’t diminish the importance of RSV,” said Dr. Peter Hotez, dean of the National School of Tropical Medicine at the Baylor College of Medicine. “So it’s a triple threat, and arguably a fourth threat because we also have pneumococcal pneumonia, which complicates a lot of these virus infections.”
Respiratory virus activity has been on the rise for weeks. Now, flu-like activity is high or very high in two-thirds of the United States, including California, New York City and Washington, as well as throughout the South and Northeast, according to the CDC.
“Remember, all of these numbers are before people got together for the holidays,” Hotez said. “So don’t be disappointed or surprised that we even see a bigger bump as we head into January.”
Vaccines can help prevent severe illness and death, but uptake remains low this season – despite a historic first, with vaccines available to protect against each of the three major viruses. Just 19% of adults and 8% of children have gotten the latest Covid-19 vaccine, and 17% of adults 60 and older have gotten the new RSV vaccine, CDC data shows. Less than half of adults and children have gotten the flu vaccine this season.
“We have, as a population, underutilized both influenza and the updated Covid vaccines, unfortunately,” said Dr. William Schaffner, an infectious disease expert at Vanderbilt University. “But it’s not too late to get vaccinated, because these viruses are going to be around for a while yet.”
According to the CDC, hospital bed capacity remains “stable” nationally, including within intensive care units. But with high levels of respiratory viruses, hospitals in at least five states are returning to requiring masks.
Mass General Brigham spokesman Timothy Sullivan said it will require masking for health-care staff who interact directly with patients starting Tuesday, and patients and visitors will be “strongly encouraged to wear a facility-issued mask.”
In Wisconsin, UW Health and UnityPoint Health – Meriter have expanded mask policies to cover more people. UW requires all staff, patients and visitors to wear a mask for patient interactions in clinic settings, including waiting areas and exam rooms.
UnityPoint Health – Meriter says masks continue to be required for team members and visitors in patient rooms.
Bellevue, a public hospital in New York City, said on social media last week that it had reinstated its mandatory masking policy due to an uptick in respiratory illnesses.
In Pennsylvania, the University of Pittsburgh Medical Center has required everyone to wear a mask when entering or inside since December 20. The systemwide masking policies were adjusted to “address the increase of respiratory virus cases” but may change when there is a “marked decrease in respiratory health cases,” according to the health care system.
An order posted last week by the Los Angeles County Health Officer requires all health-care personnel and visitors to mask while in contact with patients or in patient-care areas, based on the CDC’s categorization of Covid-19 hospital admission levels.
During the week ending December 23, more than 230 US counties were considered to have “high” levels of Covid-19 hospital admissions, defined by the CDC by at least 20 new hospital admissions for every 100,000 people. Nearly a thousand other counties, about a third of the country, have “medium” Covid-19 hospital admission levels, with at least 10 admissions for every 100,000 people.
Vaccines and masks can help reduce the risk of severe illness before getting sick, but treatments are also available to help prevent people from getting very sick if they do become infected.
Antiviral treatments for Covid-19, such as Paxlovid, and flu, such as Tamiflu, can be especially helpful for people who are more likely to get very sick, including people who are 50 or older and those with certain underlying conditions, such as a weakened immune system, heart disease, obesity, diabetes or chronic lung disease.
“If more people at higher risk for severe illness get treatment in a timely manner, we will save lives,” the CDC said in a recent blog post. But “not enough people are taking them.”
Seasonal respiratory virus activity can be hard to predict, but CDC forecasts suggest that hospitalization rates will continue at elevated levels for weeks and that this season, overall, will probably result in a similar number of hospitalizations as last season.
“One of the ways to help us all go into a happy new year is for us to be as protected as we can against these viruses,” Schaffner said.
“Of course, I continue to recommend vaccination, prudent use of the mask by high-risk people and, should you become sick, do not go to work and spread the virus further. Call your health care provider, because you may have some treatment available that will get you healthier sooner.”
On Monday, the Food and Drug Administration authorized new COVID vaccines from Moderna and Pfizer-BioNTech, and the Centers for Disease Control and Prevention followed Tuesday by recommending the shots be given as a single dose for most people five years of age and older. Children older than six months but younger than five, as well as completely unvaccinated people of any age, may be eligible for multiple doses.
These vaccines were formulated to target the XBB.1.5. variant,
which was the dominant strain in January but has since receded, although initial results suggest they remain effective against all currently circulating variants. Pharmacies and healthcare providers are expected to have the updated vaccines available by early next week.
The Gist: Due to the end of the COVID public health emergency in May, this COVID vaccination campaign will be the first not directly bankrolled by the federal government.
While insurers are still required to cover vaccinations without cost-sharing, the uninsured may find free shots, which the Biden administration says it will still provide at certain locations, harder to access.
Unlike past COVID boosters, reframing this shot as an annual vaccine that patients receive along with their flu shots should help with the rollout, as around 50 percent of Americans got a flu shot in 2022 while only 17 percent received the bivalent COVID booster.
With COVID cases and hospitalizations currently rising, promoting widespread uptake is critical to dampening a likely winter COVID spike.
However, public health officials will have to overcome many Americans’ wearied indifference toward COVID to motivate them to get vaccinated.
A new CDC study has found that the Covid-19 bivalent booster reduces the risk of symptomatic infection from the most common subvariant circulating in the U.S. right now by about half.
Additional new data, set to be published on the CDC website on Wednesday, also shows that individuals who received an updated vaccine reduced their risk of death by nearly 13 fold, when compared to the unvaccinated, and by two fold when compared to those with at least one monovalent vaccine but no updated booster.
CDC officials said during a briefing on Wednesday that the new findings were “reassuring.” But only 15.3 percent of eligible Americans — or about 50 million people — have received the new shot, which was rolled out in September.
Meanwhile, the highly transmissible Omicron subvariant XBB.1.5 — nicknamed “the Kraken” by some — is now the dominant SARS-CoV-2 strain in the U.S., projected by the CDC to make up just over 49 percent of cases in the country as of last week.
Earlier this month, the WHO said XBB.1.5 is the most transmissible variant to date, and is circulating in dozens of countries. Though a catastrophic wave has not emerged in the U.S. yet, there has nevertheless been a spike in deaths this month, with an average of 564 people dying of Covid-19 each day as of Jan. 18, compared with an average of 384 around the same time in December.
The new vaccine efficacy study, which used data from the national pharmacy program for Covid testing, found that the bivalent booster provided 48 percent greater protection against symptomatic infection from the XBB and XBB.1.5 subvariants among people who had the booster in the previous two to three months, compared with people who had only previously received two to four monovalent doses.
It also provided 52 percent greater protection against symptomatic infection from the BA.5 subvariant, though according to CDC estimates, BA.5 only accounted for about 2 percent of U.S. cases last week.
CDC officials cautioned that the findings reflected a population-level rate of protection, and that individual risk of infection varies.
“It’s hard to interpret it as an individual’s risk, because every individual is different,” said Ruth Link-Gelles, the author of the vaccine effectiveness study published in MMWR Wednesday. “Their immune system is different, their past history of prior infection is different. They may have underlying conditions that put them at more or less risk of COVID-19 disease.”
She also said it was unclear, given the limitations of the study, how long the bivalent booster protection will last.
“It’s too early to know how waning will happen with the bivalent vaccine,” she said. “What we’ve seen in the past is that your protection lasts longer for more severe illness. So even though you may have diminished protection over time against symptomatic infection, you’re likely still protected against more severe disease for a longer period of time.”
Surging from less than 5 percent of cases in the first week of December, XBB.1.5 now makes up over 40 percent of all COVID infections in the US. The new variant appears to demonstrate a high level of immune evasion, and is around 40 percent more contagious than the next most virulent strain, though illnesses caused by XBB.1.5 do not seem to be more severe. Weekly rates for new COVID-related hospital admissions are now higher than at any point since February 2022, despite case counts remaining lower than the peak of the summer wave in July 2022 (although it is likely that the vast majority of cases are now identified through home testing, and not reported, making the data unreliable).
The Gist: While the new variant seems to be less likely to create a COVID spike of the magnitude we experienced last winter, hospitalizations rising faster than case counts bears watching. That’s especially true given the current staffing situation in most hospitals, which makes each COVID admission and each caregiver call-out for illness a cause for concern.
Only 15 percent of eligible Americans have received the most recent bivalent booster, leaving the population more vulnerable to this and future variants. Plus, additional funding to support the fight against COVID does not seem to be forthcoming from the new Congress. Beset with surges of COVID, flu, and RSV admissions, hospitals must hope that the end of the holiday season brings some relief.
Hospitals across the country are being hit with a spike in respiratory syncytial virus (RSV) and influenza cases, while still dealing with a steady flow of COVID admissions, in what’s been dubbed a “tripledemic”. The graphic above uses hospitalization data from the Centers for Disease Control and Prevention (CDC) to show that each disease has been sending similar shares of the population to hospitals across late fall, with flu hospitalizations having just overtaken COVID admissions after Thanksgiving.
These numbers reflect that we’re experiencing the worst RSV season in at least five years, and we’re set to endure the worst flu season since 2009-10.As RSV is most severe in very young children, its recent surge has revealed another capacity shortage in our nation’s hospitals: pediatric beds. From 2008 to 2018, pediatric inpatient bed counts fell by 19 percent, as hospitals shifted resources to higher revenue services.
This strategy has now come to a head in many parts of the country, as RSV has driven pediatric bed usage rates to a recent high. (The Department of Health and Human Services’ pediatric capacity data only dates back to August 2020.) With three straight weeks of declining RSV hospitalizations, there is reason to hope that pediatric care units will soon feel a reprieve. However, flu season has yet to reach its peak, prompting calls for a return to widespread mask-wearing and a renewed emphasis on flu shots, given that more than half of Americans have not yet gotten vaccinated this season.
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.
A storm of these proportions should demand not only crisis clinical measures, but also community prevention efforts. Yet instead of deploying public health strategies to weather the storm, the U.S. is abandoning them.
Even before the arrival of the so-called tripledemic, U.S. health systems were on the brink. But as the fall surge of illness threatens to capsize teetering hospitals, the will to deploy public health measures has also collapsed. Pediatricians are declaring “This is our March 2020” and issuing pleas for help while public health efforts to flatten the curve and reduce transmission rates of Covid-19 — or any infectious disease — have effectively evaporated. Unmanageable patient volumes are seen as inevitable, or billed as the predictable outcome of an “immunity debt,” despite considerable uncertainty surrounding the scientific underpinnings and practical utility of this concept.
The Covid-19 pandemic should have left us better prepared for this moment. It helped the public to understand that respiratory viruses primarily spread through shared indoor air. Public health practices to stop the spread of Covid-19 — such as masking, moving activities outdoors, and limiting large gatherings during surges — were incorporated into the daily routines of many Americans. RSV and flu are also much less transmissible than Covid-19, making them easier to control with common-sense public health practices.
Instead of dialing up those first-line practices as pediatric ICUs overflow and classrooms close, though, the U.S. is relying on its precious and fragile last lines of defense to combat the tripledemic: health care professionals and medical facilities.
Warnings and advisories recently issued by U.S. public health leaders, clinical leaders, politicians, and the media have consistently neglected to mention masking as a powerful short-term public health strategy that can blunt the surge of viral illness. Instead, recent guidance has exclusively promoted handwashing and cough etiquette. These recommendations run counter to recent calls to build on improved understanding of the transmission of respiratory viruses.
In the U.S.’s efforts to “move on” from thinking about Covid, it has created a “new normal” that is deeply abnormal — one in which we normalize resorting to crisis measures, such as treating patients in tents, instead of using common-sense public health strategies. Treating Covid like the flu — or the flu like Covid — has effectively meant that we treat neither illness as if it were a serious threat to health systems and to public health. Mobilizing Department of Defense troops and Federal Emergency Management Agency personnel to cover health system shortfalls is apparently more palatable than asking people to wear masks.
The tripledemic has already claimed its first child deaths in the U.S., adding to a large ongoing death toll from Covid. Allowing health systems to reach the brink of collapse will lead to many more preventable deaths among pediatric and other vulnerable patients who can’t access the care they need.
By any accounting, these losses are shocking and tragic. But they should strike us as particularly abhorrent and shameful because the tripledemic is a crisis that leaders, health agencies, and institutions have, in a sense, chosen. Over the past year, the Biden administration and its allies have repeatedly encouraged the public to stand down on public health measures, with the President even stating in September that “the pandemic is over.” By moving real risks out of view and failing to push for more robust measures to mitigate Covid, these messages have put the country on a path to its present circumstances, in which pediatric RSV patients are transferred to hospitals hundreds of miles away because there is no capacity to treat them in their own communities.
Living with viruses should mean embracing simple public health measures rather than learning to live with staggering levels of illness and death. Leaders in public health and medicine should issue timely and appropriate guidance that reflects the latest science instead of second-guessing the prevailing winds in public opinion. Instead of self-censoring their recommendations out of fear of political consequences, they should continue to promote the full range of public health strategies, including masking in crowded indoor public places during surges.
The tripledemic should bring renewed urgency to policies that will reduce the toll of seasonal illness on health, education, and the economy. Improvements in indoor air quality in public spaces, including schools, child care centers, and workplaces, can limit the spread of diseases and have many demonstrated health and economic benefits, yet the U.S. continues to lack standards to guide infrastructure or workplace safety standards. Paid leave enabling workers to stay home when they are ill can reduce the transmission of disease as well as loss of income, yet the U.S. is one of the only high-income countries without universal paid sick leave or family medical leave.
Greater effort must also be made to increase vaccination coverage for flu and Covid and bring an RSV vaccine online as quickly as possible. Only about half of high-risk adults under 65 received a flu shot last year, a gap that can be closed with more energetic vaccination campaigns. Reducing annual flu deaths using a broader range of strategies enabled by the pandemic — rather than pegging Covid deaths to them — should be the goal.
Amid the many sobering stories of the tripledemic, there is some good news. As the experience of Covid-19 has shown, it is possible to limit the toll of respiratory viruses like flu and RSV. However, this work requires resources, appropriate policies, and political will. Americans don’t need to accept winter disease surges and overrun health systems as an inevitable new normal. Instead, the country should see the tripledemic as a call to reinvigorate public health strategies in response to these threats to the health of our communities.
A new COVID calamity is hammering China, with a surge in infections prompting a return of lockdowns, including in some manufacturing areas that supply the West.
China reported a record number of infections this week, amid lockdowns and mass testing that are fueling unrest and darkening the country’s economic outlook. Schools in Beijing returned to online teaching.
Why it matters: In addition to the human misery for the world’s most populous country, the effects will be felt around the globe, Axios China author Bethany Allen-Ebrahimian reports from Taipei.
Supply chains are likely to be disrupted, causing prices to rise in an already rocky global economy.
Rare protests broke out today in China’s far western Xinjiang region. Crowds shouted at hazmat-suited guards after a deadly fire triggered anger by prolonged COVID lockdowns, Reuters reports.
“End the lockdown!” shouted protesters in the Xinjiang capital Urumqi, where an apartment fire killed 10.
What’s happening: The moment of truth for China’s zero-COVID policy has finally come.
Either party leaders will need to plunge much of the country into draconian lockdowns, as we saw at the beginning of the pandemic — or they’ll decide it’s time to learn to live with COVID.
Reality check: China’s doctors have warned Xi Jinping that the healthcare system isn’t prepared for the huge outbreak likely to follow the easing of strict anti-COVID measures, the Financial Times reports.
Chinese-made vaccines, which don’t use the mRNA technology employed by many produced by the West, aren’t as effective compared to those made in the U.S. And China has worrisomely low vaccination rates among older people.
But the number of cases in China is actually still very low for anywhere but China.
The big picture: “Zero COVID” restrictions have damaged the economy and undermined people’s trust in government.
That’s a stark about-face from the height of the pandemic. Then, many Chinese people felt the tight central control had protected them better than any other governance model in the world.
But it’s that very model that has plunged China into its current predicament. Xi tied his reputation, and the party’s legitimacy, to the success of “zero COVID.”
Between the lines: Chinese leaders made a huge, politically motivated mistake. They resisted the import of Western-made mRNA vaccines (including Pfizer and Moderna) for its citizens. These vaccines were only recently made available to foreigners.
That’s likely because of Beijing’s big vaccine diplomacy push: Chinese officials touted their own vaccines as the best and safest.
It was politically unpalatable to admit “defeat,” and allow Chinese people to get more effective — but Western-made — jabs.