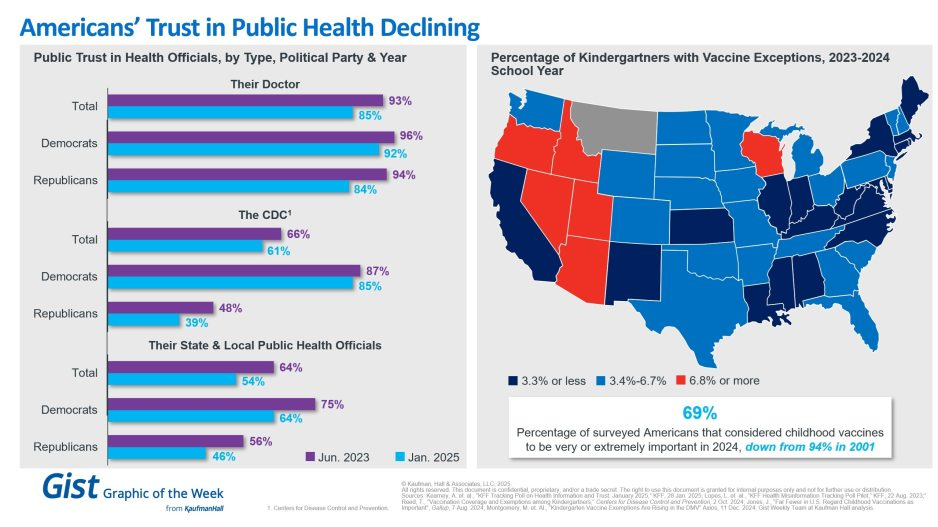
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
A surge in COVID-19 infections has swept the country this summer, upending travel plans and bringing fevers, coughs and general malaise. It shows no immediate sign of slowing.
While most of the country and the federal government has put the pandemic in the rearview mirror, the virus is mutating and new variants emerging.
Even though the Centers for Disease Control and Prevention (CDC) no longer tracks individual infection numbers, experts think it could be the biggest summer wave yet.
So far, the variants haven’t been proven to cause a more serious illness, and vaccines remain effective, but there’s no certainty about how the virus may yet change and what happens next.
The highest viral activity right now is in the West, according to wastewater data from the CDC, but a “high” or “very high” level of COVID-19 virus is being detected in wastewater in almost every state. And viral levels are much higher nationwide than they were this time last year and started increasing earlier in the summer.
Wastewater data is the most reliable method of tracking levels of viral activity because so few people test, but it can’t identify specific case numbers.
Part of the testing decline can be attributed to pandemic fatigue, but experts said it’s also an issue of access.Free at-home tests are increasingly hard to find. The government isn’t distributing them, and private insurance plans have not been required to cover them since the public health emergency ended in 2023.
COVID has spiked every summer since the start of the pandemic. Experts have said the surge is being driven by predictable trends like increased travel and extreme hot weather driving more people indoors, as well as by a trio of variants that account for nearly 70 percent of all infections.
Vaccines and antivirals can blunt the worst of the virus, and hospital are no longer being overwhelmed like in the earliest days of the pandemic.
But there remains a sizeable number of people who are not up-to-date on vaccinations. There are concerns that diminished testing and low vaccination rates could make it easier for more dangerous variants to take hold.
“One of the things that’s distinctive about this summer is that the variants out there are extraordinarily contagious, so they’re spreading very, very widely, and lots of people are getting mild infections, many more than know it, because testing is way down,” said William Schaffner, a professor of preventive medicine and infectious diseases at Vanderbilt University.
That contagiousness means the virus is more likely to find the people most vulnerable — people over 65, people with certain preexisting conditions, or those who are immunocompromised.
In a July interview with the editor-in-chief of MedPage Today, the country’s former top infectious diseases doctor, Anthony Fauci, said people in high-risk categories need to take the virus seriously, even if the rest of the public does not.
“You don’t have to immobilize what you do and just cut yourself off from society,” Fauci said. “But regardless of what the current recommendations are, when you are in a crowded, closed space and you are an 85-year-old person with chronic lung disease or a 55-year-old person who’s morbidly obese with diabetes and hypertension, then you should be wearing a mask when you’re in closed indoor spaces.”
Schaffner said hospitalizations have been increasing in his region for at least the past five weeks, which surprised him.
“I thought probably they had peaked last week. Wrong. They went up again this week. So at least locally, we haven’t seen the peak yet. I would have expected this summer increase … to have plateaued and perhaps start to ease down. But we haven’t seen that yet,” he said.
Still, much of the country has moved on from the pandemic and is reacting to the surge with a collective shrug. COVID-19 is being treated like any other respiratory virus, including by the White House.
President Biden was infected in July. After isolating at home for several days and taking a course of the antiviral Paxlovid, he returned to campaign trial.
Biden is 81, meaning he’s considered high risk for severe infection. He received an updated coronavirus vaccine in September, but it’s not clear if he got a second one, which the CDC recommends for older Americans.
Updated vaccines that target the current variants are expected to be rolled out later this fall, and the CDC recommends everyone ages 6 months and older should receive one.
As of May, only 22.5 percent of adults in the United States reported having received the updated 2023-2024 vaccine that was released last fall and tailored to the XBB variant dominant at that time.
The immunity from older vaccines wanes over time, and while it doesn’t mean people are totally unprotected, Schaffner said, the most vulnerable should be cautious. Many people being infected now have significantly reduced immunity to the current mutated virus, but reduced immunity is better than no immunity.
People with healthy immune systems and who have previously been vaccinated or infected are still less likely to experience the more severe infections that result in hospitalization or death.
Almost “none of us are naive to COVID, but the people where the protection wanes the most are the most frail, the immunodeficient, the people with chronic underlying illnesses,” Schaffner said.
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.
Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
Can bivalent boosters prevent another surge of infections?
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
How much additional protection do updated shots provide?
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Will we see an increase in vaccine uptake?
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”
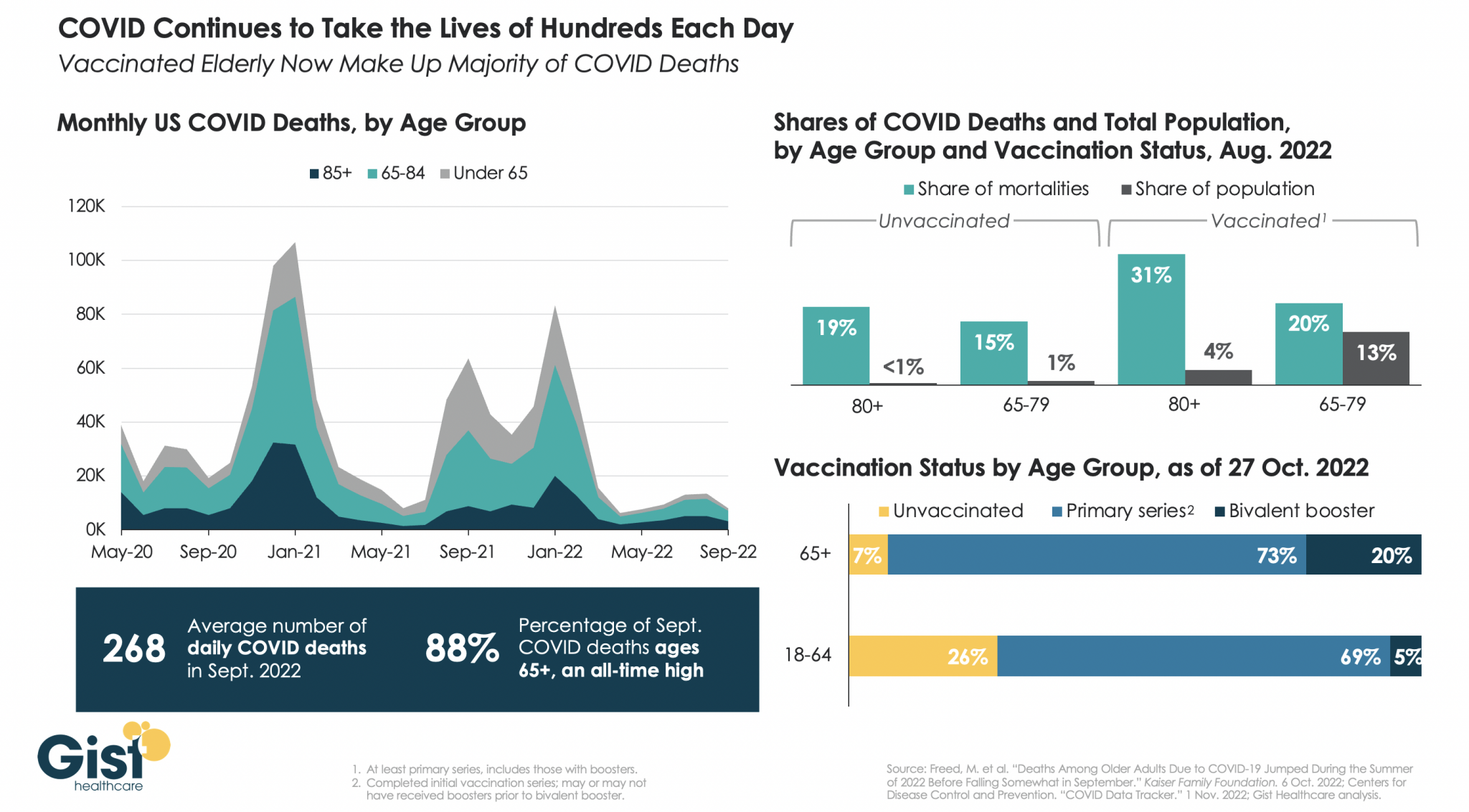
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
While infections, hospitalizations, and deaths from Covid-19 have been steadily declining in the United States in recent months, experts warn that rising cases in Europe may be “a harbinger for what’s about to happen in the United States,” Rob Stein writes for NPR’s “Shots.”
Will the US see a ‘winter resurgence’ of Covid-19?
Currently, several models project that U.S. Covid-19 infections will continue to decline at least until the end of 2022. However, researchers caution that there are multiple variables that could change current projections, including whether more infectious strains start circulating around the nation.
According to Stein, “[t]he first hint of what could be in store is what’s happening in Europe.” Recently, many European countries, including the U.K., France, and Italy, have seen an increase in Covid-19 infections.
“In the past, what’s happened in Europe often has been a harbinger for what’s about to happen in the United States,” said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota. “So I think the bottom line message for us in this country is: We have to be prepared for what they are beginning to see in Europe.”
“We look around the world and see countries such as Germany and France are seeing increases as we speak,” said Lauren Ancel Meyers, director of the UT COVID-19 Modeling Consortium at the University of Texas at Austin. “That gives me pause. It adds uncertainty about what we can expect in the coming weeks and the coming months.”
However, Justin Lessler, an epidemiologist at the University of North Carolina who helps run the COVID-19 Scenario Modeling Hub, noted that the United States may not have the same experience as Europe, largely because it is unclear whether Europe’s increase is related to individuals’ vulnerability to new strains.
“If it is mostly just behavioral changes and climate, we might be able to avoid similar upticks if there is broad uptake of the bivalent vaccine,” Lessler added. “If it is immune escape across several variants with convergent evolution, the outlook for the U.S. may be more concerning.”
Some researchers believe the United States is already experiencing early signs of this. “For example, the levels of virus being detected in wastewater is up in some parts of the country, such in Pennsylvania, Connecticut, Vermont and other parts of Northeast,” Stein writes. “That could an early-warning sign of what’s coming, though overall the virus is declining nationally.”
“It’s really too early to say something big is happening, but it’s something that we’re keeping an eye on,” said Amy Kirby, national wastewater surveillance program lead at CDC.
According to David Rubin, the director of the PolicyLab at Children’s Hospital of Philadelphia, which tracks the pandemic, Covid-19 infections and hospitalizations are already rising in some parts of New England, and other northern regions, including the Pacific Northwest.
“We’re seeing the northern rim of the country beginning to show some evidence of increasing transmission,” Rubin said. “The winter resurgence is beginning.”
How likely is a severe Covid-19 surge?
Unless a “dramatically different new variant emerges,” it is “highly unlikely this year’s surge would get as severe as the last two years in terms of severe disease and deaths,” Stein writes.
“We have a lot more immunity in the population than we did last winter,” said Jennifer Nuzzo, who leads the Pandemic Center at the Brown University School of Public Health.
“Not only have people gotten vaccinated, but a lot of people have now gotten this virus. In fact, some people have gotten it multiple times. And that does build up [immunity] in the population and reduce overall over risk of severe illness,” Nuzzo said.
Another factor that could affect the severity of the impact of rising infections is the number of people who receive updated Covid-19 vaccines, which help boost waning immunity from previous infections or shots.
However, the United States’ booster uptake has been slow. “Nearly 50% of people who are eligible for a booster have not gotten one,” said William Hanage, an associate professor of epidemiology at the Harvard T.H. Chan School of Public Health. “It’s wild. It’s really crazy.”
Since updated boosters became available in September, less than 8 million of the over 200 million people who are eligible have received one.
According to Nuzzo, it is critical for people to stay up to date on their vaccines, especially with the high likelihood of another Covid-19 surge. “The most important thing that we could do is to take off the table that this virus can cause severe illness and death,” Nuzzo said.
“There are a lot of people who could really benefit from getting boosted but have not done so,” she added.
Zoom out: Last summer’s Delta variant demolished the first sense of relief after vaccines.
“If we don’t take this opportunity now, Tedros said while calling for more vaccinations and testing, “we run the risk of more variants, more deaths, more disruption and more uncertainty.”
The bottom line: The next surge could come by surprise.
Johns Hopkins University is scaling back its COVID metrics due to a slowdown in local data reporting, the university confirmed to Axios.
The U.S. may see a “pretty sizable wave” of COVID-19 infections this fall and winter as the virus continues to evolve and immunity wanes, White House Covid-19 Response Coordinator Ashish Jha, MD, said May 8 on ABC News‘ “This Week.”
Federal health officials are looking at a range of disease forecasting models, which suggest the U.S. could experience a large surge in late 2022, similar to the last two winters, according to Dr. Jha. On May 6, the White House projected 100 million COVID-19 infections could occur this fall and winter, according to The Washington Post.
“If we don’t get ahead of this thing … we may see a pretty sizable wave of infections, hospitalizations and deaths this fall and winter,” he said. “Whether that happens or not is largely up to us as a country. If we can prepare and if we can act, we can prevent that.”
More funding to purchase COVID-19 vaccines and therapeutics will be crucial to stave off a potential surge, according to Dr. Jha. The Biden administration is asking Congress for an additional $22.5 billion in emergency aid to support these efforts.
“If Congress does not do that now, we will go into this fall and winter with none of the capabilities that we have developed over the last two years,” Dr. Jha said.