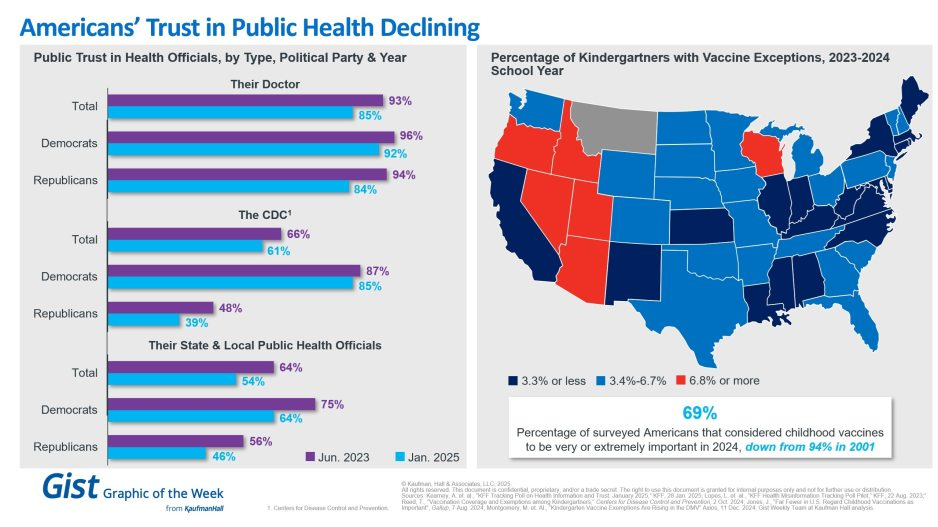
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
Last week, President-elect Donald Trump announced that Robert F. Kennedy, Jr. would be his nominee for Secretary of Health and Human Services (HHS). He followed this up on Tuesday with his selection of Dr. Mehmet Oz as his nominee for the Centers for Medicare and Medicaid Services (CMS) Administrator. If confirmed, the two men would replace Xavier Becerra and Chiquita Brooks-LaSure, respectively.
Kennedy, who ended his independent presidential campaign and endorsed Trump in August, has become known for his heterodox views on public health, including vaccine skepticism and opposition to water fluoridization.
Dr. Oz, first famous as a TV personality and more recently a Republican candidate for Pennsylvania Senator, is a strong proponent of Medicare Advantage, having co-authored an op-ed advocating for “Medicare Advantage for All” in 2020.
The Gist:
These nominees, especially Kennedy, hold a number of personal beliefs at odds with the public health consensus.
They are both likely to be confirmed, however, as the last cabinet nominee to be rejected by the Senate was John Tower in 1989. (This does not include nominees who have chosen to withdraw themselves from consideration, as former Representative Matt Gaetz has just done.)
Should they be confirmed, they will be responsible for implementing not their own but President Trump’s agenda, the specific priorities of which also remain relatively undefined.
However, possible consensus points between Trump and his nominees include public health cuts and deregulation, greater scrutiny of pharmaceutical companies, and a favoring of Medicare Advantage over traditional Medicare.
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.
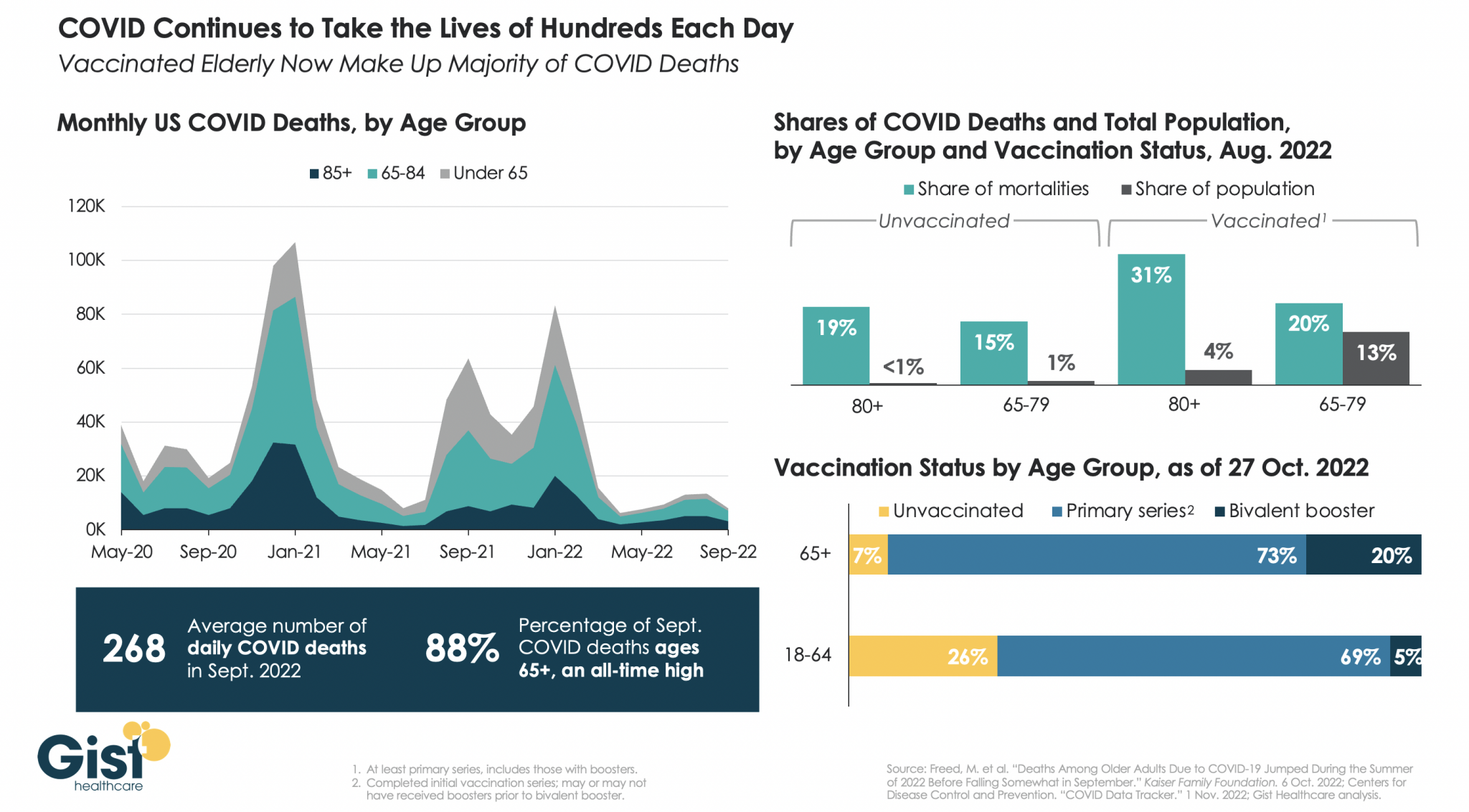
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
New York Gov. Kathy Hochul on Sept. 9 declared a state of emergency amid evidence that polio is spreading in communities around the state. The move unlocks federal resources to help the state respond and boost vaccination rates.
Under the declaration, pharmacists, emergency medical personnel and midwives can now administer polio vaccines. The executive order also requires providers to send polio vaccination data to the state’s health department.
“On polio, we simply cannot roll the dice,”said Mary Bassett, MD, health commissioner at the state’s health department. “If you or your child are unvaccinated or not up to date with vaccinations, the risk of paralytic disease is real. I urge New Yorkers to not accept any risk at all.”
The declaration came the same day state health officials reported that the virus had been detected in wastewater samples from Nassau County. Officials have also found the virus in sewage samples from New York City, Orange County, Sullivan County and Rockland County, where the nation’s first polio case in nearly a decade was confirmed July 21 in an unvaccinated man. Health officials have suggested the Rockland County case may just be the “tip of the iceberg” with hundreds of other cases potentially going undetected in the state.
The threat of polio’s resurgence is magnified by the many pockets of unvaccinated residents throughout the state. New York’s polio vaccination rate is 78.96 percent. That figure is lower in many of the counties where the virus has been detected in wastewater. In Rockland County, for example, the polio vaccination rate is 60.3 percent, state data shows. Nationwide, polio vaccination coverage sits at about 93 percent, according to the CDC.
The virus has likely been circulating in U.S. cities intermittently for years, experts say.
The fact that poliovirus was detected in New York City wastewater samples as far back as April of this year shouldn’t be surprising, as the virus likely has been circulating for longer and more widely than previously believed, several experts told MedPage Today.
“I think you’re gonna see over the next weeks more and more reports of poliovirus in wastewater elsewhere,” said Vincent Racaniello, PhD, a virologist at Columbia University in New York City.
Poliovirus probably still circulated in the U.S. after 2000, when officials stopped giving the oral polio vaccine, he said. That version protects against paralysis and provides short-term protection against intestinal infection from poliovirus.
The transition to injectable polio vaccine, which is equally as effective against paralysis but not against intestinal infection, meant that the U.S. population was more susceptible to transmitting vaccine-associated poliovirus, he explained.
This circulation is likely occasional and sporadic, he said, but the threat to vulnerable populations is still high.
“Here’s the thing: polio is here in the U.S. It’s not gone,” Racaniello said. “It’s in the wastewater. It could contaminate you, so if you’re not vaccinated, that could be a problem.”
Calls for Nationwide Surveillance
Racaniello said there’s value in learning more about the circulation of the virus, especially for communities with low vaccination rates.
The first step to understanding how long and how broadly poliovirus is circulating, he said, is to start testing wastewater everywhere. The CDC used stored wastewater from April to confirm that the virus had been circulating then, but it is just as possible to conduct nationwide surveillance for poliovirus now, he noted.
In fact, Racaniello said, he has long believed that this kind of surveillance should be done routinely to provide an early detection system for poliovirus.
“Ten years ago, I said to the CDC, you should really be looking in the sewage for poliovirus because of this issue where it could come in from overseas and be in our sewage,” he said. “If someone is unvaccinated, that would be a threat to them, but [the CDC] never did it.”
Davida Smyth, PhD, of Texas A&M University-San Antonio, pointed out that the National Wastewater Surveillance System (NWSS) was established to detect COVID-19 in 2020, so the infrastructure to conduct a wide search for the spread of polio is available.
The primary issue, she said, is that the collaboration that academic researchers have enjoyed with the CDC in surveillance of COVID-19 is so far absent with poliovirus.
“I imagine the CDC is testing those samples for polio, even as we speak, given the nature of what has happened,” Smyth said.
Better coordination with academia and better surveillance, she said, is crucial for finding any potential pockets of poliovirus circulating in other communities around the U.S.
In fact, she said, she is “absolutely convinced” that more polio will be found in the coming weeks.
MedPage Today contacted the CDC to ask whether there are plans to use the NWSS to look for polio around the U.S., but as of press time had not received a response.
Smyth noted that most areas in the country have high rates of polio vaccination, but she is concerned about pockets of rural America where vaccination has dipped in recent years.Most states boast polio vaccination rates over 90%, but Smyth said in some regions, the percentages may be as low as the mid-30s.
“[In] the vast majority of the United States, the vaccination rates are quite high, but the COVID pandemic has led to a decrease in vaccination rates,” Smyth told MedPage Today. “The rates are going down. They’re dipping below 90%, which is shocking, frankly.”
Smyth said the decline is largely due to a lack of opportunity or access to healthcare in some areas, but vaccine hesitancy around the COVID-19 vaccine might be affecting polio vaccinations as well.
“There’s a variety of reasons why people don’t get vaccinated,” she said. “The problem is children are very vulnerable. So if you have a population where the vaccination rates drop, those are exactly the kinds of areas where we need to do this surveillance.”
Racaniello echoed the importance of polio vaccination in adults as well. If patients don’t have a record of their shot, “just vaccinate them,” he said, “because there’s no downside to getting vaccinated again.”
Re-evaluating the Polio Endgame
The recent case of paralytic polio infection and concerns over the wider circulation of poliovirus have also altered some of the thinking around the goal of polio eradication.
In fact, William Schaffner, MD, of Vanderbilt University Medical Center in Nashville, highlighted the unique difficulty of preventing the spread of poliovirus.
“As you can imagine, we’ve gotten into polio endgame,” he told MedPage Today. “I think the notion has now been modified. Eradication isn’t going to be as neat and clean and quick as we once thought. Once we get rid of all paralytic disease, we will have to keep vaccinating for a long time, because there will still be circulating vaccine-associated viruses — some of which will mutate back.”
Schaffner compared the final push to eradicate polio with the successful eradication of smallpox. When the last case of smallpox ended, he explained, public health officials were able to end smallpox vaccination campaigns. For polio, however, he said, it will likely not be that simple, and it will be necessary “to keep vaccinating for quite a long time.”
He said that as public health officials in the U.S. and globally continue to grapple with the nuances of eradicating poliovirus, healthcare providers and their patients will have to come to terms with the simple fact that polio is a real health concern.
“[It’s] the reverse of the old saying, ‘it’s gone, but not forgotten,'” Schaffner said. “Polio is forgotten, but it’s not gone.”
Atul Gawande leads global health and is co-chair of the Covid-19 Task Force at the U.S. Agency for International Development.
Nearly a year ago, President Biden announced that the United States would be the “arsenal of vaccines for the world,” just as America served as an arsenal for democracies during World War II. With the president’s leadership and the consistent bipartisan support of Congress, the United States has delivered more than half a billion coronavirus vaccines to 114 lower-income countries free of charge, a historic accomplishment. This example spurred contributions from other wealthy nations and contributed to vaccination of almost 60 percent of the world.
But the global battle against covid-19 is not done. Instead, the challenge has changed. The lowest-income countries, where vaccinations have reached less than 15 percent of people, are now declining free vaccine supply because they don’t have the capacity to get shots in arms fast enough.
We must therefore not just provide an arsenal; to protect our allies against future variants, we must also provide the support they need to ramp up their vaccination campaigns. That effort requires money, and despite generously funding our covid-19 response up to this point, Congress is now failing to provide the resources we need.
I am writing to say: This bodes serious trouble for the world.
Despite a period of relative calm here at home, we’re again seeing cases and hospitalizations spike in Europe and Asia, even in places with higher levels of vaccination than the United States. These surges are due to the more-transmissible BA.2 subvariant of the already highly infectious omicron strain. Without additional funding, we risk not having the tools we need — vaccines, treatments, tests, masks and more — to manage future surges at home. And no less troubling, if we don’t close the vaccine gap between richer and poorer countries, we will give the virus more chances to mutate into a new variant.
Since the virus first emerged, the package of tools we’ve developed to fight it has proved resilient against all coronavirus variants. But there’s no guarantee that will remain true. A new variant that evades our defenses might once again fuel new surges of severe illness and batter the global economy. Helping all countries protect their populations by supercharging vaccination campaigns is our best hope to prevent future strains from emerging and ending this pandemic once and for all.
Turning vaccines into actual vaccinations has been difficult even in wealthy countries, where capable health systems, state-of-the-art cold chains and public awareness campaigns mean that anyone who wants a vaccine can get one. In countries without strong health infrastructure — without enough freezers and refrigerated trucks to keep vaccines from spoiling or enough health-care workers to reach rural populations living miles from the nearest health facility — it’s much tougher. We’ve also seen the same vaccine myths and disinformation that swirl through our media ecosystem spread just as rapidly through social media and hurt public trust abroad.
But we’ve also learned how to successfully tackle these challenges. In December, the Biden administration launched an initiative called Global VAX to help low-income countries train health workers, strengthen health infrastructure and raise vaccine access and awareness. While vaccine coverage in those countries remains far below the global average, the rapid progress we’ve supported in places such as Ivory Coast, Uganda and Zambia show what is possible when governments that are committed to fighting covid-19 have the global support they need.
Without more funding, we would have to halt our plans to expand the Global VAX initiative. The United States would have to turn its back on countries that need urgent help to boost their vaccination rates. And many countries that finally have the vaccines they need to protect their populations would risk seeing them spoil on the tarmac.
We can’t let this happen. It not only endangers people abroad but also risks the health and prosperity of all Americans. The virus is not waiting on Congress to negotiate; it is infecting people and mutating as we speak.
Over the past two years, both parties in Congress have repeatedly stepped up to fight covid-19 in an inspiring show of bipartisan unity. Now, we need our leaders to come together once more. With an effective strategy in place and the tools to transform covid-19 from a killer pandemic to a manageable respiratory disease, the United States has the expertise and capabilities the world needs to win the fight against this virus. We need Congress to let us take the fight to the front lines.
Over the next few weeks, the U.S. should expect an increase in cases from the BA.2 variant, Dr. Anthony Fauci told ABC News, but it may not lead to as severe a surge in hospitalizations or deaths.
“I would not be surprised if in the next few weeks we see somewhat of either a flattening of our diminution or maybe even an increase,” Fauci told ABC News’ Brad Mielke on the podcast “Start Here.”
His prediction is based on conversations with colleagues in the U.K., which is currently seeing a “blip” in cases, Fauci said. The pandemic trajectory in the U.S. has often followed the U.K. by about three weeks.
However, he added, “Their intensive care bed usage is not going up, which means they’re not seeing a blip up of severe disease.”
The BA.2 variant, a more transmissible strain of omicron, now represents around 23% of all cases in the U.S., according to the latest data from the Centers for Disease Control and Prevention.
And while Fauci predicted that the BA.2 variant will eventually overtake omicron as the most dominant variant, it’s not yet clear how much of a problem that will be.
“Whether or not that is going to lead to another surge, a mini surge or maybe even a moderate surge, is very unclear because there are a lot of other things that are going on right now,” Fauci said.
Similar to the U.K., much of the U.S. has recently relaxed mitigation efforts like mask mandates and requirements for proof of vaccination. At the same time, people who were vaccinated over six months ago and still haven’t gotten a booster shot, which is about half of vaccinated Americans, according to the CDC, are facing continuously waning immunity.
It’s also not yet clear how long immunity from prior infection will last, Fauci said.
Taken together, it’s why Fauci and other experts, including CDC Director Rochelle Walensky, have increasingly predicted that elderly people will need a second booster shot soon. The Food and Drug Administration began reviewing data from Pfizer on the safety and efficacy this week, and its advisory panel will debate if and when the additional booster shot is necessary in the coming weeks.
At the same time, Fauci urged Americans who haven’t yet gotten their first booster, which would be their third shot in a Pfizer or Moderna series, to do so.
A resurgence of cases could also mean Americans are asked to wear masks again, which Fauci predicted would be an uphill battle.
“From what I know about human nature, which I think is pretty much a lot, people are kind of done with COVID,” Fauci said.
Still, he defended the CDC decision to loosen its mask recommendations earlier this month by shifting to a strategy that focused more on severe outcomes, like hospitalizations and deaths, rather than on daily case spread.
“You can go ahead and continue to tiptoe towards normality, which is what we’re doing, but at the same time, be aware that you may have to reverse,” Fauci said.
And if the U.S. does continue to make its way back toward normal times, Fauci himself has a personal choice to consider. At 81 years old, the director of the National Institute of Allergy and Infectious Diseases is “certainly” thinking about retirement.
“I have said that I would stay in what I’m doing until we get out of the pandemic phase and I think we might be there already, if we can stay in this,” Fauci said, referring to the falling cases and hospitalizations in the U.S.
“I can’t stay at this job forever. Unless my staff is gonna find me slumped over my desk one day. I’d rather not do that,” he said, laughing.
While he doesn’t currently have retirement plans, the recent hire of Dr. Ashish Jha, dean of the Brown University School of Public Health, to be White House coronavirus coordinator, could alleviate some of his pandemic response duties and give him a window.
But Fauci, who has dedicated his career to public health, primarily studying HIV and AIDS, and worked under seven U.S. presidents, said he doesn’t have any particular hobbies waiting for him in retirement.
“I, unfortunately, am somewhat of a unidimensional physician, scientist, public health person. When I do decide I’m going to step down, whenever that is, I’m going to have to figure out what it is I’m going to do,” he said.
“I’d love to spend more time with my wife and family. That would really be good.”