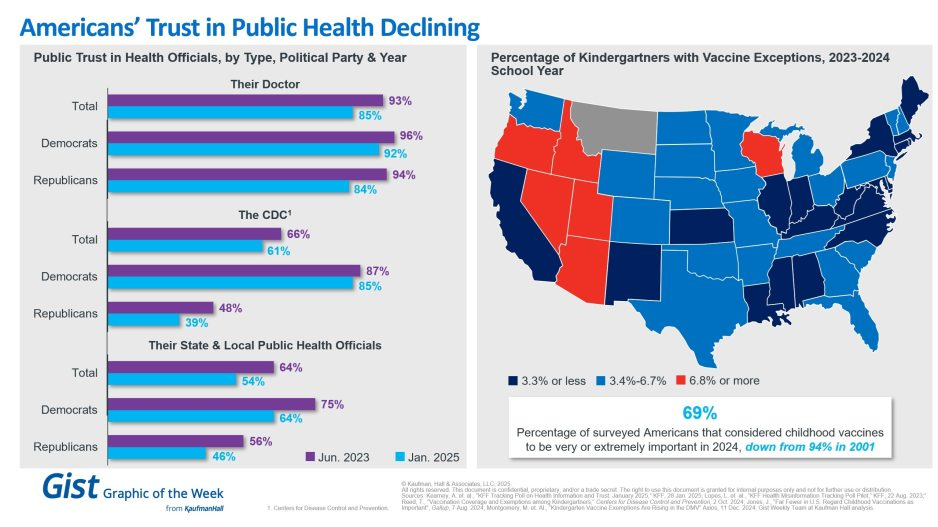
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
Gun violence is a public health problem, but we don’t approach it like one. The debate often gets framed as “guns or no guns” when it isn’t that black and white. In this episode we break down how and why to approach gun violence as a public health problem, what the current research has to say, and what we need to move forward.
The right to bear arms has existed since we became a nation. So, too, has the risk of violence that extensive gun ownership creates in our society.
Unfortunately, recent mass shooting incidents, fueled by hatred or mental illness, have sparked a great deal of fear and confusion among Americans.
As healthcare leaders, our concern centers on the treatment of those who are victims of senseless gun violence. And not just those who are shot, but the other victims as well.
Healthcare providers must care for all victims — the ones who are traumatized because a loved one has been hurt or lost, the ones who were at the chaotic scene of the violence, or who are haunted by the endless media stories they cannot seem to tune out. The emotional toll of this violence is incomprehensible.
Healthcare facilities attempt to provide refuge from violence and seek to provide healing and hope to all victims of violence.
Unstable individuals with guns and other weapons of harm find their way into our buildings and hallways as well. Earlier this month, a man who blamed his physician for ongoing pain after a recent back surgery shot and killed his surgeon and three other people before fatally shooting himself in a Tulsa, Okla., medical facility. Also this month, a hospital security officer was shot and killed by a prison inmate who was receiving care in a Dayton, Ohio, emergency room.
These incidents are the latest horrifying tragedies in a wave of deadly gun violence occurring across our country, including two heart-breaking mass shootings in Buffalo, N.Y., and Uvalde, Texas. We mention these tragedies not to make a political statement, but to raise awareness of the consequences of this violence on healthcare providers and the public health.
As healthcare workers, healers, and caregivers, we work to fix what is broken and put people back together. We bring solutions. We engage with our hearts to stand together in the fear and vulnerabilities of those who need us so that we can help them through difficult challenges. We look to bring light to dark situations. We seek to be beacons of hope.
The escalation of recent shootings, suicides and other violent behaviors underscores the urgency for a national conversation on what has become a serious public health crisis. We believe health systems have a credible voice and can play a critical role beyond being places to physically and emotionally care for the victims of violence.
It’s easy to allow ourselves to become numb to the frequency of these unconscionable, violent acts. But we owe it to present and future generations not to let that happen. We recognize there are no easy answers to this national problem. After all, we are dealing with abnormal behavior — the decision to seriously harm or kill other people. That this behavior is increasing calls for something to be done to effect positive change.
People across our country and the communities we serve are hurting and vulnerable. Many people are weary from the pandemic that has impacted our hearts and our health. Violence and death, and particularly mass shootings, hit adults hard. Now consider what the prevalence and threat of school shootings have done to an entire generation of children, who are growing up with the fear of being shot and killed in a place they should feel safe.
We all can play a role. Recently, our two organizations decided to do something to reduce gun violence by sponsoring a law enforcement gun buyback program to help get guns off the street. This effort was part of the largest single-day gun buyback in New Jersey state history. It successfully removed over 2,800 guns statewide. Private organizations, companies, and individuals must think of additional creative ways beyond criticizing politicians, to bring about the change we need.
We encourage organizations and communities to come together, to pool their minds and their resources to address gun violence in society as the urgent public health crisis that it is. We must create meaningful public health campaigns around the safe storage and handling of firearms, and sensible and innovative ways to prevent gun violence in schools, healthcare settings and public places. Individuals should educate themselves on the issues surrounding gun violence so they may contribute to the effort to bring about necessary and meaningful change.
And yes, we need to accelerate efforts around our nation’s mental health crisis. We know from the data and what we are all experiencing that the COVID-19 pandemic has exacerbated what was already a growing nationwide mental health crisis.
Violence against any person in any venue is unspeakable. Yet just because it is unspeakable does not mean we should not speak up about it. Let us put our anger, shock and heartbreak into positive change. With the same unstoppable resolution that we seek to cure cancer or slow heart disease, let us advocate, educate and take meaningful action to end gun violence and all senseless violence that is taking such a tragic toll on our nation and our wellbeing.
About Virtua Health Virtua Health is an academic health system committed to helping the people of South Jersey be well, get well, and stay well by providing the complete spectrum of advanced, accessible, and trusted healthcare services. Virtua’s 14,000 colleagues provide tertiary care, including renowned cardiology and transplant programs, complemented by a community-based care portfolio. In addition to five hospitals, two satellite emergency departments, 30 ambulatory surgery centers, and more than 300 other locations, Virtua brings health services directly into communities through Hospital at Home, physical therapy and rehabilitation, mobile screenings, and its paramedic program. Virtua has 2,850 affiliated doctors and other clinicians, and its specialties include orthopedics, advanced surgery, and maternity. Virtua is academically affiliated with Rowan University, leading research, innovation, and immersive education at the Virtua Health College of Medicine & Health Sciences of Rowan University. Virtua is also affiliated with Penn Medicine for cancer and neuroscience, and the Children’s Hospital of Philadelphia for pediatrics. As a not-for-profit, Virtua is committed to the well-being of the community and provides innovative outreach programs that address social challenges affecting health, most notably the “Eat Well” food access initiative, which includes the unparalleled Eat Well Mobile Grocery Store. A Magnet-recognized health system ranked by U.S. News and World Report, Virtua has received many awards for quality, safety, and its outstanding work environment. For more information, visit Virtua.org. To help Virtua make a difference, visit GiveToVirtua.org.
About Cooper University Health Care Cooper University Health Care is a leading academic health system with more 8,500 employees and more than 800 employed physicians. Cooper University Hospital is the only Level 1 Trauma Center in South Jersey and the busiest in the region. Annually, nearly two million patients are served at Cooper’s 635-bed flagship hospital, outpatient surgery center, three urgent care centers, and more than 105 ambulatory offices throughout the community. The Cooper Health Sciences campus is home to Cooper University Hospital, MD Anderson Cancer Center at Cooper, Children’s Regional Hospital at Cooper, and Cooper Medical School of Rowan University. Visit CooperHealth.org to learn more.
Only 10 days after a racially motivated mass shooting that killed 10 in a Buffalo, NY grocery store, 19 children and two teachers were murdered on Tuesday at an elementary school in Uvalde, TX. The Uvalde shooting was the 27th school shooting, and one of over 212 mass shootings, that have occurred this year alone.
Firearms recently overtook car accidents as the leading cause of childhood deaths in the US, and more than 45,000 Americans die from gun violence each year.
The Gist: Gun violence is, and has long been, a serious public health crisis in this country. It is both important to remember, yet difficult for some to accept, that many mass shootings are preventable.
Health systems, as stewards of health in their communities, can play a central role in preventing gun violence at its source, both by bolstering mental health services and advocating for the needed legislative actions—supported by a strong majority of American voters—to stem this public health crisis.
As Northwell Health CEO Michael Dowling said this week, “Our job is to save lives and prevent people from illness and death. Gun violence is not an issue on the outside—it’s a central public health issue for us. Every single hospital leader in the United States should be standing up and screaming about what an abomination this is. If you were hesitant about getting involved the day before…May 24 should have changed your perspective. It’s time.”
But officials caution that people should not presume they have protection against the virus going forward.
Before omicron, one-third of Americans had been infected with the coronavirus, but by the end of February, that rate had climbed to nearly 60 percent — including about 75 percent of kids and 60 percent of people age 18 to 49, according to federal health data released Tuesday.
The data from blood tests offers the first evidence that over half the U.S. population, or 189 million people have been infected at least once since the pandemic began — double the number reflected in official case counts. Officials cautioned, however, that the data, in a report from the Centers for Disease Control and Prevention, does not indicate people have protection against the virus going forward, especially against increasingly transmissible variants.
“We continue to recommend that everyone be up to date on their vaccinations, get your primary series and booster, when eligible,” CDC Director Rochelle Walensky said during a media briefing.
Kristie Clarke, the CDC official who authored the report, said by February, “evidence of previous COVID-19 infections substantially increased among every age group, likely reflecting the increase in cases we noted as omicron surged in this country.”
Clarke said the greatest increases took place in those with the lowest levels of vaccination, noting that older adults were more likely to be fully vaccinated.
The largest increases were in children and teenagers through age 17 — about 75 percent of them had been infected by February, based on blood samples that look at antibodies developed in response to a coronavirus infection but not in response to vaccination. That’s about 58 million children.
The blood test data suggests 189 million Americans had covid-19 by end of February, well over double the 80 million cases shown by The Washington Post case tracker, which is based on state data of confirmed infections. Clarke said that’s because the blood tests captures asymptomatic cases and others that were never confirmed on coronavirus tests.
With the omicron surge, officials had expected there would be more infections. “But I didn’t expect the increase to be quite this much,” Clarke added.
Separately, CDC is about to publish another study that estimates three infections for every reported case, she said.
This week the Biden Administration unveiled actions to make at-home COVID tests and N95 masks available, free of charge, to hundreds of millions of Americans. However, even as US COVID hospitalizations have now surpassed last winter’s previous peak, two newly-approved COVID antiviral drugs remain scarce. Just as fast as Omicron has surged across the country, it may be starting to recede, with cases beginning to drop in several states in the Northeast. Modelers now project the incredibly contagious variant will infect 40 percent of Americans and more than half the human race by the end of March.
The Gist:Absent another significant variant, experts are cautiously optimistic that enough of the US population will soon have either infection-acquired or vaccine-induced immunity that we may be nearing the end of the pandemic, and the beginning of “endemic COVID.”
The US must now shift from COVID “war footing” to learning how to live with the virus long term. That will mean tackling difficult and politically-charged decisions, such as what level of testing and masking are sustainable, and how many COVID deaths we are willing to tolerate.
The latest Omicron developments continue to be encouraging. New Covid-19 cases are plummeting in a growing list of places. The percentage of cases causing severe illness is much lower than it was with the Delta variant. And vaccines — particularly after a booster shot — remain extremely effective in preventing hospitalization and death.
I also think it’s time to begin considering what life after the Omicron wave might look like.
1. Plunging cases
Since early last week, new cases in Connecticut, Maryland, New Jersey and New York have fallen by more than 30 percent. They’re down by more than 10 percent in Colorado, Florida, Georgia, Massachusetts and Pennsylvania. In California, cases may have peaked.
“Let’s be clear on this — we are winning,” Mayor Eric Adams of New York said yesterday. Kathy Hochul, the governor of New York State, said during a budget speech, “We hope to close the books on this winter surge soon.”
If anything, the official Covid numbers probably understate the actual declines, because test results are often a few days behind reality.
The following data comes from Kinsa, a San Francisco company that tracks 2.5 million internet-connected thermometers across the country. It uses that data to estimate the percentage of Americans who have a fever every day. The declines over the past week have been sharp, which is a sign of Omicron’s retreat:
Many hospitals are still coping with a crushing number of patients, because Covid hospitalization trends often trail case trends by about a week. But even the hospital data shows glimmers of good news: The number of people hospitalized with Covid has begun declining over the past few days in places where Omicron arrived first:
The U.S. seems to be following a similar Omicron pattern as South Africa, Britain and several other countries: A rapid, enormous surge for about a month, followed by a rapid decline — first in cases, then hospitalizations and finally deaths.
Some of the clearest research on Covid’s risks comes from a team of British researchers led by Dr. Julia Hippisley-Cox of the University of Oxford. The team has created an online calculator that allows you to enter a person’s age, vaccination status, height and weight, as well as major Covid risk factors. (It’s based on an analysis of British patients, but its conclusions are relevant elsewhere.)
A typical 65-year-old American woman — to take one example — is five foot three inches tall and weighs 166 pounds. If she had been vaccinated and did not have a major Covid risk factor, like an organ transplant, her chance of dying after contracting Covid would be 1 in 872, according to the calculator. For a typical 65-year-old man, the risk would be 1 in 434.
Among 75-year-olds, the risk would be 1 in 264 for a typical woman and 1 in 133 for a typical man.
Those are meaningful risks. But they are not larger than many other risks older people face. In the 2019-20 flu season, about 1 out of every 138 Americans 65 and older who had flu symptoms died from them, according to the C.D.C.
And Omicron probably presents less risk than the British calculator suggests, because it uses data through the first half of 2021, when the dominant version of Covid was more severe than Omicron appears to be. One sign of Omicron’s relative mildness: Among vaccinated people in Utah (a state that publishes detailed data), the percentage of cases leading to hospitalization has been only about half as high in recent weeks as it was last summer.
For now, the available evidence suggests that Omicron is less threatening to a vaccinated person than a normal flu. Obviously, the Omicron wave has still been damaging, because the variant is so contagious that it has infected tens of millions of Americans in a matter of weeks. Small individual risks have added up to large societal damage.
3. Effective boosters
The final major piece of encouraging news involves booster shots: They are highly effective at preventing severe illness from Omicron. The protection is “remarkably high,” as Dr. Eric Topol of Scripps Research wrote.
Switzerland has begun reporting Covid deaths among three different groups of people: the unvaccinated; the vaccinated who have not received a booster shot; and the vaccinated who have been boosted (typically with a third shot). The first two shots still provide a lot of protection, but the booster makes a meaningful difference, as Edouard Mathieu and Max Roser of Our World in Data have noted:
The next stage
The Covid situation in the U.S. remains fairly grim, with overwhelmed hospitals and nearly 2,000 deaths a day. It’s likely to remain grim into early February. Caseloads are still high in many communities, and death trends typically lag case trends by three weeks.
But the full picture is less grim than the current moment.
Omicron appears to be in retreat, even if the official national data doesn’t yet reflect that reality. Omicron also appears to be mild in a vast majority of cases, especially for the vaccinated. This combination means that the U.S. may be only a few weeks away from the most encouraging Covid situation since early last summer, before the Delta variant emerged.
If that happens — and there is no guarantee it will, as Katherine Wu of The Atlantic explains — it will be time to ask how society can move back toward normalcy and reduce the harsh toll that pandemic isolation has inflicted, particularly on children and disproportionately on low-income children.
When should schools resume all activities? When should offices reopen? When should masks come off? When should asymptomatic people stop interrupting their lives because of a Covid exposure? Above all, when does Covid prevention do more harm — to physical and mental health — than good?
These are tricky questions, and they could often sound inappropriate during the Omicron surge. Now, though, the surge is receding.
Even as daily new COVID cases set all-time records and hospitals fill up, epidemiologists have arrived at a perhaps surprising consensus. Yes, the latest Omicron variant of the novel coronavirus is bad. But it could have been a lot worse.
Even as cases have surged, deaths haven’t—at least not to the same degree. Omicron is highly transmissible but generally not as severe as some older variants—“lineages” is the scientific term.
We got lucky. But that luck might not hold. Many of the same epidemiologists who have breathed a sigh of relief over Omicron’s relatively low death rate are anticipating that the next lineage might be much worse.
Fretting over a possible future lineage that combines Omicron’s extreme transmissibility with the severity of, say, the previous Delta lineage, experts are beginning to embrace a new public health strategy that’s getting an early test run in Israel: a four-shot regimen of messenger-RNA vaccine.
“I think this will be the strategy going forward,” Edwin Michael, an epidemiologist at the Center for Global Health Infectious Disease Research at the University of South Florida, told The Daily Beast.
Omicron raised alarms in health agencies all over the world in late November after officials in South Africa reported the first cases. Compared to older lineages, Omicron features around 50 key mutations, some 30 of which are on the spike protein that helps the virus to grab onto our cells.
Some of the mutations are associated with a virus’s ability to dodge antibodies and thus partially evade vaccines. Others are associated with higher transmissibility. The lineage’s genetic makeup pointed to a huge spike in infections in the unvaccinated as well as an increase in milder “breakthrough” infections in the vaccinated.
That’s exactly what happened. Health officials registered more than 10 million new COVID cases the first week of January. That’s nearly double the previous worst week for new infections, back in May. Around 3 million of those infections were in the United States, where Omicron coincided with the Thanksgiving, Christmas, and New Year holidays and associated traveling and family gatherings.
But mercifully, deaths haven’t increased as much as cases have. Worldwide, there were 43,000 COVID deaths the first week of January—fewer than 10,000 of them in the U.S. While deaths tend to lag infections by a couple weeks, Omicron has been dominant long enough that it’s increasingly evident there’s been what statisticians call a “decoupling” of cases and fatalities.
“We can say we dodged a bullet in that Omicron does not appear to cause as serious of a disease,” Stephanie James, the head of a COVID testing lab at Regis University in Colorado, told The Daily Beast. She stressed that data is still being gathered, so we can’t be certain yet that the apparent decoupling is real.
Assuming the decoupling is happening, experts attribute it to two factors. First, Omicron tends to infect the throat without necessarily descending to the lungs, where the potential for lasting or fatal damage is much, much higher. Second, by now, countries have administered nearly 9.3 billion doses of vaccine—enough for a majority of the world’s population to have received at least one dose.
In the United States, 73 percent of people have gotten at least one dose. Sixty-two percent have gotten two doses of the best mRNA vaccines. A third have received a booster dose.
Yes, Omicron has some ability to evade antibodies, meaning the vaccines are somewhat less effective against this lineage than they are against Delta and other older lineages. But even when a vaccine doesn’t prevent an infection, it usually greatly reduces its severity.
For many vaccinated people who’ve caught Omicron, the resulting COVID infection is mild. “A common cold or some sniffles in a fully vaxxed and boosted healthy individual,” is how Eric Bortz, a University of Alaska-Anchorage virologist and public health expert, described it to The Daily Beast.
All that is to say, Omicron could have been a lot worse. Viruses evolve to survive. That can mean greater transmissibility, antibody-evasion or more serious infection. Omicron mutated for the former two. There’s a chance some future Sigma or Upsilon lineage could do all three.
When it comes to viral mutations, “extreme events can occur at a non-negligible rate, or probability, and can lead to large consequences,” Michael said. Imagine a lineage that’s as transmissible as Omicron but also attacks the lungs like Delta tends to do. Now imagine that this hypothetical lineage is even more adept than Omicron at evading the vaccines.
That would be the nightmare lineage. And it’s entirely conceivable it’s in our future. There are enough vaccine holdouts, such as the roughly 50 million Americans who say they’ll never get jabbed, that the SARS-CoV-2 pathogen should have ample opportunities for mutation.
“As long as we have unvaccinated people in this country—and across the globe—there is the potential for new and possibly more concerning viral variants to arise,” Aimee Bernard, a University of Colorado immunologist, told The Daily Beast.
Worse, this ongoing viral evolution is happening against a backdrop of waning immunity. Antibodies, whether vaccine-induced or naturally occurring from past infection, fade over time. It’s not for no reason that health agencies in many countries urge booster doses just three months after initial vaccination. The U.S. Centers for Disease Control and Prevention is an outlier, and recommends people get boosted after five months.
A lineage much worse than Omicron could evolve at the same time that antibodies wane in billions of people all over the world. That’s why many experts believe the COVID vaccines will end up being annual or even semi-annual jabs. You’ll need a fourth jab, a fifth jab, a sixth jab, et cetera, forever.
Israel, a world leader in global health, is already turning that expectation into policy. Citing multiple studies that showed a big boost in antibodies with an additional dose of mRNA and no safety concerns, the country’s health ministry this week began offering a fourth dose to anyone over the age of 60, who tend to be more vulnerable to COVID than younger people.
That should be the standard everywhere, Ali Mokdad, a professor of health metrics sciences at the University of Washington Institute for Health, told The Daily Beast. “Scientifically, they’re right,” he said of the Israeli health officials.
If there’s a downside, it’s that there are still a few poorer countries—in Africa, mostly—where many people still struggle to get access to any vaccine, let alone boosters and fourth doses. If and when other richer countries follow Israel’s lead and begin offering additional jabs, there’s some risk of even greater inequity in global vaccine distribution.
“The downside is for the rest of the world,” Mokdad said. “I’m waiting to get my first dose and you guys are getting a fourth?”
The solution isn’t to deprive people of the doses they need to maintain their protection against future—and potentially more dangerous—lineages. The solution, for vaccine-producing countries, is to further boost production and double down on efforts to push vaccines out to the least privileged communities.
A sense of urgency is key. For all its rapid spread, Omicron has actually gone fairly easy on us. Sigma or Upsilon might not.