In 63 days, Americans will know the composition of the 119th Congress and the new occupants of the White House and 11 Governor’s mansions. We’ll learn results of referenda in 10 states about abortion rights (AZ, CO, FL, MD, MO, MT, NE, NV, NY, SD) and see how insurance coverage for infertility (IVF therapy) fares as Californians vote on SB 729. But what we will not learn is the future of the U.S. health system at a critical time of uncertainty.
In 6 years, every baby boomer will be 65 years of age or older. In the next 20 years, the senior population will be 22% of the population–up from 18% today. That’s over 83 million who’ll hit the health system vis a vis Medicare while it is still digesting the tsunami of obesity, a scarcity of workers and unprecedented discontent:
- The majority of voters is dissatisfied with the status quo. 69% think the system is fundamentally flawed and in need of major change vs. 7% who think otherwise. 60% believe it puts its profits above patient care vs. 13% who disagree.
- Employers are fed up: Facing projected cost increases of 9% for employee coverage in 2025, they now reject industry claims of austerity when earnings reports and executive compensation indicate otherwise. They’re poised to push back harder than ever.
- Congress is increasingly antagonistic: A bipartisan coalition in Congress is pushing populist reforms unwelcome by many industry insiders i.e. price transparency for hospitals, price controls for prescription drugs, limits on private equity ownership, constraint on hospital, insurer and physician consolidation, restrictions on tax exemptions of NFP hospitals, site neutral payment policies and many more.
Fanning these flames, media characterizations of targeted healthcare companies as price gouging villains led by highly-paid CEOs is mounting: last week, it was Acadia Health’s turn courtesy of the New York Times’ investigators.
Navigating uncertainty is tough for industries like healthcare where demand s growing, technologies are disrupting how and where services are provided and by whom, and pricing and affordability are hot button issues. And it’s too big to hide: at $5.049 trillion, it represents 17.6% of the U.S. GDP today increasing to 19.7% by 2032. Growing concern about national debt puts healthcare in the crosshairs of policymaker attention:
Per the Committee for a Responsible Federal Budget: “In the latest Congressional Budget Office (CBO) baseline, nominal spending is projected to grow from $6.8 trillion in Fiscal Year (FY) 2024 to $10.3 trillion in 2034. About 87% of this increase is due to three parts of the federal budget: Social Security, federal health care programs, and interest payments on the debt.”
In response, Boards in many healthcare organizations are hearing about the imperative for “transformational change” to embrace artificial intelligence, whole person health, digitization and more. They’re also learning about ways to cut their operating costs and squeeze out operating margins. Bold, long-term strategy is talked about, but most default to less risky, short-term strategies compatible with current operating plans and their leaders’ compensation packages. Thus, “transformational change” takes a back seat to survival or pragmatism for most.
For Boards of U.S. healthcare organizations, the imperative for transformational change is urgent: the future of the U.S. system is not a repeat of its past. But most Boards fail to analyze the future and construct future-state scenarios systematically. Lessons from other industries are instructive.
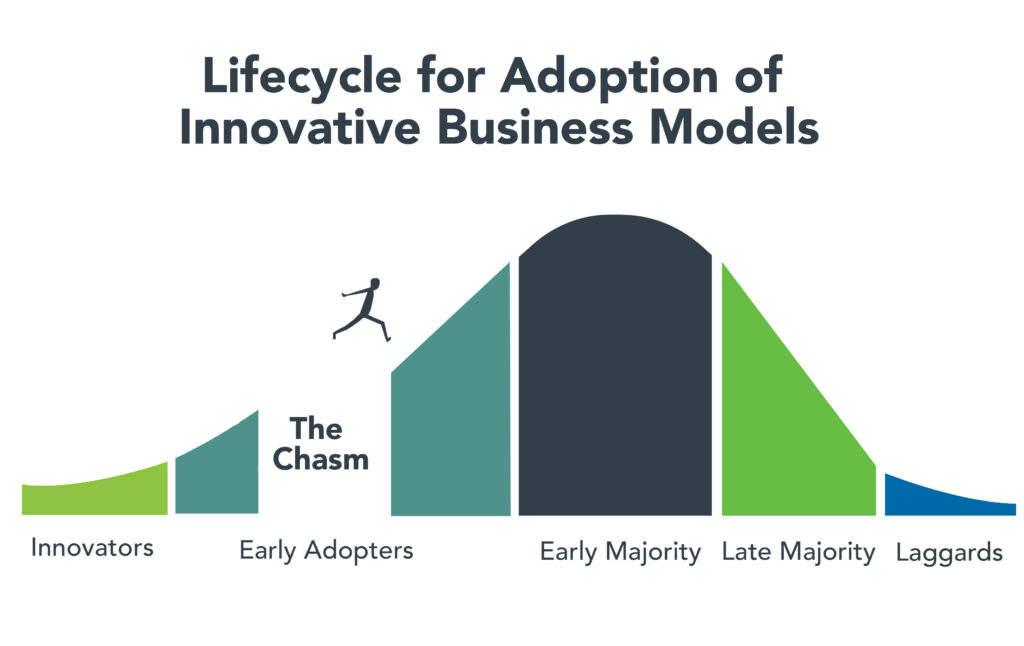
- Transformational change in mission critical industries occurs over a span of 20-25 years. It starts with discontent with the status quo, then technologies and data that affirm plausible alternatives and private capital that fund scalable alternatives. It’s not overnight.
- Transformational change is not paralyzed by regulatory hurdles. Transformers seek forgiveness, not permission while working to change the regulatory landscape. Advocacy is a critical function in transformer organizations.
- Transformation is welcomed by consumers. Recognition of improved value by end-users—individual consumers—is what institutionalizes transformational success. Transformed industries define success in terms of the specific, transparent and understandable results of their work.
Per McKinsey, only one in 8 organizations is successful in fully implementing transformational change completely but the reward is significant: transformers outperform their competition three-to-one on measures of growth and effectiveness.
I am heading to Colorado Springs this weekend for the Governance Institute. There, I will offer Board leaders four basic questions.
- Is the future of the U.S. health system a repeat of the past or something else?
- How will its structure, roles and responsibilities change?
- How will affordability, quality, innovation and value be defined and validated?
- How will it be funded?
Answers to these require thoughtful discussion. They require independent judgement. They require insight from organizations outside healthcare whose experiences are instructive. They require fresh thinking.
Until and unless healthcare leaders recognize the imperative for transformational change, the system will calcify its victim-mindset and each sector will fend for itself with diminishing results. No sector—hospitals, insurers, drug companies, physicians—has all the answers and every sector faces enormous headwinds. Perhaps it’s time for a cross-sector coalition to step up with transformational change as the goal and the public’s well-being the moral compass.
PS: Last week, I caught up with Drs. Steve and Pat Gabbe in Columbus, Ohio. Having served alongside them at Vanderbilt and now as an observer of their work at Ohio State, I am reminded of the goodness and integrity of those in healthcare who devote their lives to meaningful, worthwhile work. Steve “burns with a clear blue flame” as a clinician, mentor and educator. Pat is the curator of a program, Moms2B, that seeks to alleviate Black-White disparities in infant mortality and maternal child health in Ohio. They’re great people who see purpose in their calling; they’re what make this industry worth fixing!