The U.S. health care industry is approaching a critical inflection point, according to veteran health care strategist Paul Keckley. In a candid and thought-provoking keynote at the 2025 Healthcare Marketing & Physician Strategies Summit (HMPS) in Orlando, Keckley outlined the challenges and potential opportunities health care leaders must navigate in an era of unprecedented economic uncertainty, regulatory disruption, and consumer discontent.
Drawing on decades of policy experience and his signature candid style, Keckley delivered a sobering yet actionable assessment of where the industry stands and what lies ahead.
Paul Keckley, PhD, health care research and policy expert and managing editor of The Keckley Report
Health care now accounts for a staggering 28 percent of the federal budget, with Medicaid expenditures alone ranging from the low 20s to 34 percent of individual state budgets. Despite its fiscal significance, Keckley points out that health care remains “not really a system, but a collection of independent sectors that cohabit the economy.”
In the article that follows, Keckley warns of a reckoning for those who remain entrenched in legacy assumptions. On the flip side, he notes, “The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
A Fractured System in a Fractured Economy
Fragmentation complicates any effort to meaningfully address rising costs or care quality. It also heightens the stakes in a political climate marked by what Keckley termed “MAGA, DOGE, and MAHA” factions, shorthand for various ideological forces shaping health care policy under the Trump 2.0 administration.
Meanwhile, macroeconomic conditions are only adding to the strain. At the time of Keckley’s address, the S&P 500 was down 8 percent, the Dow down 10 percent, and inflationary pressures were squeezing both provider margins and household budgets.
“Economic uncertainty is not just about Wall Street,” Keckley warns. “It’s about kitchen-table economics — how households decide between paying for care or paying the cable bill.”
Traditional Forecasting Is Failing
One of Keckley’s key messages was that conventional methods of strategic planning in health care, based on lagging indicators like utilization rates and demographics, are no longer sufficient. Instead, leaders must increasingly look to external forces such as capital markets, regulatory volatility, and consumer behavior.
“Think outside-in,” he urges. “Forces outside health care are shaping its future more than forces within.”
He encourages health systems to go beyond isolated market studies and adopt holistic scenario planning that considers clinical innovation, workforce shifts, AI and tech disruption, and capital availability as interconnected variables.
Affordability and Accountability: The Hospital Reckoning
Keckley pulls no punches in addressing the mounting criticism of hospitals on Capitol Hill, particularly not-for-profit health systems. Public perception is faltering, with hospital pricing increasing faster than other categories in health care and only a third of providers in full compliance with price transparency rules.
“Economic uncertainty is not just about Wall Street. It’s about kitchen-table economics — how households decide between paying for care or paying the cable bill.”
“We have to get honest about trust, transparency, and affordability,” he says. “I’ve been in 11 system strategy sessions this year. Only one even mentioned affordability on their website, and none defined it.”
Keckley also predicts that popular regulatory targets like site-neutral payments, the 340B program, and nonprofit tax exemptions will face intensified scrutiny.
“Hospitals are no longer viewed as sacred institutions,” he says. “They’re being seen as part of the problem, especially by younger, more educated, and more skeptical Americans.”
The Consumer Awakens
Perhaps the most urgent shift Keckley outlines is the redefinition of the health care consumer. “We call them patients,” he says, “but they are consumers. And they are not happy.”
Keckley cites polling data showing that two out of three Americans believe the health care system needs to be rebuilt from the ground up. Roughly 40 percent of U.S. households have at least one unpaid medical bill, with many choosing intentionally not to pay. Among Gen Y and younger households, dissatisfaction is particularly acute.
“[Consumers] expect digital, personalized, seamless experiences — and they don’t understand why health care can’t deliver.”
These consumers aren’t just passive recipients of care; they’re voters, payers, and critics. With 14 percent of health care spending now coming directly from households, Keckley argues, health systems must engage consumers with the same sophistication that retail and tech companies use.
“They expect digital, personalized, seamless experiences — and they don’t understand why health care can’t deliver.”
Tech Disruption Is Real
Keckley underscores the transformative potential of AI and emerging clinical technologies, noting that in the next five years, more than 60 GLP-1-like therapeutic innovations could come to market. But the deeper disruption, he warns, is likely to come from outside the traditional industry.
Citing his own son’s work at Microsoft, Keckley envisions a future where a consumer’s smartphone, not a provider or insurer, is the true hub of health information. “Health care data will be consumer-controlled. That’s where this is headed.”
The takeaway for providers: Embrace data interoperability and consumer-centric technology now, or risk irrelevance. “The Amazons and Apples of the world are not waiting for CMS to set the rules,” Keckley says.
Capital, Consolidation, and Private Equity
Capital constraints and the shifting role of private equity also featured prominently in Keckley’s remarks. With declining non-operating revenue and shrinking federal dollars, some health systems increasingly rely on investor-backed funding.
But this comes with reputational and operational risks. While PE investments have been beneficial to shareholders, Keckley says, they’ve also produced “some pretty dire results for consumers” — particularly in post-acute care and physician practice consolidation.
“Policymakers are watching,” he says. “Expect legislation that will limit or redefine what private equity can do in health care.”
Politics and Optics: Navigating the Policy Minefield
In the regulatory arena, Keckley emphasizes that perception often matters more than substance. “Optics matter often more than the policy itself,” he says.
He cautions health leaders not to expect sweeping policy reform but to brace for “de jure chaos” as the current administration focuses on symbolic populist moves — cutting executive compensation, promoting price transparency, and attacking nonprofit tax exemptions.
With the 2026 midterm elections looming large, Keckley predicts a wave of executive orders and rhetorical grandstanding. But substantive policy change will be incremental and unpredictable.
“Don’t wait for a rescue from Washington. The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
The Workforce Crisis That Wasn’t Solved
Keckley also addresses the persistent shortage of health care workers and the failure of Title V of the ACA, which had promised to modernize the workforce through new team-based models. “Our guilds didn’t want it,” Keckley notes, bluntly. “So nothing happened.”
He argues that states, not the federal government, will drive the next chapter of workforce reform, expanding the scope of practice for pharmacists, nurse practitioners, and even lay caregivers, particularly in behavioral health and primary care.
What Should Leaders Do Now?
Keckley closed his keynote with a challenge for marketers and strategists: Get serious about defining affordability, understand capital markets, and stop defaulting to legacy assumptions.
“Don’t wait for a rescue from Washington,” he says. “The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
He encouraged leaders to monitor shifting federal org charts, track state-level policy moves, and scenario-plan for a future where trust, access, and consumer empowerment define success.
Conclusion: A Health Care Reckoning in the Making
Keckley’s keynote was more than a policy forecast; it was a wake-up call. In a landscape shaped by economic headwinds, political volatility, and consumer rebellion, health care leaders can no longer afford to stay in their lane. They must engage, adapt, and transform, or risk becoming casualties of a system under siege.
“Health care is not just one of 11 big industries,” Keckley says. “It’s the one that touches everyone. And right now, no one is giving us a standing ovation.”
During a fireside chat at AHIP 2024, Mary Langowski, executive vice president and president of U.S. healthcare at Walgreens Boots Alliance, said she sees a bright future for retail in healthcare.
Retailers are facing several headwinds in healthcare in 2024.Walmart and Dollar General both recently ended healthcare endeavors, and CVS Health is reportedly looking for a private equity partner for Oak Street Health (which it acquired in 2023). VillageMD, which is backed by Walgreens, is shuttering numerous clinics.
Still, Mary Langowski, executive vice president and president of U.S. healthcare at Walgreens Boots Alliance, sees a strong future for retailers in healthcare.
“I happen to be very bullish on the role of retail in healthcare and frankly, having a very central role in healthcare,” she said. “And part of that is because over 80% of people want health and wellness offerings in a pharmacy and in a retail setting. Consumers want the ease, they want the convenience of it. And those are important things to keep in mind, that demand is there.”
Langowski, who joined Walgreens in March, made these comments during a Tuesday fireside chat at the AHIP 2024 conference held in Las Vegas. She added that what the industry is seeing is not an “evolution” of whether retailers will exist in healthcare, but a shift around what the “right model is going to be.”
“We really think that if you take our core assets, … we can be a really good partner to not just one provider entity but many, many provider entities and payers across the United States,” Langowski said. “We’re everywhere. We’re in the community, we’re digitally inclined. I think a strategy for us is less capital-intensive, capital-light and very scaled models.”
She also told the health plans in the audience that she wants to collaborate more. She said she sees retail as a “really critical entry point” in the healthcare system.
“We have people using their pharmacists two times more than any doctor and Medicare patients see us eight times more than their physician,” Langowski declared. “We’re not doing enough together to take advantage of those moments where we can engage people and we can create interventions way earlier in their healthcare disease state.”
Langowski noted that insurers are under a lot of pressure, including rising costs, regulatory issues and challenges contracting with providers. However, Walgreens’ assets are “highly complementary” to insurers’ assets, she said.
“We aren’t going to do what you do. You don’t do what we do, but we work really well together,” she said. “And what it will take is being clever about the commercial and economic model and I believe there are multiple ways to create win-win scenarios where everybody does well. Most importantly, patients get healthier and they have a much better and much more seamless experience with the system.”
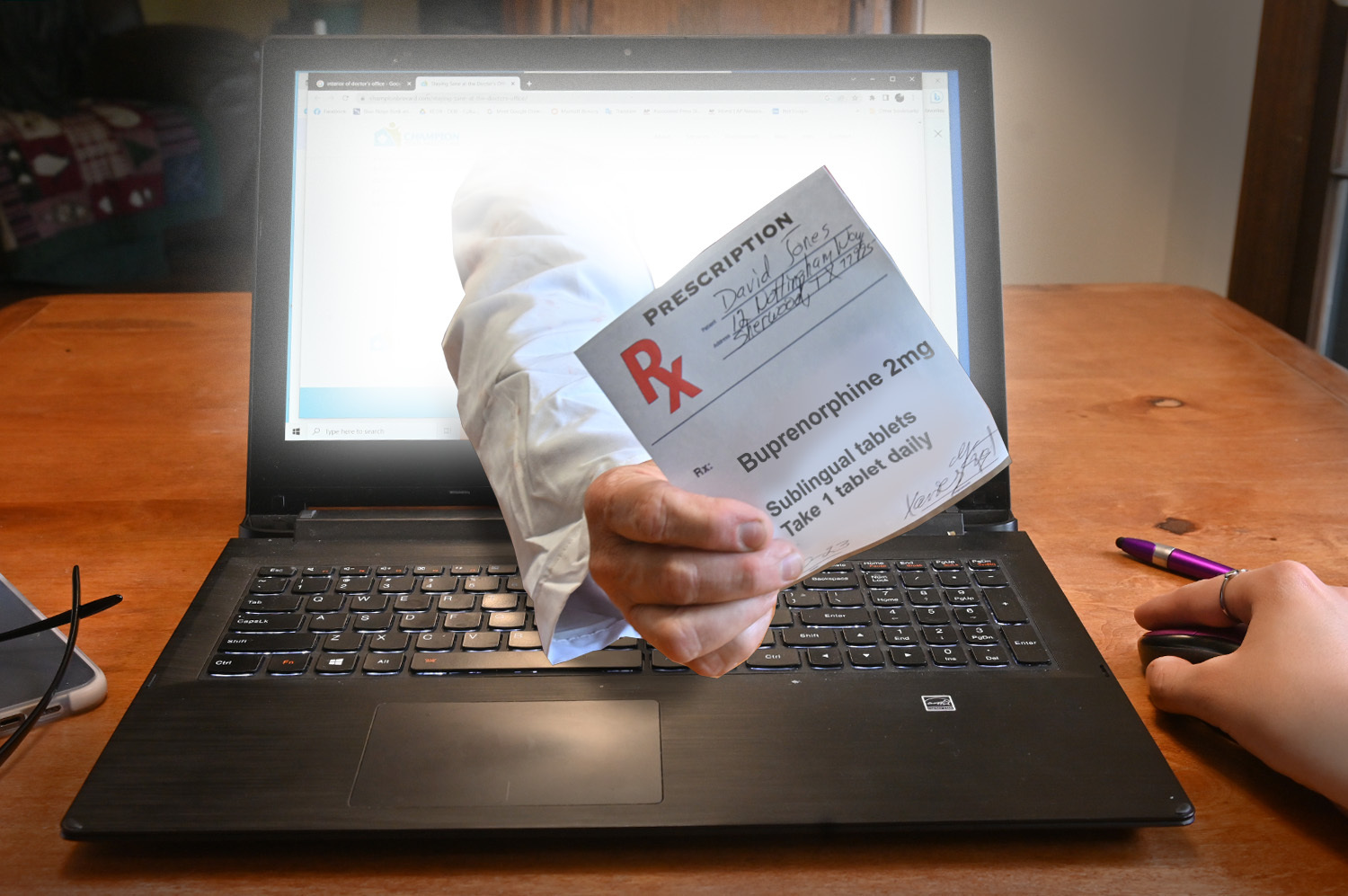
Recently published in Stat, this article outlines how the launch of telehealth platforms by pharmaceutical companies, most notably Eli Lilly’s LillyDirect, portends a gamechanger for DTC prescription marketing.
Spurred by the escalating demand for Eli Lilly’s Zepbound and Mounjaro GLP-1 drugs, LillyDirect connects consumers with a third-party telehealth provider for prescriptions, an online pharmacy for fulfillment, and in-house payment support through streamlined coupon applications and prior authorization troubleshooting. In exchange, Eli Lilly gets access to reams of patient data, in addition to boosted sales. Pharma companies insist that the platforms have proper firewalls in place, as no money directly changes hands between them and their affiliated telehealth providers.
The Gist:With so manyothercompanies hopping on the GLP-1 virtual prescription bandwagon, it’s no wonder why pharma companies are opting to enter the market directly. What LillyDirect offers is not fundamentally different than platforms like Ro or Teladoc: using telehealth to blur the lines between prescription and over-the-counter medications by empowering consumers to seek out the care they want.
However, Eli Lilly’s control of the drug supply, ability to offer coupons, relationships with pharmacy benefit managers, and inherent brand association with the drugs give it a leg up on the competition.
By replacing “talk to your doctor about” with “visit our website for”, these consumer-focused platforms perpetuate the ongoing fragmentation of care and risk tapping into the potentially harmful side of consumerization in healthcare.
On Wednesday, e-commerce giant Amazon announced that its 167M US-based Prime members can now access One Medical primary care services for $9 per month, or $99 per year, which amounts to a 50 percent annual discount on One Medical membership. (Additional Prime family members can join for $6/month or $66/year.)
One Medical, which Amazon purchased for $3.9B last year, provides its 800K members with 24/7 virtual care as well as app-based provider communication and access to expedited in-person care, though clinic visits are either billed through insurance or incur additional charges. Amazon also recently started offering virtual care services through its Amazon Clinic platform, at cash prices ranging from $30 to $95 per visit.
The Gist:After teasing this type of bundle with a Prime Day sale earlier this year, Amazon has made the long-expected move to integrate One Medical into its suite of Prime add-ons, using a similar pricing model as its $5-per-month RxPass for generic prescription medications.
At such a low price, Amazon risks flooding One Medical’s patient population with demand it may struggle to meet. But if Amazon can scale One Medical, while maintaining its quality and convenience, it may be able to make the provider organization profitable.
Known for its willingness to take risks and absorb financial losses, Amazon is continuing to build a healthcare ecosystem focused on hybrid primary care and pharmacy services that delivers a strong consumer value proposition based on convenience and low cost.
There is a local urgent care chain that we frequented regularly when my kids were young and cycling through rounds of ear infections and strep throat. The experience was always solid, driven by online scheduling, efficient operations, and good customer service.
A few years ago, the clinics were bought by a local health system. We recently visited one for the first time post-acquisition, when my now teenage son needed to rule out a broken bone from a sports injury. This experience at the same urgent care left a very different impression.
In contrast to the “easy in, easy out” experience I expected, we sat in an exam room for hours, even though the place was not crowded. While this could be due to the staffing challenges pervasive across the industry, other elements of the acquisition left a different impression.
Gone was the advertised cash pricing (and I’m anticipating a higher bill once we get one). The new patient self-registration system was overly complex, built for a hospital, not an immediate care setting.
The only signs of “systemness”? Multiple prompts to sign up for the health system’s MyChart patient portal (not interested, they have few facilities close by), and a printed referral to an employed orthopedic surgeon a forty-minute drive from home (with no guidance as to whether or when we should seek it, given that no bones were broken).
A few days ago, a scheduler from the system called to book the appointment. With no inquiry as to whether my son’s pain had improved, the interaction felt like a business transaction, not clinical follow-up. I declined.
Just because a care site is acquired by a health system, that doesn’t mean that patients will feel any value from its being part of a system.
Right or wrong, my impression was that health system ownership has made for a worse experience: inefficient, more complicated, and possibly more expensive.
Nothing about the visit gave me confidence that there was a benefit to following up with an affiliated provider. The health system had failed to earn our referral.
Systems buy assets like urgent care to create entry points that will generate downstream demand and hopefully build loyalty to the brand. But capturing that must start with delivering an excellent experience in every encounter, not merely changing the name on the building.
Politicians, economists, auto industry analysts and main street business owners are closely watching the UAW strike that began at midnight last Thursday. Healthcare should also pay attention, especially hospitals. medical groups and facility operators where workforce issues are mounting.
Auto manufacturing accounts for 3% of America’s GDP and employs 2.2 million including 923,000 in frontline production. It’s high-profile sector industry in the U.S. with its most prominent operators aka “the Big Three” operating globally. Some stats:
The US automakers sold an estimated 13.75 million new and 36.2 million used vehicles in 2022.
The total value of the US car and automobile manufacturing market is $104.1 billion in 2023:
9.2 million US vehicles were produced in 2021–a 4.5% increase from 2020 and 11.8% of the global total ranking only behind China in total vehicle production.
As of 2020, 91.5% of households report having access to at least one vehicle.
There were 290.8 million registered vehicles in the United States in 2022—21% of the global market.
Americans spend $698 billion annually on the combination of automobile loans and insurance.
By comparison, the healthcare services industry in the U.S.—those that operate facilities and services serving patients—employs 9 times more workers, is 29 times bigger ($104 Billion vs. $2.99 trillion/65% of total spend) and 6 times more integral in the overall economy (3% vs. 18.3% of GDP).
Surprisingly, average hourly wages are similar ($31.07 in auto manufacturing vs. $33.12 in healthcare per BLS) though the range is wider in healthcare since it encompasses licensed professionals to unskilled support roles. There are other similarities:
Each industry enjoys ubiquitous presence in American household’ discretionary. spending.
Each faces workforce issues focused on pay parity and job security.
Each is threatened by unwelcome competitors, disruptive technologies and shifting demand complicating growth strategies.
Each is dependent on capital to remain competitive.
And each faces heightened media scrutiny and vulnerability to misinformation/disinformation as special interests seek redress or non-traditional competitors seek advantage.
Ironically, the genesis of the UAW dispute is not about wages; it is about job security as electric-powered vehicles that require fewer parts and fewer laborers become the mainstay of the sector. CEO compensation and the corporate profits of the Big Three are talking points used by union leaders to galvanize sympathizer antipathy of “corporate greed” and unfair treatment of frontline workers.
But the real issue is uncertainty about the future: will auto workers have jobs and health benefits in their new normal?
In healthcare services sectors—hospitals, medical groups, post-acute care facilities, home-care et al—the scenario is similar: workers face an uncertain future but significantly more complicated. Corporate greed, CEO compensation and workforce discontent are popular targets in healthcare services media coverage but the prominence of not-for-profit organizations in healthcare services obfuscates direct comparisons to for-profit organizations which represents less than a third of the services economy. For example, CEO compensation in NFPs—a prominent target of worker attention—is accounted differently for CEOs in investor-owned operations in which stock ownership is not treated as income until in options are exercised or shares sold. Annual 990 filings by NFPs tell an incomplete story nonetheless fodder for misinformation.
The competitive landscape and regulatory scrutiny for healthcare services are also more complicated for healthcare services. Unlike auto manufacturing where electric vehicles are forcing incumbents to change, there’s no consensus about what the new normal in U.S. healthcare services will be nor a meaningful industry-wide effort to define it. Each sector is defining its own “future state” based on questionable assumptions about competitors, demand, affordability, workforce requirements and more. Imagine an environmental scan in automakers strategy that’s mute on Tesla, or mass transit, Zoom, pandemic lock-downs or energy costs?
While the outlook for U.S. automakers is guardedly favorable, per Moody’s and Fitch, for not-for-profit health services operators it’s “unsustainable” and “deteriorating.”
Nonetheless, the parallels between the current state of worker sentiment in the U.S. auto manufacturing and healthcare services sectors are instructive. Auto and healthcare workers want job security and higher pay, believing their company executives and boards but corporate profit above their interests and all else. And polls suggest the public’s increasingly sympathetic to worker issues and strikes like the UAW more frequent.
Ultimately, the UAW dispute with the Big Three will be settled. Ultimately, both sides will make concessions. Ultimately, the automakers will pass on their concession costs to their customers while continuing their transitions to electric vehicles.
In health services, operators are unable to pass thru concession costs due to reimbursement constraints that, along with supply chain cost inflation, wipe out earnings and heighten labor tension.
So, the immediate imperatives for healthcare services organizations seem clear as labor issues mount and economics erode:
Educate workers—all workers—is a priority. That includes industry trends and issues in sectors outside the organization’s current focus.
Define the future. In healthcare services, innovators will leverage technology and data to re-define including how health is defined, where it’s delivered and by whom. Investments in future-state scenario planning is urgently needed.
Address issues head-on: Forthrightness about issues like access, prices, executive compensation, affordability and more is essential to trustworthiness.
Stay tuned to the UAW strike and consider fresh approaches to labor issues. It’s not a matter of if, but when.
PS: I drive an electric car—my step into the auto industry future state. It took me 9 hours last Thursday to drive 275 miles to my son’s wedding because the infrastructure to support timely battery charges in route was non-existent. Ironically, after one of three self-charges for which I paid more than equivalent gas, I was prompted to “add a tip”. So, the transition to electric vehicles seems certain, but it will be bumpy and workers will be impacted.
The future state for healthcare is equally frought with inadequate charging stations aka “systemness” but it’s inevitable those issues will be settled. And worker job security and labor costs will be significantly impacted in the process.
A physician who has led the primary care enterprise for a large health system for over twenty years told us he’s never seen physician morale as low as it is now:
“Burnout is bad across the board for all specialties, but I’m having a really hard time finding the bright spots for primary care”.
We recalled a recent survey of primary care physicians that confirmed his observations, with 61 percent of doctors stating that primary care is “crumbling”. But it struck us that we’ve been seeing these kinds of dire surveys about the state of primary care for the entire quarter-century we’ve been doing this work.
What’s different now?
He posited one critical change. Ten years ago, during the heyday of accountable care, primary care was central to health system strategy. Systems were devoting resources to converting practices to patient-centered medical homes. “We felt like primary care was at the heart of transforming health systems, and that we were finally getting resources to help patients,” he shared.
“Now it feels like the health system has moved away from ‘value’, the focus is all on specialists and growing procedure volume again, and we’re being treated as a cost center and told to cut staff and up our referral targets.”
We agree. Although large independent primary care groups continue to command record valuations, overall, the transition to value has slowed, and work burden has increased given staffing shortages.
Where could optimism come from now?
We both agreed that workflow innovations to ease documentation burden and help the transition to virtual care appear closer to reality than ever before.
And the increased focus on “consumerism” has many systems recognizing that primary care is the first—and principal—touchpoint for most patients and will be key to winning consumer loyalty.
Amazon announced that it has expanded its direct-to-consumer virtual care platform to all 50 states and the District of Columbia. Amazon Clinic, which the e-commerce giant launched in 32 states last November, connects consumers to third-party clinicians via Amazon’s website or mobile app. Through video call or message-based visits (the latter of which are only available in some states), it offers diagnosis and treatment for a range of low-acuity, common health conditions like pink eye and sinus infections. The clinic features flat, upfront cash pricing, and doesn’t currently accept insurance. On the provider side, Amazon is partnering with telehealth companies Wheel, SteadyMD, Curai Health, and Hello Alpha.
The Gist: This is the kind of venture at which Amazon excels: creating a marketplace convenient for buyers and sellers (patients and telemedicine providers, respectively), pricing it competitively to pursue scale over margins, and upselling customers by pairing care with Amazon’s other products or services (like Amazon Pharmacy).
We’ll be watching for how Amazon builds on this service, and whether it connects Amazon Clinic to its Prime membership and One Medical assets. In the meantime, in addition to its consumer-focused offerings,Amazon is also simultaneously expanding its enterprise workflow offerings through its AWS for Health division, recently launching HealthScribe and HealthImaging.
This annual look at high-impact trends affecting healthcare in the coming year is based on evaluation of current industry research data. Healthcare Finance Trendsfor2023 (Trends) explores eight themes identified by CommerceHealthcare® ranging across four areas:
Financial. Providers enter the year contending with multiple financial stress points. They will also seek growth in technology-enabled remote care.
Patient financial experience. The need to drive not only improvement but also personalization of the financial experience is paramount. A central role will be played by patient financing programs which will see growing demand in 2023.
Trust. Building trust with all constituencies is explored as a linchpin for long-term provider success. The latest findings on cybersecurity show that this contributor to trust will continue to consume leadership attention.
Digital transformation. Pursuit of digital-first operations is accelerating, with the finance area an important focus. Emerging payment modes are finding a home in healthcare’s digital finance landscape.
This report’s consistent message is that these trends intersect in ways that compound both the challenges and the upside potential of strategies that address them.
1. Multiple Financial Stress Points Will Constrain Options
Healthcare’s financial predicament for the next 12–18 months is being described in strong terms. Citing $450 billion of EBITDA that could be in jeopardy, more than half of the industry’s project profit pool by 2027, one analyst suggests “a gathering storm.” Another perceives “broad and serious threats” as “elevated expenses” erode margins and exact “a profound financial toll.” Fitch Ratings issued a “deteriorating” outlook for nonprofit health systems.
These financial headwinds are upending healthcare’s traditional status as “recession-proof.” It is helpful to probe the multiple forces in play, the urgent workforce management challenge, and the varied solution set.
Multiple stress factors at work
Observing that margins will be down 37% in 2022 relative to pre-pandemic, a recent stark assessment concluded, “U.S. hospitals are likely to face billions of dollars in losses — which would result in the most difficult year for hospitals and health systems since the beginning of the pandemic.”
A confluence of factors is exacerbating the stress for 2023:
Rising acuity levels. Over two-thirds of surveyed C-suite executives said patient health has worsened from pandemic-induced delayed care. The upshot, stated by 27% of CFOs, is rising expenses due to higher acuity. Inpatient days are projected to increase at an 8% rate over the coming decade.
Reimbursement gaps and inflation. Commercial and government reimbursement rates are not keeping pace with rising costs. Surging inflation is widening this gap. Hospitals are also reporting substantial insurer payment delays and denials.
Investment declines. Stock and bond market declines have removed a cushion for operating weakness. Market uncertainty will complicate 2023 portfolio management.
Persistent workforce concerns remain center stage
Burnout and shortages have disrupted the clinical workforce. Nearly 60% of physician, advanced practice provider and nurse survey respondents said their teams are not adequately staffed, and 40% lack resources to operate at full potential. Many providers face extreme to moderate shortages of allied health professionals.
The problem extends beyond the clinical. A survey saw 48% of respondents experiencing severe labor deficiencies in revenue cycle management (RCM) and billing, and one in four finance leaders must fill over 20 positions to be fully staffed.
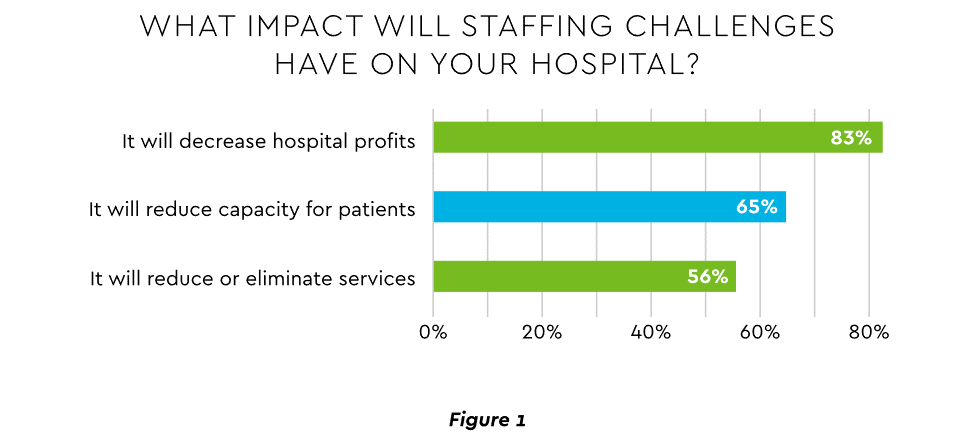
An executive outlook highlighted demonstrable impact on financial performance and growth from these workforce problems, citing reductions in profitability, capacity and service (Figure 1).1
Expenses. Hospital employee expense is expected to increase $57 billion from 2021 to 2022, with contract labor ballooning another $29 billion. Average weekly earnings are up 21.1% since early 2022. Half of medical practices budgeted higher staff cost-of-living increases in 2022. Shortages plague post-acute facilities as well. Their reduced capability to accept discharged patients is lengthening many hospitals’ patient stays.
Capacity constraint. Two-thirds of healthcare leaders identify “ability to meet demand” as their top workforce concern, suggesting a “looming capacity gap between future demand and labor supply.”
Range of measures being deployed
Health systems, hospitals and practices will vigorously pursue at least four direct actions to overcome the financial and staffing hurdles:
Cost cutting. Expense control will be paramount and “hospitals will be forced to take aggressive cost-cutting measures.” McKinsey estimates total industry administrative savings of $1 trillion through multiple aggressive changes.
Service line rationalization. Providers are rethinking how they deliver services to optimize efficiency. One path is utilizing “lower level” healthcare professionals in ways that free RNs and LPAs for more complex work suited to their top skills. Integrating remote care into the mix is another core element of the strategy.
Recruitment and retention programs. Attracting and retaining talent is crucial. Compensation is one avenue. Over two-thirds of organizations are offering signing bonuses for allied health professionals. Some are instituting value-based payments for physicians, offering salary floors to protect from drops in patient volume. CFOs and CNOs are joining forces to invest in nurse retention strategies.
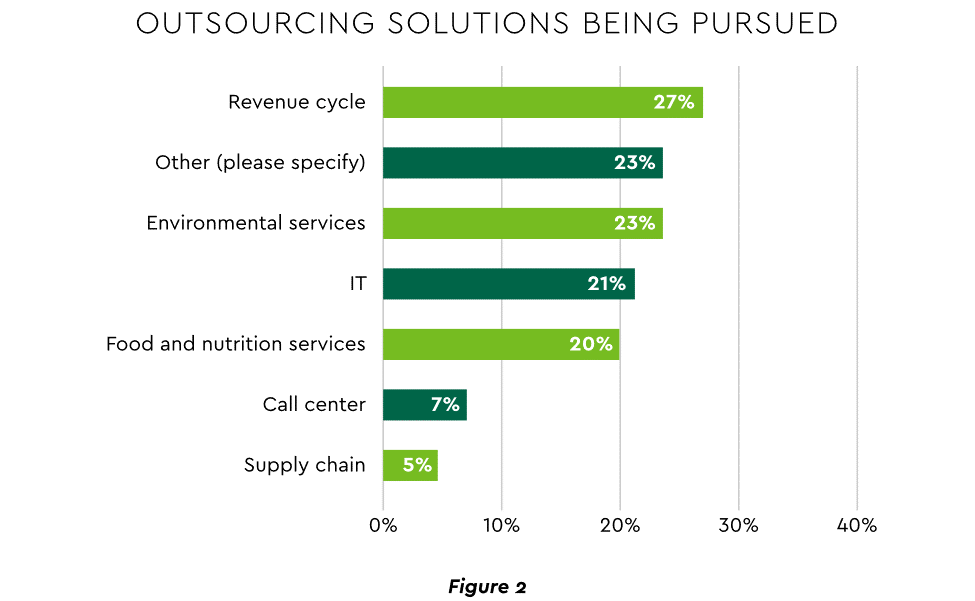
Staffing management. An increasingly popular tool to reduce labor cost and optimize staff resources is outsourcing. Figure 2 shows that RCM is leading the way among those using the solution.
2. Growth Strategies Favor Outpatient, Virtual, Acute Home Care
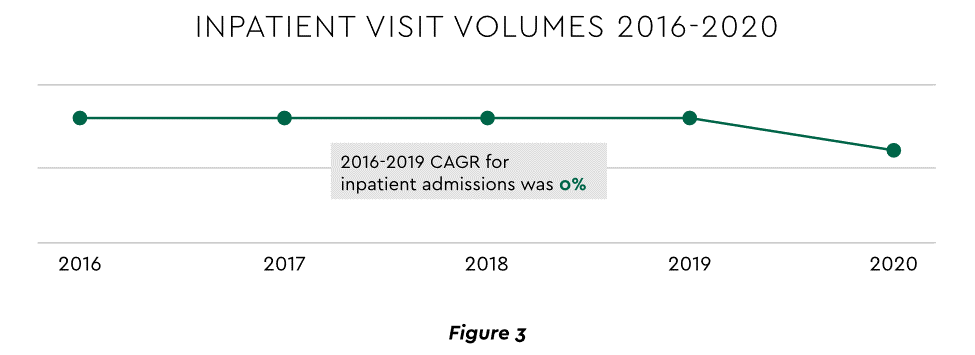
Pursuing top line growth in tandem with reining in expenses is essential. Inpatient volume growth has been tepid for several years ─ essentially flat in the 2016–20 period (Figure 3).
Leaders have been pivoting to outpatient and virtual care to diversify revenue streams. Two high-potential 2023 growth tracks in this sector merit deeper assessment.
Telehealth
Considerable evidence attests to strong commitment to telehealth and remote care. Sixty-three percent of physicians worldwide expect most consultations to be performed remotely within 10 years. Approximately 40% of health centers are using remote patient monitoring today. Consumers are also positive: 94% definitely or probably will use telehealth again, 57% prefer it for regular mental health visits and 61% use it for convenient care.
Telehealth is still in early stages of maturity. Only 4% of surveyed top executives consider their organization proficient at implementing remote care. Healthcare is also recognizing that a full telehealth ecosystem must be constructed. A physician leader explained that the industry’s early telehealth incarnations failed to build “virtual-only environments or really drive e-consults as a way of doing things.” A vital ecosystem demands alterations to current contracts, coding, collections, patient financing, staff training and other business practices.
Hospital-at-Home (HaH)
Health systems see particularly promising growth in the provision of acute care in patients’ home settings, including post-surgical and cancer treatment. The federal government has already allowed waivers to 114 systems and 256 hospitals to obtain inpatient-level reimbursement for acute care at home. However, these waivers were prompted by the pandemic and are slated to end in early 2023. The renewal uncertainty has stymied some activity and represents an overhang on the opportunity. However, enthusiasm appears strong, and 33% of hospitals in a recent poll said they would be prone to continue HaH even without renewal.
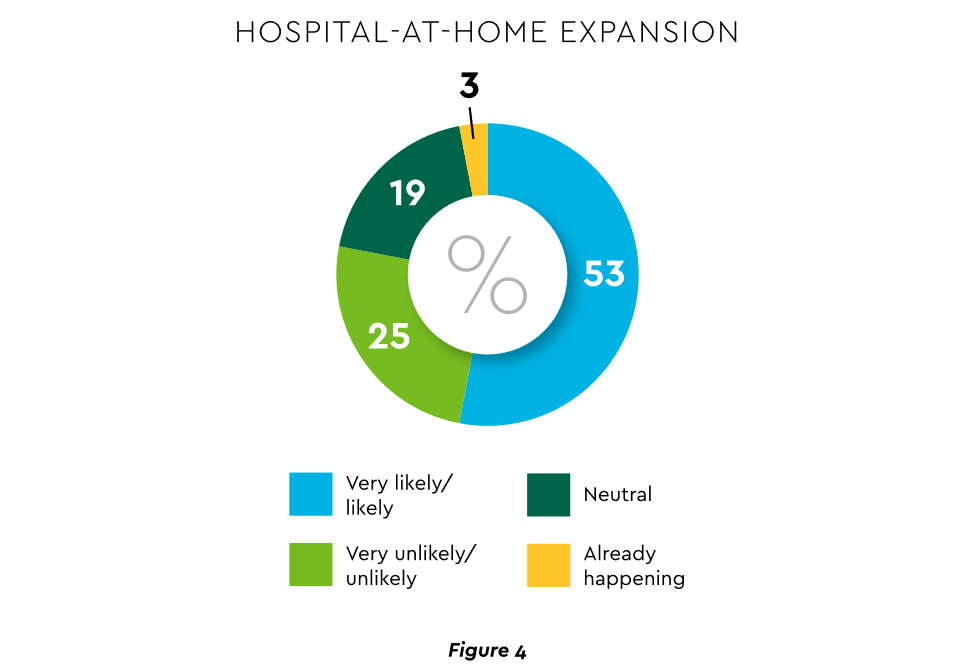
The forecasts are encouraging. Over half of hospitals believe it likely they will utilize HaH for at least half of their chronically ill patients over the next several years (Figure 4).
Harvesting the HaH potential will require implementation of current and emerging enabling technologies in remote monitoring, high-speed networks and artificial intelligence that generates algorithmic guidance for caregivers and patients alike.
3. Strong Drive to Improve and Personalize the Patient Financial Experience
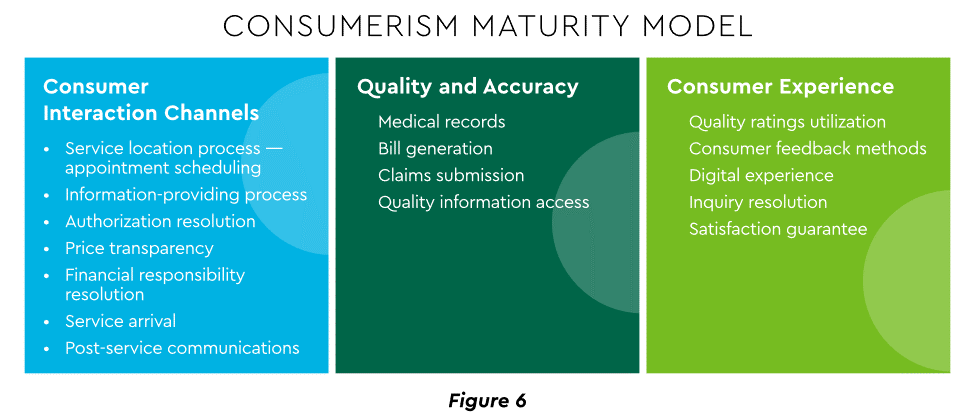
Today’s healthcare market dynamics place a premium on positive patient experiences. The goal is to deliver “an empathetic relationship between customers and brands built on what the customer wants and how they want to be treated.” It is a complex undertaking, with numerous touchpoints as captured in HFMA’s Consumerism Maturity Model (Figure 6).
An array of studies underscores the value proposition for intense provider focus on patient financial experience:
Sixty-one percent of consumers said that ease of making payments is very or somewhat important in decisions to continue seeing a doctor. Over half of patients also said text message reminders make them very or somewhat more likely to pay a bill faster than usual.
Thirty-five percent of respondents “have changed or would change healthcare providers to get a better digital patient administrative experience.”
A quality financial experience encompasses “simplified explanations, consolidated bills that match one’s health plan benefits, clear language displaying patient liability and payment options.”35
Significantly improving the financial experience requires a unified strategy, not just a collection of individual initiatives. Three threads to such a strategy will be prominent in 2023.
Using a Digital Front Door
Organizations have been moving swiftly to channel many patient financial transactions through an integrated Digital Front Door (DFD). This approach offers patients a singular online point of access and intelligent navigation to needed services. Growth is accelerating. A DFD is their patients’ first contact point for 55% of responding organizations, according to one technology survey. A leading forecaster sees 65% of patients engaging services via digital front doors by 2023.
Expanding price transparency
Mandates for full price transparency and “no surprises” billing are in effect, but estimates of compliance are mixed. An analysis of 2,000 hospitals determined that only 16% met the requirement to post an online “machine readable” file displaying clear charges for 300 “shoppable services.” Another assessment showed a more substantial 76% of hospitals had posted files, and 55% were deemed “complete.” One provision of interest to practices is the “good faith estimate” of expected charges required to be given to uninsured and self-pay individuals when they schedule visits. CommerceHealthcare® has worked with clients to enhance the patient financial experience by complementing their website pricing data with clear information on patient financing options and enrollment access. Bill pay information can also be added for one-stop guidance.
Personalizing the experience
Beyond choice and convenience, the deeper objective is truly personalized experiences throughout the care journey. The words of leading analysts best define the drive to personalize:
“Tomorrow’s healthcare experience will be built by patients tailoring their own experience.”
“By 2024, 30% of chronic care patients will truly own and openly leverage their personal health information to advocate for, secure, and realize better personalized care.”
Opportunities abound to personalize the patient financial experience. Automating manual processes establishes a foundation. Patient financing with no- or low-interest credit lines and flexible terms can produce monthly payment schedules tailored to each patient’s needs. Refunds can be made through multiple payment modes to meet varying patient preferences.
4. Evidence Underscores Growing Demand for Patient Financing
Emphasizing patient financing as part of the overall experience is powerful. Patients continue to struggle paying for care. Recent granular data details three related forces at work.
Meeting care costs difficult for many patients
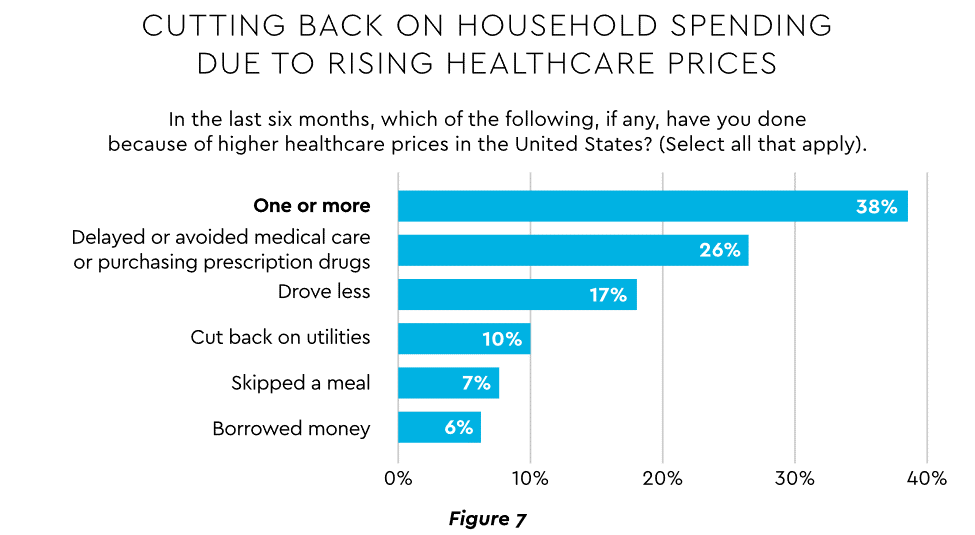
Commonwealth Fund found that 42% of individuals had problems paying medical bills or were paying off medical debt during the past year, while 49% were unable to pay an unexpected $1,000 medical bill.42 Health costs trigger reduction in a range of personal expenditures, led by deferring or avoiding care and drugs (Figure 7).
Twenty-eight percent of Americans now describe themselves as less prepared than last year to pay for routine or unanticipated care.
Patient obligation for care costs still rising
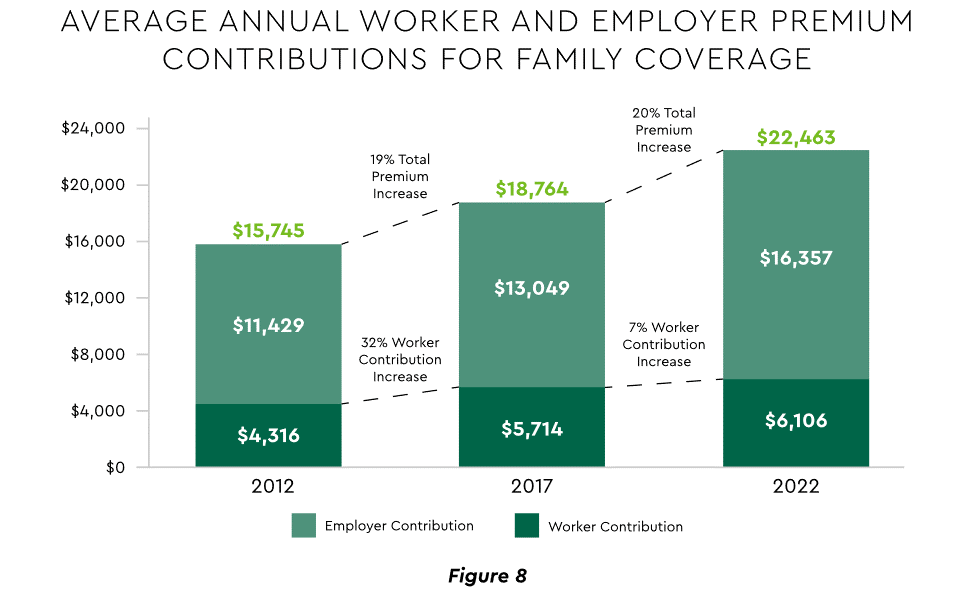
Patient obligation continues its upward march. Insurance premiums have climbed steadily for both the insured and their employers, and employees now pay over $6,000 annually on average for family coverage (Figure 8).45
High deductible health plans (HDHP) also place substantial burden on the patient. Through 2021, 28% of workers were enrolled in an HDHP with an average family deductible of $4,705. Employer satisfaction with these plans is high, auguring further expansion.
Providers feeling the financial effects
Patient payment difficulties are clearly impacting provider financials. A recent in-depth analysis uncovered substantial self-pay issues:
Self-pay accounts represented 60% of 2021 patient bad debt, up from 11% in 2018.
Nearly 18% of patient balances were over $7,500 and 17% over $14,000. Collections were noticeably lower at these balances.
Multiple chronic conditions add to the problem. A recent extensive analysis concluded: “Among individuals with medical debt in collections, the estimated amount increased with the number of chronic conditions ($784 for individuals with no conditions to $1,252 for individuals with 7–13).”
For their part, providers will be encouraged to broaden patient financing programs. Patients are certainly interested. When asked, 62% of consumers indicated they would use financing options or creative payment plans if available for large bill amounts. Many health systems, hospitals and practices will turn to outside help to satisfy the demand. A recent analysis recommended that health systems “consider keeping shorter-term payment plans in-house and extended term plans through external partnerships.”
Organizations will also need to step up their communications. A survey revealed that 64% of patients were unaware that their doctors and hospitals offered payment plans or financial help.
5. Building Trust Becoming a Critical Success Factor
Trust has emerged as a paramount issue today for most organizations as they encounter an “imperative to build trust and transparency among different stakeholder groups — employees, customers, suppliers, regulators and the communities in which they operate.” Healthcare is no exception, and the trust issue is growing in both complexity and urgency.
Healthcare’s trust gap
Trust in healthcare took a hit from the COVID-19 experience. A spring 2022 HFMA survey recorded 44% of finance leaders saying they perceived decreased patient trust. Between April 2020 and December 2021, the percentage of Americans who trusted information from doctors “a great deal” declined by 23%, from hospitals 21%, and from nurses 16%. The patient financial experience also faces “drivers of mistrust,” according to surveyed leaders who cited general payment confusion (58%), surprise billing (39%), high prices of commodity items (28%) and lack of price transparency (26%). Building trust reaps dividends. People who trust their providers are five times more likely to stay with them than those who are neutral or distrustful.
Strategies for building trust
Industry experts promote several approaches to galvanize trust among all constituencies:
Commitment. Embedding trust deeply in the organization requires full support from senior leadership.
Data transparency and governance. IDC predicts that “by end of 2023, 20% of expenses on care integration solutions will be centered around ‘trust’ to protect data, workflows and transactions.”
Reliance on fewer business partners. Many health systems, hospitals and practices are reducing their number of vendors in order to focus on a set of trusted long-term partners. For example, almost two-thirds of surveyed providers said they were seeking to streamline the number of software solutions over the next year.
The bank partner advantage
A provider’s banking relationship can yield valuable collaboration in the trust-building endeavor. Banks enjoy solid trust among consumers. As an example, 53.4% of consumers rated banks as most trusted to provide payment “super apps” and financial digital front doors ─ exceeding the next closest source by 10 points.
6. Cybersecurity in 2023: No Rest for the Weary
Cybersecurity is part of the trust calculus and has become an evergreen topic in healthcare. Compromised data and ransomware attacks are ongoing and leaders must continually refine their understanding in at least three areas: the overall security landscape, particular financially related considerations and contemporary security defenses.
The current landscape
The latest statistics quantify the cyber assault on healthcare:
Incidence. 89% of organizations suffered at least one attack in the past 12 months with the average number at 43.
Cost. A provider’s most serious attack costs an average of $4.4 million. IBM calculated healthcare’s average total cost of a breach at $10.1 million, up 42% since 2020.
Attack Characteristics. Healthcare data types most commonly compromised are personal (58%), medical (46%), and credentials (29%). Organizations have an exposure to an average of over 26,000 network-connected devices. A disturbing finding is that those healthcare institutions that paid ransom got back only 65% of their data in 2021.
Specific financial considerations
Finance leaders will also need awareness of the following:
Cyberattacks could affect credit ratings and are often a component of Environmental, Social and Governance assessments.
Financial outsourcing requires monitoring. A recent news story chronicled an accounts receivable firm’s breach that exposed individual information, account balances and payments.
Cyber insurance premiums are likely to increase substantially.
Responses/tools
Beyond a host of management and monitoring tools being deployed, a strategic philosophy is rapidly gaining ground. The “zero trust” model sounds counter to the trust-building mindset described earlier, but it has become essential. It “denies access to applications and data by default,” and 58% of hospitals and health systems have a zero trust initiative in place. Another 37% intend to implement one within 12–18 months.
Cybersecurity investment will challenge CFOs in 2023, especially in areas such as talent. Cybersecurity worker availability is estimated to satisfy only 68% of open positions. Banking partners will also be expected to play an important role. Over the years, major banks have become “leaders in enhancing cyber strategy and investing in cyber defenses, processes and talent.”
7. Digital Transformation of Finance In Focus
Digital transformation is fundamental to healthcare’s business and care delivery model changes. IBM’s website succinctly captures the goal, “Digital transformation means adopting digital-first customer, business partner, and employee experiences.” A leading forecaster believes 70% of healthcare organizations will rely on digital-first strategies by 2027.
Transformation efforts need to accelerate. One study showed that “digital, technology and analytics strategies exist for nearly all organizations, yet only 30% have begun to execute on those plans.”
One functional segment ramping up digital transformation is finance. According to a recent survey, 94% of CFOs and senior leaders stated that such efforts will be at the forefront of financial operations and strategy for 2023–2024, and 79% described it as an “absolute need” for “commercial stabilization and long-term survival of their healthcare organization.”
Advanced technology is gaining traction. Many see optimization in combining robotic process automation (RPA), artificial intelligence and machine learning to create “intelligent automation.” Together, these technologies create algorithms to automate decisions that guide “robotic” software to perform financial actions and thereby reduce manual labor.
Getting to digital-first in finance and across the enterprise has several critical success factors. These include sustained commitment, a platform-centric mindset and effective governance.
Commitment
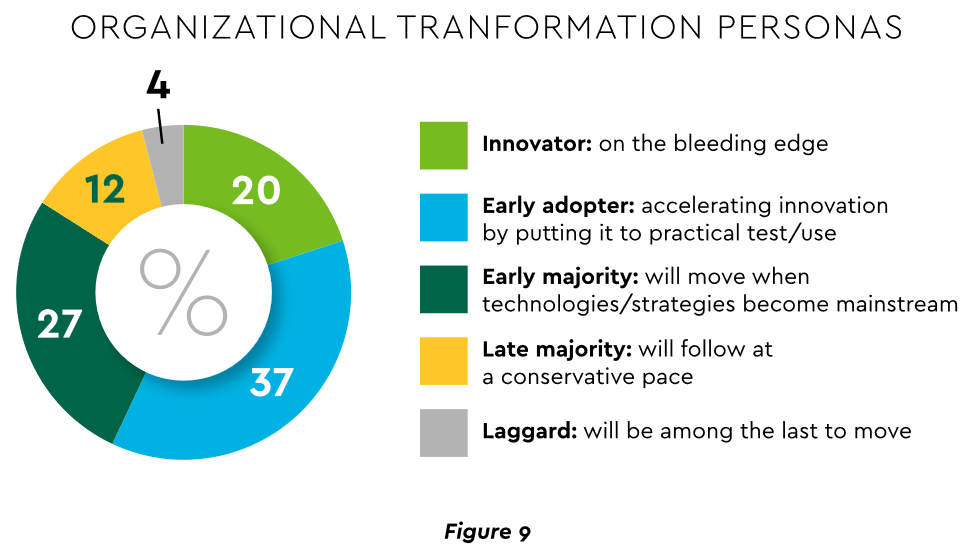
Some assert that few healthcare executives have “created digital strategies that look far enough into the future.” Speed of change is also important. Health systems, hospitals and practices exhibit varying risk appetites and change rates. When asked to self-identify “transformation personas,” a little over half regarded themselves as being on the innovative “early mover” end of the spectrum, while the remainder will adapt as technologies prove themselves (Figure 9). Slower organizations will likely need to increase the pace.
Implementing enterprise platforms rather than proliferating “point solutions” is obligatory. Organizations must be “prepared to compete in the platform economy as platform-based business models have changed the way we live, work and receive care.”
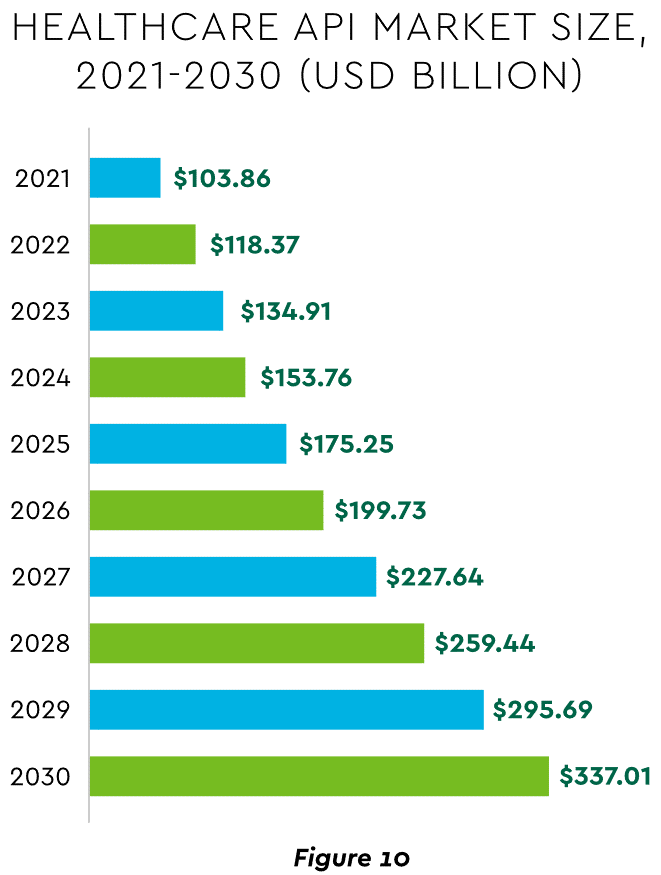
There are still too many tools and applications. A survey of top decision-makers at health systems found that 60% use over 50 software solutions just in operations (24% have over 150). System integration is one answer. Use of application programming interfaces (API) helps this effort substantially. API-first is fast becoming the norm among solution providers, with global API investment expected to nearly triple by 2030 (Figure 10)
Effective governance is vital to constructing a platform-based transformative model and to ensuring wide user adoption. Healthcare has seen the rise of new senior roles such as Chief Digital Officer and Chief Transformation Officer, positions focusing on initiatives like ownership of technology success at the department level and devising user incentives.
8. Digital Payments on the Horizon for Healthcare
A variety of emerging digital payment modes will further the transformation of finance. These payments are expected to grow almost 23% annually in healthcare. ACH payments have been on a strong upward trajectory in healthcare for several years, especially for business transactions. In 2021, ACH tallied a yearly increase of 18% in volume and 5% in dollars.
Notable technologies and payment rails to watch for expected crossover from consumer markets to healthcare include:
Mobile payments. The market for mobile payment technologies has been growing at a 16% compound annual clip and should reach $90 billion in 2023, powered by wide smartphone use, 5G networks and convenience. This category encompasses technologies such as e-wallets, forecasted to grow 23% annually worldwide through 2030.
Real-time payments (RTP). These digital transactions are settled nearly instantaneously through platforms such as The Clearing House. One forecast sees 30.4% compound RTP growth in the U.S. from 2022 to 2030.
Buy Now Pay Later (BNPL). This growing mode offers consumers short-term financing to stretch payments over several installments. A recent survey established that 23% of American adult respondents have used a BNPL service. BNPL is just entering healthcare and is currently regarded as an option for certain elective or cosmetic procedures or for specific individual credit scenarios.
Earned Wage Access (EWA). Using an RTP approach, employers are beginning to offer on-demand pay which enables “instant access to earned wages right after the work is performed, at the end of the shift, or upon completion of a project.” It is not a loan or advance pay. A 2021 poll conducted by Harris found that 83% of U.S. workers feel they should be able to access earned wages at the end of each day. Millennials were particularly interested: 80% would like daily automatic pay streaming to their bank accounts, and 78% said free EWA would boost loyalty to their employer. Given its pressing workforce concerns, healthcare is likely to find EWA a tool to promote retention.
Seeking the right use cases for these payment technologies offers many potential provider benefits.
Conclusion
The connected forces discussed and quantified here create major challenges to address in 2023. The strategic agenda calls for balancing tight cost control with investment in growth opportunities, significantly enhancing patient financial experience by meeting growing patient financial need, shoring up trusted relationships and cybersecurity, and accelerating the digital transformation of finance.
In an era of significant medical debt, rising healthcare costs and delayed treatments, our current healthcare system is ripe for solutions that alleviate the burden of paying patient bills.
Enter embedded finance. While not a new concept by any stretch – it has long existed in retail – fintechs and traditional banks are determined to give patients more options and a fundamentally better experience in the way they pay for healthcare services. In doing so, a financially strained domestic healthcare system stands to benefit from increased cash flow, improved health equity and optimized patient engagement.
Simply put, embedded finance is the integration of financial services – such as payment, lending, banking and insurance features – into another company’s normal service or products. We have all undoubtedly come across these offerings in our daily lives as consumers. Think private label credit cards with retail chains or airlines, digital wallet purchase options at the Amazon checkout, a buynow-pay-later (BNPL) plan from Affirm or Klarna, or insurance obtained from a car rental.
The goal of embedded finance:
is to improve a user’s experience by accessing financial services without leaving a brand’s platform. By layering application programming interface (API)-driven fintech or banking capabilities on top of a website or mobile app for, say, a hospital patient portal, the bundled solution allows the user to stay on one website or application to complete a financial transaction. Doing so removes friction in the experience and delivers a breadth of contextual information that a provider or payer can use to prompt further action on the patient’s medical journey.
The implications for embedded finance in healthcare are vast and benefit every stakeholder across the revenue cycle value chain:
Patients: Flexibility and convenience to better structure and plan bill payment while receiving greater access to financial options and additional services that improve the care experience such as reminders and health tracking
Providers: Faster and higher rates of collections coupled with ongoing patient dialogue that cements loyalty, affords clinicians the opportunity to suggest customized treatment options, and improves revenue composition and potential valuation
Payers: More efficient claims processing cycle, automated processes and improved data security
The burden of patient bills and increasing medical costs are not new to our system. Yet there has been a confluence of fundamental changes that make embedded finance particularly attractive in healthcare going forward, including increased smartphone usage and Internet penetration, COVID19 adoption of fintech products across healthcare settings, rising inflation rates that reduce a patient’s ability to pay and the adoption of mobile-based apps among younger, digitally native consumers and lower income patients.
These tailwinds support a massive addressable market as healthcare is expected to comprise approximately 23% of a U.S. embedded finance industry set to exceed $230 billion by 2025, or a 10x increase from $23 billion in 2020.
Significant attention and capital investment are accelerating the rise of embedded finance in healthcare.
Punctuated by attractive elements at the intersection of technology, financial services and healthcare sectors, nimble fintech companies and large financial institutions alike are competing for market presence. For example, pioneering healthcare-focused fintech PayZen closed $220 million in fresh capital in late 20223, while banks such as Wells Fargo and Synchrony have launched the popular medical-focused credit cards Health Advantage and CareCredit, respectively. Cain Brothers’ parent company, KeyBank, has also advanced an embedded strategy to provide healthcare digital innovation at scale and enhance patient experiences by acquiring XUP Payments in 2021. The resulting U.S. landscape for healthcare embedded finance is one that is evolving rapidly and that we are monitoring closely for investment and eventual M&A consolidation.
With expanding options around the type of medical care received and where it is received, we expect the financial tools at a patient’s disposal to garner significant attention in the years to come.
Embedded finance is a leading solution positioned to improve health equity and the financial well-being of millions of patients across the U.S., as well as fuel sector growth. Just as we’re accustomed now to buying pretty much anything with a few clicks, so too will embedded finance become a ubiquitous part of the healthcare landscape.