Across the hospital industry, heavy reliance on contract labor in 2021 and 2022 caused a significant challenge for profitability.
However, a chief financial officer recently posited that his system’s large contract labor load has had unexpected benefits.
“Other hospitals [in our market] thought we were crazy to keep staffing with high contract rates until recently,” he shared. “But by keeping the agency nurses around a little longer, we were able to avert raising base salaries quite as much, and are in a better place today now that the labor market has softened.” It’s a story we’ve heard several times now.
While market rates for nursing and other clinical labor have undoubtedly been rebased, salary increases are sticky—it’s hard to adjust wages downward when the labor market loosens.
Systems who were able to avert large wage increases by increasing bonuses and other non-salary benefits, or forestalled permanent hiring at higher salaries by extending contract labor, now find themselves with more flexibility and potentially lower staffing costs in the long-term.
Many hospitals and health systems aim to recruit and retain permanent staff to replace contract labor positions, which have seen wages skyrocket because of staff shortages during the COVID-19 pandemic.
Hospitals across the country have relied on contract labor and temporary staffing agencies to support their clinical teams when many burned-out providers are exiting healthcare. An October survey conducted by Bain & Company found that 25 percent of physicians, advanced practice providers and nurses are considering changing careers. Eight-nine percent of the providers thinking about leaving the profession cited burnout as the driving force.
Staffing shortages are driving labor costs to an unsustainable level for hospitals operating on razor-thin margins and reducing temporary staffing costs is top of the agenda for many financial executives looking to reduce expenses in the coming quarters.
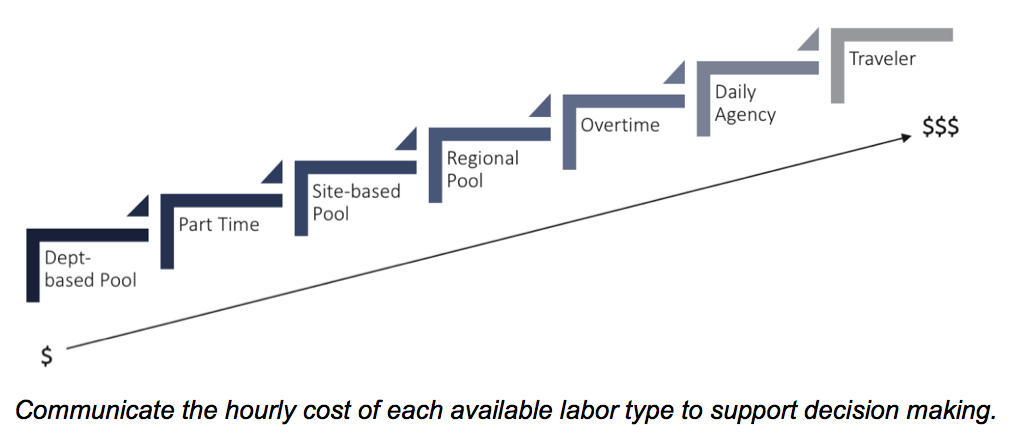
Here are 22 numbers that demonstrate the cost of contact labor for hospitals, according to reports from Kaufman Hall, Definitive Healthcare, Vaya Workforce and big hospital operators:
1. The demand for contract labor increased500 percent in fall 2021 compared with 2019, according to healthcare staffing services company Vaya Workforce. While demand has since decreased, it is still nearly triple pre-pandemic levels and is projected to remain as high as 20 percent above the 2019 baseline.
2. In 2020, the average amount hospitals spent on contract labor was $4.6 million, more than double the average expense of $2.2 million in 2011, according to a report from Definitive Healthcare, a data and analytics company.
3. Rochester, Minn.-based Mayo Clinic Hospital, Saint Mary’s Campus spent $286.8 million on contract labor in 2020, the most of any hospital in the country that year, according to Definitive Healthcare’s analysis of about 3,100 U.S. hospitals
4. From 2019 to 2022, the hourly wage rate for contract nurses increased106 percent, according to Kaufman Hall. Contract nurses are earning an average of $132an hour in 2022 versus $64an hour in 2019. At the height of the pandemic, some travel nurses earned up to $300 an hour, with rates as high as these placing immense pressure on hospital balance sheets.
5. The rise in contract labor from 2019 through March of 2022 led to a 37 percent increase in labor expenses per patient, equating to between $4,009 and $5,494 per adjusted discharge.
6. Hospitals with 25 beds or fewer spent about $460,000 on contract labor in 2020 compared to hospitals with more than 250 beds that spent almost $11 million on average, according to Definitive Healthcare.
7. Hospitals in the western U.S. have the highest contract labor expenses, with an average of $9.6 million reported in 2020. Large cities, high cost of living and high salary rates in the region contribute to this high average.
8. Labor costs were one of the core reasons Franklin, Tenn.-based Community Health Systems reported a net loss of $42 million in the third quarter, but CFO Kevin Hammons said he expects to see a 40 percent to 50 percent reduction in contract labor costs next year compared with 2022.
9. Nashville, Tenn.-based HCA Healthcare reported a 19 percent decrease in contract labor costs in the third quarter compared to the second quarter, allowing the system to absorb much of the market-based wage adjustment costs for its employee workforce, CFO Bill Rutherford said during an Oct. 21 earnings call.
10. According to Kaufman Hall’s “2022 State of Healthcare Performance Improvement” report, published Oct. 18, 46 percent of hospital and health system leaders identify labor costs as the greatest opportunity for cost reductions. This was significantly up from the 17 percent of respondents who noted labor costs as their greatest opportunity to cut costs last year.
11. There are some hopeful signs that the use of contract labor has stabilized and is steadily falling, according to Kaufman Hall: 44 percent of hospitals in its survey reported that their utilization of contract labor is declining while 29 percent said that it is holding steady.
Early into flu season, nationwide flu activity is ten times higher than at the same point last year. Meanwhile, cases of respiratory syncytial virus (RSV), a virus most severe in young children and the elderly, have tripled in the past two months, with some children’s hospitals reporting “unprecedented” admissions for the virus. And most experts expect at least some winter COVID surge, possibly involving several different variants. The combined threat of these viruses circulating together has been labeled a potential “tripledemic.”
The Gist: Across the past two winters, the widespread adoption of COVID prevention measures, including masking and social distancing, kept the spread of other viruses at bay. But with return to normal life for most Americans, other viruses have returned to circulation—and with a vengeance, as population immunity toward flu and RSV has weakened.
While it’s hard to predict when and where local surges will occur, hospitals struggling with staffing shortages may be forced to hire more contract labor to care for an influx of patients—making this a potentially challenging winter for already stretched facilities.
Working as a travel nurse in the early days of the Covid pandemic was emotionally exhausting for Reese Brown — she was forced to leave her young daughter with her family as she moved from one gig to the next, and she watched too many of her intensive care patients die.
“It was a lot of loneliness,” Brown, 30, said. “I’m a single mom, I just wanted to have my daughter, her hugs, and see her face and not just through FaceTime.”
But the money was too good to say no. In July 2020, she had started earning $5,000 or more a week, almost triple her pre-pandemic pay. That was the year the money was so enticing that thousands of hospital staffers quit their jobs and hit the road as travel nurses as the pandemic raged.
Two years later, the gold rush is over. Brown is home in Louisiana with her daughter and turning down work. The highest paid travel gigs she’s offered are $2,200 weekly, a rate that would have thrilled her pre-pandemic. But after two “traumatic” years of tending to Covid patients, she said, it doesn’t feel worth it.
“I think it’s disgusting because we went from being praised to literally, two years later, our rates dropped,” she said. “People are still sick, and people are still dying.”
The drop in pay doesn’t mean, however, that travel nurses are going to head back to staff jobs. The short-lived travel nurse boom was a temporary fix for a long-term decline in the profession that predates the pandemic. According to a report from McKinsey & Co., the United States may see a shortage of up to 450,000 registered nurses within three years barring aggressive action by health care providers and the government to recruit new people. Nurses are quitting, and hospitals are struggling to field enough staff to cover shifts.
Nine nurses around the country, including Brown, told NBC News they are considering alternate career paths, studying for advanced degrees or exiting the profession altogether.
“We’re burned out, tired nurses working for $2,200 a week,” Brown said. People are leaving the field, she said, “because there’s no point in staying in nursing if we’re expendable.”
$124.96 an hour
Travel nursing seems to have started as a profession, industry experts say, in the late 1970s in New Orleans, where hospitals needed to add temporary staff to care for sick tourists during Mardi Gras. In the 1980s and the 1990s, travel nurses were often covering for staff nurses who were on maternity leave, meaning that 13-week contracts become common.
By 2000, over a hundred agencies provided travel contracts, a number that quadrupled by the end of the decade. It had become a lucrative business for the agencies, given the generous commissions that hospitals pay them. A fee of 40 percent on top of the nurse’s contracted salary is not unheard of, according to a spokesperson for the American Health Care Association, which represents long-term care providers.
Just before the pandemic, in January 2020, there were about 50,000 travel nurses in the U.S., or about 1.5 percent of the nation’s registered nurses, according to Timothy Landhuis, vice president of research at Staffing Industry Analysts, an industry research firm. That pool doubled in size to at least 100,000 as Covid spread, and he says the actual number at the peak of the pandemic may have far exceeded that estimate.
By 2021, travel nurses were earning an average of $124.96 an hour, according to the research firm — three times the hourly rate of staff nurses, according to federal statistics.
That year, according to the 2022 National Health Care Retention & RN Staffing Report from Nursing Solutions Inc., a nurse recruiting firm, the travel pay available to registered nurses contributed to 2.47% of them leaving hospital staff jobs.
But then, as the rate of deaths and hospitalizations from Covid waned, the demand for travel nurses fell hard, according to industry statistics, as did the pay.
Demand dropped 42 percent from January to July this year, according to Aya Healthcare, one of the largest staffing firms in the country.
That doesn’t mean the travel nurses are going back to staff jobs.
Brown said she’s now thinking about leaving the nursing field altogether and has started her own business. Natalie Smith of Michigan, who became a travel nurse during the pandemic, says she intends to pursue an advanced degree in nursing but possibly outside of bedside nursing.
Pamela Esmond of northern Illinois, who also became a travel nurse during the pandemic, said she’ll keep working as a travel nurse, but only because she needs the money to retire by 65. She’s now 59.
“The reality is they don’t pay staff nurses enough, and if they would pay staff nurses enough, we wouldn’t have this problem,” she said. “I would love to go back to staff nursing, but on my staff job, I would never be able to retire.”
The coronavirus exacerbated issues that were already driving health care workers out of their professions, Landhuis said. “A nursing shortage was on the horizon before the pandemic,” he said.
According to this year’s Nursing Solutions staffing report, nurses are exiting the bedside at “an alarming rate” because of rising patient ratios, and their own fatigue and burnout. The average hospital has turned over 100.5% of its workforce in the past five years, according to the report, and the annual turnover rate has now hit 25.9%, exceeding every previous survey.
There are now more than 203,000 open registered nurse positions nationwide, more than twice the number just before the pandemic in January 2020, according to Aya Healthcare.
An obvious short-term solution would be to keep using travel nurses. Even with salaries falling, however, the cost of hiring them is punishing.
LaNelle Weems, executive director of Mississippi Hospital Association’s Center for Quality and Workforce, said hospitals can’t keep spending like they did during the peak of the pandemic.
“Hospitals cannot sustain paying these exorbitant labor costs,” Weems said. “One nuance that I want to make sure you understand is that what a travel agency charges the hospitals is not what is paid to the nurse.”
Ultimately, it’s the patients who will suffer from the shortage of nurses, whether they are staff or gig workers.
“Each patient added to a hospital nurse’s workload is associated with a 7%-12% increase in hospital mortality,” said Linda Aiken, founding director of the University of Pennsylvania’s Center for Health Outcomes and Policy Research.
Nurses across the country told NBC News that they chose the profession because they cared about patient safety and wanted to be at the bedside in the first line of care.
“People say it’s burnout but it’s not,” Esmond said about why nurses are quitting. “It’s the moral injury of watching patients not being taken care of on a day-to-day basis. You just can’t take it anymore.”
Hospitals’ reliance on travel workers is nothing new. The pandemic intensified it and highlighted the gap between full-time workers’ pay and lucrative temporary contracts.
While the average salary for a travel nurse can vary based on location, regional demand, hospital type and specialty, the compensation for a travel nurse has increased significantly compared to pre-pandemic, Bill Morgan, president of the Orlando, Fla.-based travel nurse staffing firm Jackson Nurse Professionals, toldBecker’s in September.
Meanwhile, hospitals and health systems have offered bonuses, increased wages and made other investments in employee retention for their staff workers. Still, the compensation gap between hospital employed nurses and travel or agency nurses remains stark.
The gap poses the seemingly simple question: Why aren’t hospitals paying full-time staff more instead of paying higher prices for travel workers?
Travel nursing’s start
Taking a look back at the history of why hospitals started using travel nurses in the first place helps answer that question, said Kathy Sanford, DBA, RN, chief nursing officer at Chicago-based CommonSpirit Health.
Dr. Sanford recalls first using local agencies and travel nurses in the 1980s as a cost-effective staffing strategy for periods when the patient census fluctuates, such as during flu epidemics.
“When you have those fluctuations, you need to have a staffing strategy of what you want to do when the census goes up higher than we are staffed for, but it’s only going to last maybe a month, or a little longer,” she told Becker’s. “Because of the fluctuations, our nursing strategy for staffing was to use these non-employed nurses to fill in when there were gaps.”
The COVID-19 pandemic, however, has created a situation where volumes are consistently higher than normal. And while rates for a travel or agency nurse have traditionally been higher than those of a hospital staff nurse, the current demand has pushed travel rates to record highs.
Rising rates
Pittsburgh-based UPMC, for example, paid an estimated $85 an hour for a traveling nurse or a nurse from an agency before the pandemic. The health system is now experiencing rates between $225 and $250 an hour. Such rates have made nurses who may not have considered traveling before take the leap.
“And the nurses are making more, and we don’t fault the nurses for taking advantage of that opportunity. But … now not only are nurses making more, but the agencies have taken the opportunity to triple their profits … and it shouldn’t be permitted during a pandemic, just like we don’t permit building companies to triple the price of lumber after a hurricane. It just shouldn’t be allowed,” said John Galley, chief human resource officer at UPMC.
“Hospitals are all trying to fill the positions that need to be filled to help us get through this crisis with travel nurses, but because there aren’t enough, it becomes a cycle of bidding of who will pay me the most to travel,” Dr. Sanford said. Because of that, many nurses who may have never considered traveling before are now choosing to do so and leaving hospitals in areas of the country with a lower wage index, she said.
Pay for travel nurses has always been higher for the same reasons hospitals pay float pool nurses more, Dr. Sanford explained.
“Nurses are specialists and they work on a particular type of unit, and sometimes one unit’s census will be down and another unit’s census will be up,” she said. Float pool nurses are willing to shift to different units that need help “and it’s not a favorite thing for nurses to do,” Dr. Sanford said. “You have to pay them a little extra to be willing to learn different types of nursing and be willing to float.”
The same line of thinking applies to agency or travel nurses. Travelers don’t have the perks that come with a full-time job, like job security and benefits. That coupled with the burden of travel itself and short-term assignments was the initial justification for why travel nurses had higher rates.
Simply put, hospitals can’t afford to pay full-time staff wages that were meant for temporary assignments.
“The bottom line is it would not be sustainable for hospitals to pay the kind of dollars that they’re paying right now for travel nurses in the long run. Because nurses are our backbone … they’re our heart, but they’re also our backbone. They’re the majority of our staff.” Dr. Sanford said.
Mr. Galley of UPMC echoed that sentiment, noting that salaries and benefits make up about 50 percent of a health system’s entire expenses. “If you were to double a good portion of that — the nursing salaries — you’d completely wipe out any operating margin. Then you wouldn’t be able to invest in anything to keep the hospitals going,” he said.
And healthcare has a lot of costly demands that would go unaddressed if such rates became the expectation for staff nurses.
“There are a lot of needs that healthcare has in technology, and making sure that we have the equipment to take care of patients, and that we can do programs for the poor and vulnerable that we wouldn’t be able to afford if we pay these non-sustainable prices forever,” Dr. Sanford of CommonSpirit said.
The value of in-house agencies
To combat skyrocketing travel nursing costs, some health systems have introduced their own travel agencies, including CommonSpirit and UPMC, where travel nurses work within the system.
Mr. Galley said UPMC started the agency for its 40-hospital system not only to combat the nursing shortage — and attract back nurses the health system has lost to outside travel agencies — but also to address increased rates from outside travel agencies.
Nurses and surgical techs who qualify for UPMC’s in-house agency will earn $85 an hour and $63 an hour, respectively, in addition to a $2,880 stipend at the beginning of each six-week assignment.
Compensation for travel nurses at UPMC is still higher than full-time employees because the job comes with its own set of challenges. While full-time nurses get to know their facilities and have a more regular schedule, travel nurses are constantly on the move.
“They’re going to have assignments for a few weeks at a time at a particular location, then we’re going to pick them up and move them somewhere else, so they’re going to be constantly traveling, living out of a suitcase, and that’s what external travelers do, so we want to be just like the market, create roles like that and pay like that,” Mr. Galley said. “I think our employees understand the difference between that kind of a lifestyle that goes along with the higher salary.”
CommonSpirit’s internal agency plans to start traveling in the early spring and is in the process of hiring a national director for the program. The system’s goal is to have 500 nurses.
Dr. Sanford said the program will be beneficial because it will bring down competition, and people who want to travel can still be employees within the health system.
“It gives nurses who are our employees a choice if they want to be travelers or if they want to do it part time and then come back to a job within one of our hospitals or in one of our clinics. … They won’t lose their benefits, they won’t lose their seniority. They’ll be our employees,” Dr. Sanford said.
Other systems are exploring similar programs, such as Charlotte, N.C.-based Atrium Health, which recently ran a pilot in-house traveler program. The health system has also used outside agencies, which cost about triple compared to pre-pandemic.
“This program was very successful, less expensive than using an external travel agency and worked really well across our large health system that covers multiple states,” said Patricia Mook, MSN, RN, vice president of nursing operations at Atrium Health.
But internal travel programs may not be easy for other health systems to mimic, especially smaller ones. Hospitals have to be of a certain size for an internal travel program to work, meaning an individual hospital wouldn’t be able to have one, Mr. Galley said.
More than that, it’s a complex undertaking, he said.
“It’s not without its challenges,” Mr. Galley said. “I just think it’s something that takes the resources and thought leadership to be able to do. But you’re not going to find independent hospitals being able to mirror this.”
Dr. Sanford also recommends having a few different strategies in place to combat nurse shortages.
“Don’t make it your only strategy because there are so many issues that we could do better with our nursing staff. … You need to be looking at all of the different things that give nurses voice in your organization,” Dr. Sanford said.
The American Hospital Association (AHA) is asking Congress for an additional $25B to help hospitals offset high labor costs, largely incurred by the need to rely on travel nurse staffing firms that charge two to three times pre-pandemic rates. The AHA, along with 200 members of Congress, is urging the Federal Trade Commission to investigate the staffing agencies for anti-competitive activity, although the agency has previously declined to do so.
The Gist: The Department of Health and Human Services (HHS) is now releasing$2B in of provider relief dollars from the CARES Act. Beyond that, after nearly two years and $178B of federal support, hospitals shouldn’t count on additional funds from the government, even as costs of labor and supplies continue to rise.
Instead, we’d expect more scrutinyover how the remaining relief dollars are spent. Federal support during the pandemic has masked structural economic flaws in provider economics, and we expect 2022 will be a year of financial reckoning for many hospitals and health systems.
Labor shortages from the COVID-19 pandemic will continue to worsen the financial performance of nonprofit and for-profit hospitals into 2022, an October Moody’s quarterly report found.
As nurses and other workers deal with burnout and resign from positions, some hospitals are limiting elective procedures, which is reducing revenue. They’re also increasing minimum wage and using contract nurses with much higher hourly wages.
Physician staffing companies like Envision Healthcare Corp. and TeamHealth will also struggle with profitability as it becomes more difficult to fill open positions because of fewer available physicians, the report said.
An Association of American Medical Colleges study in 2020 found that more than 2 out of 5 physicians will be 65 or older by 2030; COVID-19 is accelerating retirement.
Meanwhile, health insurers are not as affected by labor shortages, wage pressure and inflation, according to the report. Because their product is more short-term and premiums reset every year, they have more flexibility when it comes to inflation.
Clinical labor costs are up by an average of 8% per patient day, translating to $17 million in additional annual labor expenses.
As the delta variant pushes COVID-19 caseloads to all-time highs, hospitals and health systems across the country are paying $24 billion more per year for qualified clinical labor than they did pre-pandemic, according to a new PINC AI analysis from Premier.
Clinical labor costs are up by an average of 8% per patient day when compared to a pre-pandemic baseline period in 2019. For the average 500-bed facility, this translates to $17 million in additional annual labor expenses since the beginning of the public health emergency.
The data also shows that overtime hours are up 52% as of September. At the same time, the use of agency and temporary labor is up 132% for full-time and 131% for part-time workers. The use of contingency labor – positions created to complete a temporary project or work function – is up nearly 126%.
Overtime and the use of agency staff are the most expensive labor choices for hospitals – usually adding 50% or more to a typical employee’s hourly rate, Premier found.
And hospital workers aren’t just putting in more hours – they’re also working harder. The analysis shows that productivity, measured in worked hours per unit of departmental volume, increased by an average of 7% to 14% year-over-year across the intensive care, nursing and emergency department units, highlighting the significance of the increases in cost-per-hour.
Another complicating factor is that hospital employees are more exposed to COVID-19 than many other workers, with quarantines and recoveries requiring the use of sick time. The data shows that use of sick time, particularly among full-time employees (FTEs) in the intensive care unit, is up 50% for full-time clinical staff and more than 60% for part-time employees when compared with the pre-pandemic baseline.
WHAT’S THE IMPACT
The combined stressors of working more hours while under the constant threat of coronavirus exposure are pushing many hospital workers to the breaking point. In fact, the data shows clinical staff turnover is reaching record highs in key departments like emergency, ICU and nursing.
Since the start of the pandemic, the annual rate of turnover across these departments has increased from 18% to 30%. This means nearly one-third of all employees in these departments are now turning over each year, which is almost double the rate from two years ago.
This is a number that could increase as new vaccination mandates take effect. Already, one Midwestern system reported a loss of 125 employees who chose not to be vaccinated, while a New York facility reported another 90 resignations. Overall, staffing agencies are predicting up to a 5% resignation rate once vaccine mandates kick in.
While a minority of the overall workforce, losses of even a few employees during times of extreme stress can have a ripple effect on hospital operations and costs.
THE LARGER TREND
According to the American Hospital Association, hospitals nationwide will lose an estimated $54 billion in net income over the course of the year, even taking into account the $176 billion in federal CARES Act funding from last year. Added staffing costs were not addressed as part of CARES and are further eating into hospital finances.
As a result, some are now predicting that more than half of all hospitals will have negative margins by the end of 2021 – a trend that could be dire for some community hospitals.
Prior to the pandemic, about one quarter of hospitals had negative margins, the Kaufman Hall data showed. At the beginning of 2021, after almost a year of COVID-19, half of hospitals had negative margins.
Meanwhile, the most potentially disruptive forces facing hospitals and health systems in the next three years are provider burnout, disengagement and the resulting shortages among healthcare professionals, according to a March survey of 551 healthcare executives.