In a rare show of bipartisanship for the mostly polarized 115th Congress, Republican and Democratic Senate leaders announced a two-year budget deal that would increase federal spending for defense as well as key domestic priorities, including many health programs.
Not in the deal, for which the path to the president’s desk remains unclear, is any bipartisan legislation aimed at shoring up the Affordable Care Act’s individual health insurance marketplaces. Senate Majority Leader Mitch McConnell (R-Ky.) promised Sen. Susan Collins (R-Maine) a vote on health legislation in exchange for her vote for the GOP tax bill in December. So far, that vote has not materialized.
The deal does appear to include almost every other health priority Democrats have been pushing the past several months, including two years of renewed funding for community health centers and a series of other health programs Congress failed to provide for before they technically expired last year.
“I believe we have reached a budget deal that neither side loves but both sides can be proud of,” said Senate Minority Leader Chuck Schumer (D-N.Y.) on the Senate floor. “That’s compromise. That’s governing.”
Said McConnell, “This bill represents a significant bipartisan step forward.”
Senate leaders are still negotiating last details of the accord, including the size of a cut to the ACA’s Prevention and Public Health Fund, which would help offset the costs of this legislation.
According to documents circulating on Capitol Hill, the deal includes $6 billion in funding for treatment of mental health issues and opioid addiction, $2 billion in extra funding for the National Institutes of Health, and an additional four-year extension of the Children’s Health Insurance Program (CHIP), which builds on the six years approved by Congress last month.
In the Medicare program, the deal would accelerate the closing of the “doughnut hole” in Medicare drug coverage that requires seniors to pay thousands of dollars out-of-pocket before catastrophic coverage kicks in. It would also repeal the controversial Medicare Independent Payment Advisory Board (IPAB), which is charged with holding down Medicare spending for the federal government if it exceeds a certain level. Members have never been appointed to the board, however, and its use has not so far been triggered by Medicare spending. Both the closure of the doughnut hole and creation of the IPAB were part of the ACA.
The agreement would also fund a host of more limited health programs — some of which are known as “extenders” because they often ride along with other, larger health or spending bills.
Those programs include more than $7 billion in funding for the nation’s federally funded community health centers. The clinics serve 27 million low-income people and saw their funding lapse last fall — a delay advocates said had already complicated budgeting and staffing decisions for many clinics.
And in a victory for the physical therapy industry and patient advocates, the accord would permanently repeal a limit on Medicare’s coverage of physical therapy, speech-language pathology and outpatient treatment. Previously, the program capped coverage after $2,010 worth of occupational therapy and another $2,010 for speech-language therapy and physical therapy combined. But Congress had long taken action to delay those caps or provide exemptions — meaning they had never actually taken effect.
According to an analysis by the nonpartisan Congressional Budget Office, permanently repealing the caps would cost about $6.47 billion over the next decade.
Lawmakers would also forestall cuts mandated by the ACA to reduce the payments made to so-called Disproportionate Share Hospitals, which serve high rates of low-income patients. Those cuts have been delayed continuously since the law’s 2010 passage.
Limited programs are also affected. The deal would fund for five years the Maternal, Infant and Early Childhood Home Visiting Program, a program that helps guide low-income, at-risk mothers in parenting. It served about 160,000 families in fiscal year 2016.
“We are relieved that there is a deal for a 5-year reauthorization of MIECHV,” said Lori Freeman, CEO of advocacy group the Association of Maternal & Child Health Programs, in an emailed statement. “States, home visitors and families have been in limbo for the past several months, and this news will bring the stability they need to continue this successful program.”
And the budget deal funds programs that encourage doctors to practice in medically underserved areas, providing just under $500 million over the next two years for the National Health Service Corps and another $363 million over two years to the Teaching Health Center Graduate Medical Education program, which places medical residents in Community Health Centers.
Republican and Democrat Senate leaders unveiled a two-year budget deal Wednesday that would boost federal spending for several health programs.
Here are five things to know about the budget agreement.
1. The budget deal includes an additional four-year extension of the Children’s Health Insurance Program. That extension is on top of the six years of CHIP funding Congress approved in late January.
2. The plan includes more than $7 billion in funding over two years for the nation’s community health centers. Federal funding for community health centers, which serve more than 27 million people, expired Sept. 30.
3. The spending deal would delay payment cuts to Disproportionate Share Hospitals mandated by the ACA, which have been pushed back since 2010, according to Kaiser Health News.
4. The budget deal includes $2 billion in additional funding for the National Institutes of Health and $495 million for the National Health Service Corps.
5. The budget deal would repeal the ACA’s Independent Payment Advisory Board, which was intended to hold down Medicare payments if the program’s spending exceeded a certain threshold. Members have never been appointed to the IPAB, according to Kaiser Health News.
California is the most diverse place on earth. You see that diversity in our people, our culture, and our landscape. Our differences are our strength – but only if we remember the things that bind us together and the values we all share.
The belief that everyone should have health care is one of those universal values. From the day we are born, health care gives people the opportunity to have full lives and the vitality to pursue their dreams. And no one should lack support when illness strikes.
Over the last year, the California Health Care Foundation (CHCF) has been re-examining the work we do, because we want to make sure our efforts and our dollars are making the greatest possible impact in light of what’s happening in the world around us. As we went through that process, one unavoidable truth remained as our top concern: Too many low-income Californians are held back or suffer because it is too hard to get the care they need. Our board of directors and CHCF’s deeply committed staff have decided that the foundation’s top priority should be to address that problem.
Certainly, this undertaking will not be easy, but the good news is that there are clear ways to make health care work for low-income Californians. Here are three that are top of mind for us now.
1. All Californians Should Have Health Coverage
California has made huge gains in recent years under the Affordable Care Act (ACA). We’ve cut our number of uninsured by half. Now we must finish the job and work to ensure everyone has health benefits.
Achieving universal coverage would level the playing field in two key ways. It would allow all Californians to meet basic needs for care, and it would protect all Californians financially from extraordinary health care expenses. Today, three million of our friends and neighbors remain uninsured. Most have jobs and are contributing to our economy and communities, but those jobs do not include health insurance. We must also remember that one in three uninsured Californians is an undocumented immigrant. These people are part of the fabric of California’s society; if we allow them to remain vulnerable, all of California will pay the price.
Never has California been so close to achieving universal coverage. There is no one pathway to get to that goal, but get there we must.
2. Coverage Must Lead to Better Care
Coverage is not an end in itself – it’s really just the gateway to better health. To deliver on this promise, coverage must lead to better care. Our biggest opportunity to improve care for low-income Californians is to make sure that California’s approach to coverage for low-income populations – the Medi-Cal program – delivers high-value care. The program covers one in three Californians. And two-thirds of Californians say Medi-Cal is important to them and their families. When we get Medi-Cal right, the impact is broad and deep because of the program’s overall reach and the profound ways in which it improves a person’s prospects for health.
In the last year, we have seen major new federal threats to Medicaid’s fiscal and policy stability. Given the importance of Medi-Cal to California, we must continue working together locally and with other states to protect Medicaid from ill-advised budget and policy changes.
But it isn’t enough for California to protect the status quo. There is so much potential for improvement in Medi-Cal, which serves Californians with the greatest health burdens. We must be diligent and vigilant in finding new ways to reduce the struggle of those who depend on the program and to give them opportunities to live healthy lives. We can and should make the system easier to navigate and care easier to access. We must modernize the state’s health workforce to make treatment more effective and more cost-effective. And we can and should expect innovation in Medi-Cal to keep pace with the evolution of care in the private sector.
3. Stop Treating Conditions and Start Treating People
Our health care safety net still is organized around the outdated assumption that one person’s body and mind require two or more separate systems of care. Today we know that physical health and mental health are inextricably bound together. It is past time to update our health care system to reflect that understanding.
It is especially important that we better integrate care for low-income Californians who experience mental illness, drug or alcohol addiction, or other complex health conditions. Even though they comprise a relatively small share of the population, they account for half of health care spending. Siloed systems of care cause needless and profound suffering.
Health care leaders and providers across California have been working harder than ever to address this problem. Innovations in policy, like Medi-Cal’s Whole Person Care and Drug Medi-Cal pilots, are giving communities new opportunities to integrate care. Technology innovations can help providers extend those opportunities to larger and larger numbers of people.
Solutions Are Out There. It’s Time to Put Them to Work Everywhere.
California has the power to accomplish each of these goals. We boast the world’s sixth largest economy. California is rich in health care and innovation talent. But even with those advantages, we cannot succeed without working together across sectors, across professions, and across ideological camps.
Health care is a universal value. It will take a universal effort to make sure all Californians can meet their basic need for care.
The market economy fails when applied to healthcare.
That healthcare expenditures in the US are high and rising rapidly is nothing new, but this study appearing in the Journal of the American Medical Association identifies the exact components of healthcare that are driving those soaring costs. As F. Perry Wilson, MD points out in this 150 Second Analysis, the data suggest traditional economic forces break down in the US healthcare market.
The US spends the most of any country in the world on healthcare in terms of percent of GDP, sitting around 18% as of the most recent data.
But to address the issue, we need to understand what is driving this increase, and a new study appearing in the Journal of the American Medical Association does the best job yet in decomposing the factors behind the rising costs.
Issue: Given uncertainty about the future of the Affordable Care Act, it is useful to examine the progress in coverage and access made under the law.
Goal: Compare state trends in access to affordable health care between 2013 and 2016.
Methods: Analysis of recent data from the U.S. Census Bureau and the Behavioral Risk Factor Surveillance System.
Findings and Conclusions: Between 2013 and 2016, the uninsured rate for adults ages 19 to 64 declined in all states and the District of Columbia, and fell by at least 5 percentage points in 47 states. Among children, uninsured rates declined by at least 2 percentage points in 33 states. There were reductions of at least 2 percentage points in the share of adults age 18 and older who reported skipping care because of costs in the past year in 36 states and D.C., with greater declines, on average, in Medicaid expansion states. The share of at-risk adults without a recent routine checkup, and of nonelderly individuals who spent a high portion of income on medical care, declined in at least of half of states and D.C. These findings offer evidence that the ACA has improved access to health care for millions of Americans. However, actions at the federal level — including a shortened open enrollment period for marketplace coverage, a failure to extend CHIP funding, and a potential repeal of the individual mandate’s penalties — could jeopardize the gains made to date.
Background
The year 2017 marked a turning point in the implementation of the Affordable Care Act. Republicans in Congress attempted to repeal and replace the Affordable Care Act numerous times, ultimately failing but promising to try again. In addition, the Trump administration significantly cut funding for outreach and enrollment activities during 2018’s open enrollment period for the marketplaces, and disrupted markets by declining to pay insurers money owed to them for providing cost-reduced plans for lower-income enrollees. In December, Senate Republicans passed a tax bill that included a provision to repeal the ACA’s individual mandate penalties, paid by most people who do not have health insurance. Given these developments, many Americans are confused about the ACA’s status, which could reduce the number of people who enroll in health plans for the coming year, despite strong enrollment thus far.
It is useful to assess the changes in coverage and access that happened across states under the law before this tumultuous year. Between 2013, the year before the ACA’s major coverage expansions took effect, and the end of 2016, the number of uninsured Americans under age 65 fell by an estimated 17.8 million.1 Uninsured rates declined in every state and the District of Columbia (Exhibit 1).
In this issue brief, we examine the extent to which health care access and affordability improved from 2013 to 2016 for residents in each of the 50 states and D.C. We use six indicators: uninsured rates for working-age adults and for children, three measures of adults’ access to care, and the percentage of individuals under age 65 with high out-of-pocket medical costs relative to their income (Exhibit 2). These measures align with those reported in the Commonwealth Fund’s ongoing series of Health System Performance Scorecards.
Implications
After three years of the ACA’s major coverage expansions, the number of uninsured working-age adults and children in the United States had fallen to a record low. This historic decline was accompanied by widespread reductions in cost-related access problems and improvements in access to routine care for at-risk adults, particularly in states that expanded Medicaid. If the 19 states that have not yet expanded Medicaid decided to expand, they could see similar positive effects for their residents.
There is no deadline for adopting the Medicaid expansion. In November, Maine residents voted to expand Medicaid under a citizen-initiated ballot referendum, indicating that popular support for expanding the program may exist in states where elected officials have rejected it. While implementation in Maine could face hurdles because of opposition from the state’s governor, similar efforts are now under way in other nonexpansion states.
Actions at the federal level could, however, jeopardize the gains made under the ACA. Recent actions by the Trump administration, including a shortened open enrollment period for marketplace coverage and deep cuts in advertising and outreach, could reduce enrollment for 2018.10 In addition, Congress has yet to extend funding for the Children’s Health Insurance Program, which expired at the end of September. In the absence of an extension, more than half of states are projected to run out of federal CHIP dollars by March 2018.11 The result could be a loss of coverage for millions of children.12
Further, the tax bill passed by Senate Republicans included a repeal of the ACA’s individual mandate penalties, which would mean a cancellation of the penalties owed by people who do not take up insurance. The Congressional Budget Office estimated that repealing the penalties would reduce the number of Americans with health insurance by 13 million by 2027 and significantly increase premiums for plans purchased in the individual market. This is because healthy individuals would be the most likely to forgo coverage, leaving sicker people (who are more expensive to insure) in the risk pool.13
People who buy their own coverage on the individual market and who have incomes above 400 percent of the federal poverty level (about $48,200 for an individual and $98,400 for a family of four) — the threshold for ACA premium subsidies — would face the brunt of the premium increase.14 A recent Commonwealth Fund analysis estimates that a 40-year-old buying unsubsidized individual market coverage in one of the 39 states that uses the federally facilitated marketplace would face an average dollar increase in premiums ranging from $556 in North Dakota to $1,264 in Nebraska (Exhibit 10).15
Rather than defining addiction as destructive, compulsive behavior, this ideology focuses on physical dependence. If you need a drug to avoid being physically ill, you are considered addicted. So Prozac would be considered addictive, but not cocaine, because quitting Prozac abruptly can cause flulike symptoms while stopping cocaine doesn’t, even though it elicits extreme craving.
In the 1980s, crack cocaine made clear just how addictive cocaine could be, even without physical withdrawal symptoms. Today, both the National Institute on Drug Abuse and the Diagnostic and Statistical Manual of Mental Disorders reject the idea that addiction is synonymous with dependence. Unfortunately, many clinicians, including doctors, haven’t caught up.
What is addiction, then? The root problem is craving, which drives a compulsion to use drugs despite the harm they cause. That’s what makes crack addictive, while Prozac can be therapeutic.
Because methadone and buprenorphine are opioids themselves, it’s easy to assume that using them is “substituting one addiction for another.” However, the pattern of taking the same dose every day at the same time means that there is no high or intoxication. Patients on maintenance doses are able to nurture a baby, drive, work and be a loving spouse.
In these patients, addiction is replaced by physical dependence. And that’s not a problem for those who have health care coverage: It’s no different from needing antidepressants or insulin. When a drug’s benefits outweigh its risks, continued use is healthy, not addictive.
Sadly, though, there’s another reason for widespread skepticism about addiction medication. It comes from the fact that many patients will continue to misuse opioids. Medication reduces relapse more than abstinence does — but relapse is still common, as in Mr. Thompson’s case. In abstinence treatment, however, relapsers drop out and are invisible; with medication, they often remain in treatment.
And remaining in treatment is important because it cuts overdose risk, even during relapse. Many highly traumatized people also need the continued health care support before they are able to quit street drugs.
When we fail to understand that these medications can be used both to reduce harm and stabilize people in recovery, we risk letting the perfect be the enemy of the good. For some, medication is a way to reduce risk while drug use continues. For others, it’s a path to rapid recovery. Often, people will need to take the first route to survive long enough to reach the second.
For harm reduction to work, maintenance drugs need to be almost as accessible as street drugs. Whenever people take buprenorphine rather than heroin, their risk of dying is lowered, especially since so much heroin these days is tainted with deadly strong fentanyl. For stabilization, people need empathetic counseling that doesn’t view dependence as continuing addiction.
Change will require innovative measures. The government should stop funding and insurers should stop covering any program that does not use all the F.D.A.-approved anticraving medications and does not provide informed consent about their effectiveness. While abstinence can work for some, we need many options. We also need to rethink our regulations for methadone and buprenorphine prescribing.
Then we need to publicly recognize that recovery on medication is every bit as valid as any other treatment. What matters is whether, as Freud put it, you can love and work, not the chemical content of your brain or urine.
Earlier this week, Amazon.com Inc., JPMorgan Chase & Co., and Berkshire Hathaway Inc. jolted Wall Street with their announcement of a joint venture designed to reduce health care costs for their combined one million US employees. It is exciting to see innovative private sector companies lend their intellectual and financial capital to a seemingly intractable issue that has plagued the American economy for decades. About 18 percent of our nation’s financial output is now devoted to health care. For decades, health care costs have outpaced overall economic growth, and the gap is projected to remain to remain at three percentage points a year.
How the High Cost of Care Affects Employers – and Everyone Else
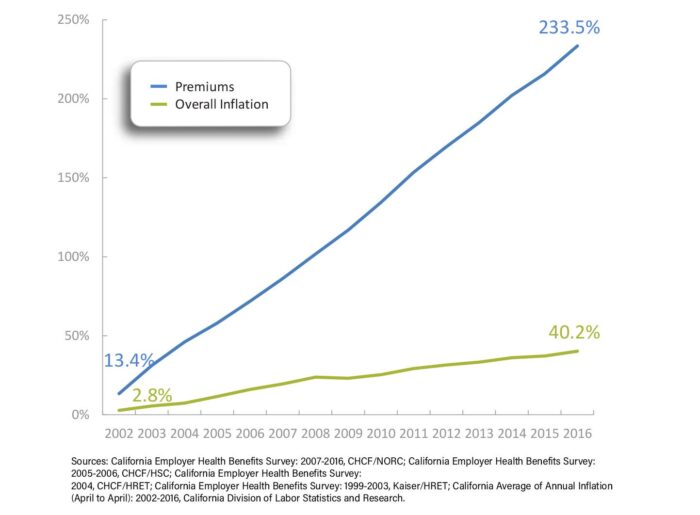
Employees directly and indirectly shoulder these costs. The average premium that employers and their workers pay for a family plan in California now exceeds $1,600 a month. Employer-based family health insurance premiums in the state have increased by 234% over the last 15 years, nearly six times the increase in the state’s overall inflation rate. Every dollar spent on health care is a dollar unavailable for something else, such as education, affordable housing, and environmental protection.
Sixty-six percent of working California families face a deductible of $2,000 or more for their employer-based coverage, including many without high-deductible health plans linked to tax-advantaged health savings accounts.
Increasingly, health care is unaffordable for all of us—not just businesses like Amazon and its workers, but for retirees, the self-employed, people seeking employment, and low-income Californians who aren’t eligible for public coverage. The Affordable Care Act (ACA) attempted to address the cost burden for those with employer coverage by creating disincentives for employers to simply pass on unaffordable premiums, and by capping the share of premiums health plans spent on overhead and profit. For people who shop for insurance coverage on the individual market, the ACA provided federal tax credits to offset premium and cost sharing.
While these and other efforts have helped, more work is needed. Too many families still struggle to afford health care. In 2017, 37% of Americans with health insurance found it difficult to afford premiums each month. Forty-three percent said it was hard to meet their deductibles before coverage kicked in. Among California workers with an aggregate family deductible, 66% faced a deductible of $2,000 or more in 2016.
At least 40% of adults say they worry about being able to afford health care services, losing their insurance, or being able to afford prescription drugs.
What We Already Know About Reducing Health Care Costs
Addressing the affordability of care in California and throughout the country requires lowering the underlying cost of care across market segments. Many efforts are already underway. Health insurance companies, large self-funded employers, and public purchasers of care often deploy management strategies to reduce the use of expensive tests, high-cost prescription drugs, and duplicative services. The most common strategies include prior authorization, patient education for better clinical decisionmaking, chronic disease initiatives, and pushing the cost to employees through deductibles and other cost-sharing tools.
To date, the results of these initiatives have been mixed. The findings are consistent with a growingbody of academicresearch that suggests the real driver of health care costs is price, not increased demand. If that is the case, the solution might be to create a market that rewards high-value providers and cost-effective drugs. This type of strategy would rely on tools like reference pricing (individual drugs are grouped by therapeutic class and payment is limited to the price of the cheapest drugs in each class), value-based insurance design (copayments are reduced or eliminated for the most efficient, effective services), or high-deductible health plans.
Unfortunately, consumer-driven approaches have also had limited impact. While companies like Amazon might develop new technologies to enable patients to easily compare, shop for, and purchase health care services in a competitive marketplace, to date these types of tools have not succeeded in reducing costs or changing provider behavior in California. More to the point, introducing blunt consumer-facing financial incentives may run counter to the overall goal of affordability. Everyone should have access to the care they need at a price they can afford and not face care that is rationed by their ability to pay for it.
The Promise of Scale
Perhaps the biggest advantage of the new joint venture is its size and reach. The most promising solutions today are found in large, integrated delivery systems. They have consistently shown that the best approach is to give providers simple, strong financial incentives to make care more efficient and effective. Because this type of model works best on a large scale, the ideal approach is for multiple public and private purchasers of care to come together to align quality reporting requirements, reward value, and support investments in improving health outcomes across entire groups of people. We are already seeing this happen in California and other states.
No one group or slice of the private health care market has the power to really drive down health care costs for everyone. It will take many, many players in the private and public sectors working together to align their efforts. The foundation of payment and delivery reform laid by the Affordable Care Act is a good place to start. Technology is critical and necessary – but it is not by itself sufficient. Leaders also need to pull policy levers, fix payment systems, and spark collaboration between purchasers. Innovators like Amazon, JPMorgan Chase, and Berkshire Hathaway will no doubt make material contributions. Their leadership, in tandem with that of other large purchasers, offers a prime opportunity to make care more affordable for everyone.
WASHINGTON — Federal investigators say they have found huge gaps in the regulation of assisted living facilities, a shortfall that they say has potentially jeopardized the care of hundreds of thousands of people served by the booming industry.
The federal government lacks even basic information about the quality of assisted living services provided to low-income people on Medicaid, the Government Accountability Office, a nonpartisan investigative arm of Congress, says in a report to be issued on Sunday.
Billions of dollars in government spending is flowing to the industry even as it operates under a patchwork of vague standards and limited supervision by federal and state authorities. States reported spending more than $10 billion a year in federal and state funds for assisted living services for more than 330,000 Medicaid beneficiaries, an average of more than $30,000 a person, the Government Accountability Office found in a survey of states.
States are supposed to keep track of cases involving the abuse, neglect, exploitation or unexplained death of Medicaid beneficiaries in assisted living facilities. But, the report said, more than half of the states were unable to provide information on the number or nature of such cases.
Just 22 states were able to provide data on “critical incidents — cases of potential or actual harm.” In one year, those states reported a total of more than 22,900 incidents, including the physical, emotional or sexual abuse of residents.
Many of those people are “particularly vulnerable,” the report said, like older adults and people with physical or intellectual disabilities. More than a third of residents are believed to have Alzheimer’s or other forms of dementia.
The report provides the most detailed look to date at the role of assisted living in Medicaid, one of the nation’s largest health care programs. Titled “Improved Federal Oversight of Beneficiary Health and Welfare Is Needed,” it grew out of a two-year study requested by a bipartisan group of four senators.
Assisted living communities are intended to be a bridge between living at home and living in a nursing home. Residents can live in apartments or houses, with a high degree of independence, but can still receive help managing their medications and performing daily activities like bathing, dressing and eating.
Nothing in the report disputes the fact that some assisted living facilities provide high-quality, compassionate care.
The National Center for Assisted Living, a trade group for providers, said states already had “a robust oversight system” to ensure proper care for residents. In the last two years, it said, several states, including California, Oregon, Rhode Island and Virginia, have adopted laws to enhance licensing requirements and penalties for poor performance.
But the new report casts a harsh light on federal oversight, concluding that the Centers for Medicare and Medicaid Services has provided “unclear guidance” to states and done little to monitor their use of federal money for assisted living.
As a result, it said, the federal health care agency “cannot ensure states are meeting their commitments to protect the health and welfare of Medicaid beneficiaries receiving assisted living services, potentially jeopardizing their care.”
Congress has not established standards for assisted living facilities comparable to those for nursing homes. In 1987, Congress adopted a law that strengthened the protection of nursing home residents’ rights, imposed dozens of new requirements on homes and specified the services they must provide.
But assisted living facilities have largely escaped such scrutiny even though the Government Accountability Office says the demand for their services is likely to increase because of the aging of the population and increased life expectancy.
That potential has attracted investors. “Don’t miss out on the largest market growth in a generation!” says the website of an Arizona company, which adds that “residential assisted living is the explosive investment opportunity for the next 25 years.”
Carolyn Matthews, a spokeswoman for the company, the Residential Assisted Living Academy, said: “Unfortunately, there has been elderly abuse in this business. We are trying to change the industry so the elderly have better quality care and we are not warehousing them.”
The government report was requested by Senator Susan Collins of Maine, a Republican who is the chairwoman of the Special Committee on Aging; Senator Orrin G. Hatch of Utah, a Republican who is the chairman of the Finance Committee; and two Democratic senators, Claire McCaskill of Missouri and Elizabeth Warren of Massachusetts.
The Trump administration agreed with the auditors’ recommendation that federal officials should clarify the requirement for states to report on the abuse or neglect of people in assisted living facilities. The administration said it was studying whether additional reporting requirements might be needed.
“Although the federal government has comprehensive information on nursing homes providing Medicaid services, not much is known about Medicaid beneficiaries in assisted living facilities,” the report said.
Assisted living was not part of the original Medicaid program, but many states now cover it under waivers intended to encourage “home and community-based services” as an alternative to nursing homes and other institutions.
The report said that assisted living could potentially save money for Medicaid because it generally cost less than nursing home care. Under the most common type of waiver, Medicaid covers assisted living only for people who would be eligible for “an institutional level of care,” in a nursing home or hospital.
Nine states are considering laws that would require their residents to purchase health insurance, the The Wall Street Journal reported Saturday.
The proposals come less than two months after Republicans, as part of a sweeping tax code overhaul, voted to repeal the Affordable Care Act’s (ACA) mandate requiring individuals to have health insurance.
Lawmakers in Maryland are considering a law requiring residents to buy health insurance. California, Connecticut, Hawaii, Minnesota, New Jersey, Rhode Island, Vermont and Washington, as well as the District of Columbia, are also considering similar proposals, according to the Journal report.
The ACA’s individual mandate was implemented as a way to keep premiums low by requiring everyone to have insurance. Proponents of the mandate say that, without it, healthy people are less inclined to buy insurance, causing premiums to rise for those who need it the most.
But Republicans have long argued against the idea that people should be forced to purchase health coverage.
The decision to repeal the mandate as part of the GOP tax bill was touted as a victory in Republicans’ effort to repeal the ACA. While the provision did not do away with the entire law, it was a blow.
The proposals to impose health coverage mandates in some states marks a shift of authority over health care from the federal government to the states, possibly leading to significant coverage differences between red states and blue states.
“The federal government has just stalled. They don’t accomplish the basics, and that leaves states with a great opportunity to step up and craft policy,” Connecticut state Rep. Sean Scanlon (D), who sits on a health-care working group, told the Journal.
For over 50 years, the program for the poor and sick has been required to ferry certain clients to and from medical appointments. Though California is not among the states out to cut this service, it could feel the pinch if the feds slash Medicaid funding overall.
This special series examines the reach and the role of Medicaid, the federal-state program that began as a medical program for the poor but now provides a wide variety of services for a large swath of America.
EVERETT, Wash. — Unable to walk or talk, barely able to see or hear, 5-year-old Maddie Holt waits in her wheelchair for a ride to the hospital.
The 27-pound girl is dressed in polka-dot pants and a flowered shirt for the trip, plus a red headband with a sparkly bow, two wispy blond ponytails poking out on top.
Her parents can’t drive her. They both have disabling vision problems; and, besides, they can’t afford a car. When Maddie was born in 2012 with the rare and usually fatal genetic condition called Zellweger syndrome, Meagan and Brandon Holt, then in their early 20s, were plunged into a world of overwhelming need — and profound poverty.
“We lost everything when Maddie got sick,” said Meagan Holt, now 27.
Multiple times each month, Maddie sees a team of specialists at Seattle Children’s Hospital who treat her for the condition that has left her nearly blind and deaf, with frequent seizures and life-threatening liver problems.
The only way Maddie can make the trip, more than an hour each way, is through a service provided by Medicaid, the nation’s health insurance program started more than 50 years ago as a safety net for the poor.
Called non-emergency medical transportation, or NEMT, the benefit is as old as Medicaid itself. From its inception, in 1966, Medicaid has been required to transport people to and from such medical services as mental health counseling sessions, substance abuse treatment, dialysis, physical therapy, adult day care and, in Maddie’s case, visits to specialists.
“This is so important,” said Holt. “Now that she’s older and more disabled, it’s crucial.”
More than 1 in 5 Americans, about 74 million people, now rely on Medicaid to pay for their health care. In California, one-third of the population — about 13.5 million people — are enrolled in the state’s Medicaid program, called Medi-Cal.
Nationally, the numbers have grown dramatically since the program expanded in California and 31 other states, plus the District of Columbia, to cover prescription drugs, health screening for children, breast and cervical cancer treatment and nursing home care.
With a Republican administration vowing to trim Medicaid, Kaiser Health News is examining how the U.S. has evolved into a “Medicaid Nation,” where millions of Americans rely on the program, directly and indirectly, often unknowingly.Medicaid’s role in transportation is a telling example. Included in the NEMT coverage are nearly 104 million trips each year at a cost of nearly $3 billion, according to a 2013 estimate, the most recent, by Texas researchers.
Citing runaway costs and a focus on patients taking responsibility for their health, Republicans have vowed to roll back the benefits, cut federal funding and give states more power to eliminate services they consider unaffordable.
Already, states have wide leeway in how to provide and pay for the transportation.
In California, Medi-Cal members in managed care get transportation through their health plans, while fee-for-service enrollees can arrange for the service through their counties, said Amber Christ, a Los Angeles-based staff attorney for Justice in Aging, a legal advocacy group.
Medi-Cal transportation is a “lifeline” for the low-income seniors she works with, she said.
“Most of them cannot afford a car, or if they have a car they can’t afford to keep gas in that car, or they can’t use public transportation,” she said. “Medicaid transportation is the only way they are going to their doctor appointments.”
California has not proposed cutting this service, but should the federal government slash Medicaid funding overall, “you could see where states would feel the pressure to make cuts, and this might be one of the first places to do that,” Christ said.
Proponents of limiting NEMT say the strategy will cut escalating costs and more closely mirror private insurance benefits, which typically don’t include transportation.
They also contend that changes will help curb what government investigators in 2016 warned is “a high risk for fraud and abuse” in the program. In recent years, the Centers for Medicare & Medicaid Services (CMS) reported that a Massachusetts NEMT provider was jailed and fined more than $475,000 for billing for rides attributed to dead people.
Last year, a public interest law office in Los Angeles sued a company contracted to provide transportation to Medicaid enrollees in California and other states for allegedly failing to provide “safe, reliable and timely transportation” to fragile patients — some with brain injuries and amputations. That caused them to miss appointments, the suit alleges.
Two ambulance programs in Connecticut paid almost $600,000 to settle claims that they provided transportation for dialysis patients who didn’t have medical needs for ambulance transportation. And the mother of a Medicaid patient who was authorized to transport her child for treatment billed Medicaid for trips that didn’t take place. She was sentenced to 30 days in jail and ordered to pay $21,500.
Last March, Rep. Susan Brooks, an Indiana Republican, introduced a resolutionthat would have revoked the federal requirement to provide NEMT in an effort to provide states with “flexibility.” That effort stalled.
Another Republican proposal in 2017 would have reversed the Affordable Care Act’s Medicaid expansion and reduced federal funding for the NEMT program. It failed, but other efforts by individual states still stand.
Former Health and Human Services Secretary Tom Price and CMS Administrator Seema Verma encouraged the nation’s governors to consider NEMT waivers, among other actions, in a March letter to them.
“We wish to empower all states to advance the next wave of innovative solutions to Medicaid challenges,” they wrote. The Trump administration has used state waivers to bypass or unravel a number of the Obama administration’s more expansive health policies, and has granted some states’ requests.
At least three states, Iowa, Indiana and Kentucky, have received federal waivers — and extensions —allowing them to cut Medicaid transportation services. Massachusetts has a waiver pending.
Critics of the cuts worry the trend will accelerate, leaving poor and sick patients with no way to get to medical appointments.
“I wouldn’t be surprised to see more of these waivers in the pipeline,” said Joan Alker, executive director of the Georgetown University Center for Children and Families.
Because medical transportation isn’t typically covered by the commercial insurance plans most Americans use, it’s unfamiliar to many people and could be seen as unnecessary, said Eliot Fishman, senior director of health policy for Families USA, a nonprofit, nonpartisan consumer health advocacy group.
Formerly a Medicaid official in the federal government, Fishman called the transportation program “vital” not only for children with severe disabilities, but also for non-elderly, low-income adults.
CMS released results of a 2014 survey of Medicaid users, which found that lack of transportation was the third-greatest barrier to care for adults with disabilities, with 12.2 percent of those patients reporting they couldn’t get a ride to a doctor’s office.
“This is not something to be trifled with lightly,” Fishman said. “We’re talking about a lifesaving aspect of the Medicaid program.”
About 3.6 million Americans miss or delay non-emergency medical care each year because of transportation problems, according to a 2005 study published by the National Academy of Sciences.
That same study analyzed costs for providing NEMT to patients facing 12 common medical conditions and found that providing additional transportation is cost-effective. For four of those conditions — prenatal care, asthma, heart disease and diabetes — medical transportation saved money when the total costs for both transportation and health care were tallied.
Medicaid is required to provide NEMT services using the most appropriate and least costly form of transportation, whether that’s taxis, vans or public transit.
Most states rely on NEMT brokers or managed-care organizations to administer the transportation services. Other states run the service directly, paying providers on a per-ride basis, while some use local ride services and pay independent taxi firms to shuttle patients.
Proponents of revamping NEMT note that disabled children like Maddie and other people with serious disabilities are in little danger of losing services. In Iowa and Indiana, Medicaid transportation remains available to several groups of patients, including those classified as “medically frail,” though the definition of who qualifies can vary widely.
In addition, one managed-care provider, Anthem, continues to transport Indiana Medicaid patients, despite the waiver that was first enacted in 2007.
Still, Medicaid clients like Fallon Kunz, 29, of Mishawaka, Ind., are often stuck. Kunz, who has cerebral palsy, migraine headaches and chronic pain, uses a power wheelchair. When she was a child, she qualified for door-to-door service to medical appointments, she said.
Today, she lives with her father, whose home is outside the route of a Medicaid transit van. Getting to and from medical appointments for her chronic condition is a constant struggle, she said. Taxis are too expensive: $35 each way for a wheelchair-enabled cab.
“The only way I can get rides to and from my doctor’s appointment is to ride the 2 miles in my wheelchair, despite all kinds of weather, from my home, across the bridge, to the grocery store,” she said. “Right outside the grocery store is the bus stop. I can catch the regular bus there.”
Sometimes, she’s in too much pain or the Indiana weather — warm and humid in the summer, frigid and windy in the winter — is too much to battle and she skips the appointment.
“Today I didn’t go because it was too cold and my legs hurt too much,” she said on a December Tuesday. “I didn’t feel like getting blown off the sidewalk.”
In Maddie Holt’s case, she was shuttled to Seattle Children’s on a rainy Tuesday morning in a medical van driven by Donavan Dunn, a 47-year-old former big-rig trucker. He works for Northwest Transport, one of several regional brokers that manage NEMT services for Washington state.
Dunn said he received special training to transport patients like Maddie, who is loaded onto a motorized platform, wheelchair and all, into the van and then carefully strapped in.
“I have to drive different,” said Dunn. “I have to watch my corners, watch my starts, watch my stops. It’s always in the back of my mind that I have somebody on board that’s fragile.”
We’re talking about a lifesaving aspect of the Medicaid program.
The transportation service can be used only for medical visits to the specialists who treat Maddie’s condition, which is caused by mutations in any one of at least 12 genes. If Meagan Holt needs to pick up prescriptions or get groceries, she leaves Maddie and a second daughter, Olivia, 3, at home with their dad and takes the bus or walks to her destinations.
Caring for a severely disabled child is not the life she expected, Meagan Holt said, but she cherishes time with Maddie, who has learned to communicate through tactile sign language spelled into her hand.
“She knows about 100 words. She knows the alphabet,” Meagan said. “She likes Disney princesses. She loves ‘Frozen.’”
Maddie is one of hundreds of NEMT-eligible children transported to Seattle Children’s each month. Last September, for instance, more than 1,300 clients made more than 3,600 trips at a cost of more than $203,000, according to the Washington Health Care Authority, which oversees the state’s Medicaid program called Apple Health.
The need is so great, in fact, that the hospital created a transportation will-call desk to help organize the comings and goings.
“When we realized how much transportation is a barrier to getting to your appointment, we decided to do something about it,” said Julie Povick, manager of international exchanges and guest services at Seattle Children’s.
“The majority of our patients are in survival mode,” Povick added. “You need a lot of handholding.”
But Verma, the architect of Indiana’s Medicaid overhaul plan, has suggested that too much handholding might be “counterproductive” for patients — and bad for the country.
In a 2016 Health Affairs essay, Verma noted that early analysis of the effects of curtailing NEMT in Indiana showed that more Medicaid patients with access to the program said transportation was a primary reason for missed appointments than did members without access.
“Moreover, 90 percent of [Healthy Indiana Plan] members report having their own transportation or the ability to rely on family and friends for transportation to health care appointments,” she wrote.
But Marsha Simon, a Washington, D.C., health policy consultant who has tracked NEMT for years, said Medicaid is the option of last resort. People who are able to get rides on their own already do.
“If 90 percent can and 10 percent can’t, what about the 10 percent?” Simon said.
It’s a question that haunts Kunz every day.
“I’m a college student, I have a cat,” said Kunz, who is studying psychology online at Southern New Hampshire University. “I’m just a regular human trying to do things, and the inaccessibility in this area is ridiculous.”