As we’ve discussed before, the greatest challenge facing health system economics is demographics. Simply put, with 80M Boomers entering their Medicare years, hospitals beds will fill with elderly patients receiving treatment for exacerbations of congestive heart failure (CHF), diabetes, or other chronic conditions, of which the average Medicare beneficiary has four. It’s easy to envision the hospital becoming a giant nursing facility, with the vast majority of beds occupied by Medicare patients receiving nursing care and drugs, only to be sent home until their chronic disease flares again and the cycle repeats, four or five times a year.
Health systems must create a new model for managing Medicare patients with multiple chronic conditions, one that does not rely on care delivered in an inpatient setting. In the graphic below, we outline two approaches for managing a Medicare patient with advanced CHF. The top path illustrates today’s legacy model, where limited support for ongoing care management leaves the patient vulnerable to exacerbations, leading to numerous ED visits and admissions for diuresis, after which the patient returns home to a sub-optimal diet and lifestyle and is likely to return.
A better alternative is illustrated in the second path. Here our CHF patient has access to the ongoing support of a care team, which regularly monitors her status from home with the help of remote monitoring and can communicate with the patient to adjust therapy if early symptoms are detected. At Gist, we’re working with clinicians to understand just how to build this system of care and maximize its impact.
One example: a leading heart failure specialist told us that admissions for CHF could be reduced by one-third if patients with severe heart failure were monitored with a CardioMEMS implantable device, which can detect changes in pressure before the patient has symptoms, allowing for very early intervention. Developing these kind of care approaches to manage chronic disease outside the hospital will be the key to sustainable health system economics—and may have the greatest impact on lowering the total cost of care for the growing Medicare population.
The Residences at Camelback West in Phoenix has 500 rental units ranging from studios to two-bedroom apartments, of which 100 are set aside for homeless UnitedHealth Medicaid members. Photo: Tiempo Development & Management
In the course of a single year, a homeless man named Steve in Phoenix, Arizona, visited the emergency room 81 times. Only 54 years old, Steve is coping with a daunting array of medical conditions: multiple sclerosis, cerebral palsy, heart disease, and diabetes. Because of his health and reliance on emergency rooms, his medical costs averaged about $13,000 per month that year.
Thanks to an innovative housing program run by the nation’s largest health insurer, UnitedHealth Group, Steve no longer sleeps outside — a crucial prerequisite to improved health. He is one of about 60 formerly homeless people covered by Arizona Medicaid who now receive housing and support services in Phoenix, John Tozzi reported for Bloomberg Businessweek. The UnitedHealth housing program, called myConnections, represents the growing recognition across the health care system that improved health cannot be achieved exclusively by traditional clinical models. Getting patients off the streets is often the first — and most important — step to helping them heal, physically and mentally.
“Patients like Steve wind up in the ER because they don’t fit into the ways we deliver health care. . . . [The US system] is not set up to keep vulnerable people housed, clothed, and nourished so they’ll be less likely to get sick in the first place. —John Tozzi, Bloomberg News
“Patients like Steve wind up in the ER because they don’t fit into the ways we deliver health care,” Tozzi explained. “The US system is engineered to route billions of dollars to hospitals, clinics, pharmacies, and labs to diagnose and treat patients once they’re sick. It’s not set up to keep vulnerable people housed, clothed, and nourished so they’ll be less likely to get sick in the first place.”
MyConnections was the brainchild of a partnership between UnitedHealthcare (a division of UnitedHealth) and the Camden Coalition, a New Jersey–based nonprofit dedicated to improving care for people with complex health and social needs. The partnership was established in 2017 at the same time Jeffrey Brenner, MD, founder and executive director of the Camden Coalition, announced he was leaving the nonprofit to lead myConnections. He is now UnitedHealthcare’s senior vice president for integrated health and human services. UnitedHealthcare provides managed care to about six million people nationwide, according to company filings. It does not get reimbursed by Medicaid for housing assistance.
Making the Case for Addressing Social Determinants
Brenner hopes myConnections will show that both a health care and a business case can be made for investing in a Housing First (PDF) model. Tozzi reported that UnitedHealth “aims to reduce expenses not by denying care, but by spending more on social interventions, starting with housing.”
At the Residences at Camelback West, a Phoenix apartment complex of 500 apartments ranging from studios to two-bedroom units, up to 100 apartments are set aside for UnitedHealth Medicaid members enrolled in myConnections. The rest of the units are rented out at market rates. Five health coaches use an on-site office to serve as case managers and counselors for the myConnections residents. The coaches make sure that their clients remember medical appointments, and arrange transportation for them and sometimes accompany them to the doctor.
Since receiving housing and health coaching from Brenner’s team, Steve’s average monthly medical costs have dropped from $12,945 to $2,073. An analysis of the first 41 participants in Phoenix shows that “housing and support services proved cost effective for the 25 most expensive patients, reducing their overall costs dramatically,” Tozzi reported. But total spending for the other 16 increased, highlighting the complexity of this work.
“The return’s only going to work out if we target the right people,” Brenner told Tozzi. The myConnections team selects patients who are enrolled in UnitedHealth, are homeless, and who have annual medical spending greater than $50,000 mostly because of ER visits and inpatient stays. Those high-cost patients are UnitedHealth’s best bet for recovering the cost of its housing investment.
UnitedHealth is starting with 10 subsidized apartments in each new city where it’s introducing the program, including in places where there might be hundreds of homeless Medicaid members on its rolls, Tozzi reported. MyConnections will be in 30 markets by early 2020.
Kaiser Addresses Homelessness in Its Backyard
In its home base of Oakland, California, health system Kaiser Permanente has invested $200 million in an affordable housing project, Hannah Norman reported in the San Francisco Business Times. Its help is not targeted exclusively at Kaiser members, instead aiming to benefit any residents who live in communities it serves.
The initiative was championed by Bernard Tyson, the late chairman and CEO of Kaiser, who died unexpectedly this month. In a New York Times remembrance, Reed Abelson noted that Tyson was committed to addressing social determinants of health in the places where Kaiser operates. “He had the organization examine broad issues like housing shortages, food insecurity, and gun violence and their impact on health and well-being,” Abelson wrote.
Tyson, who was the health system’s first Black chief executive, served as chair of the Bay Area Council, a business association dedicated to economic development in the San Francisco region. His chairmanship culminated in a major report (PDF) that documented the severity of the homelessness crisis and recommended ways to address it, Norman reported.
“We don’t believe as a mega-health system that our only lane is medical care,” Tyson said in April. “It’s a critical lane, but it’s not our only lane.”
Steady Rents in Buildings with Seismic Upgrades
Kaiser announced its $200 million housing initiative, the Thriving Communities Fund, in January. Since then, it partnered with Enterprise Community Partners, a nonprofit organization focused on affordable housing, and the nonprofit East Bay Asian Local Development Corporation to invest a total of $8.7 million ($5.2 million from Kaiser) in Kensington Gardens, a 41-apartment building in East Oakland. “The trio of organizations plans to keep the residents in place and the rent steady at $1,597 per month for a studio and $2,250 for a two-bedroom,” Norman wrote. “Some residents receive federal housing benefits, including Section 8, to help cover the cost.”
The Kensington Gardens purchase is part of the Thriving Communities Fund’s strategy to keep rents steady and to make health and safety upgrades such as seismic upgrades and new roofs.
Kaiser’s Built for Zero initiative committed $3 million over three years to a data-driven, county-level approach to understanding the dynamics of homelessness. Built for Zero tracks the homeless population in a county from month to month to understand “who they are, what they need, and even how many of them are repeatedly visiting emergency rooms,” Norman reported. Fifteen Kaiser communities, including eight in California, are participating in the program.
The health troubles we’re seeing now — especially among young people — will continue to strain the system for years and even decades to come.
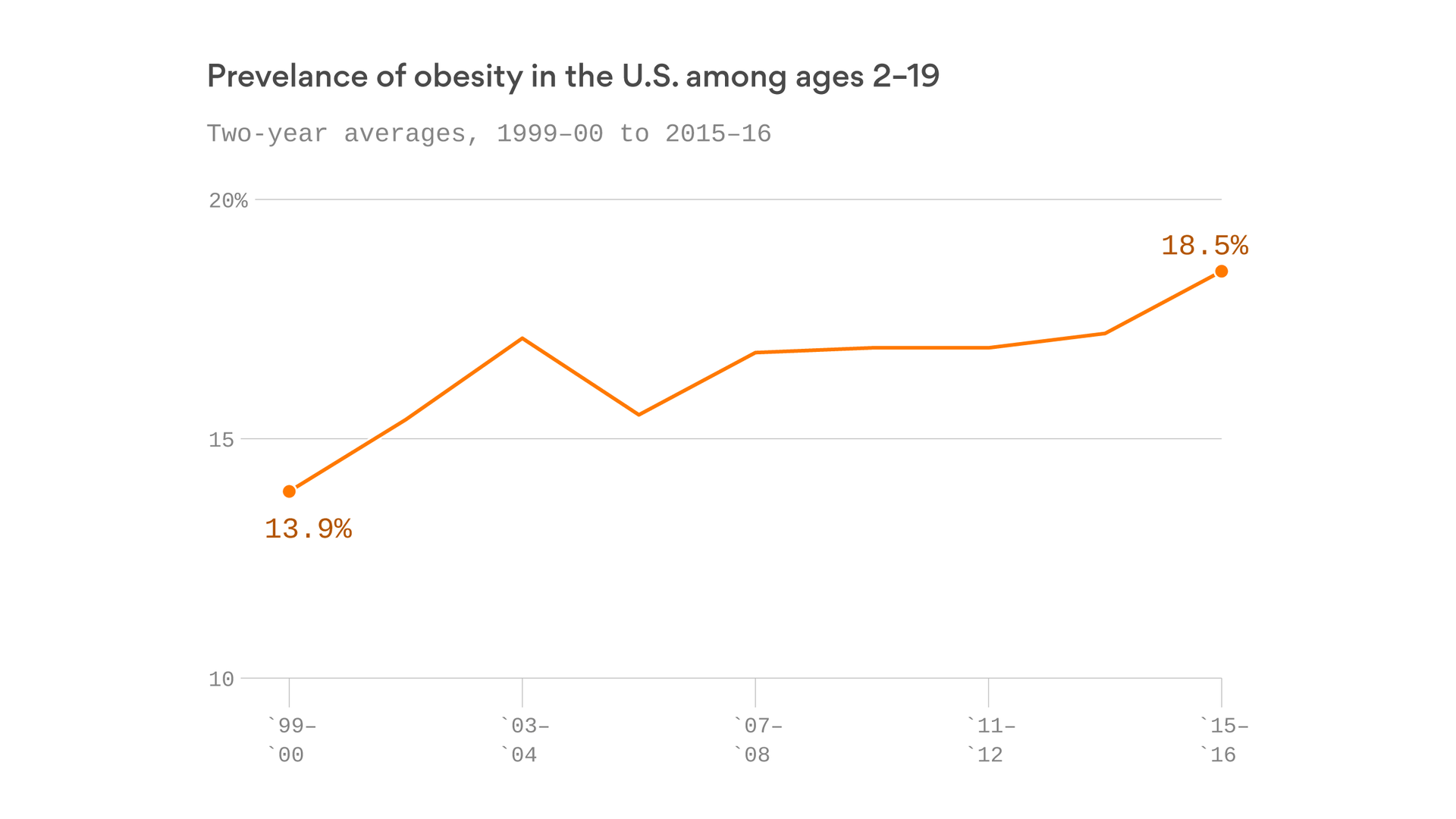
The big picture: Rising obesity rates nowwill translate into rising rates of type 2 diabetes and heart disease. The costs of the opioid crisis will continue to mount even after the acute crisis ends. And all of this will strain what’s already the most expensive health care system in the world.
By the numbers: 18% of American kids are now obese, according to new CDC data. So are roughly 40% of adults. And it’s projected to get worse.
That helps explain why diabetes rates are also rising, and why roughly 30% of adults have high blood pressure.
Why it matters: More obese children means there will be more adults down the road with chronic conditions like diabetes — which can’t be cured, only managed — and these diseases in turn increase the risk of further complications, such as kidney disease and stroke.
Diabetes roughly doubles your lifetime health care bills, according to the CDC, and costs the U.S. a total of $245 billion per year.
As the price of insulin continues to skyrocket, the disease only gets harder for patients to manage, if they can afford treatment at all.
We’re only beginning to see the full costs of the opioid crisis, even though it has raged for years.
A White House report earlier this week pegged the cost of the epidemic at a staggering $696 billion last year alone, including the cost of productivity lost to addiction.
The tide has only barely begun to turn on overall overdose deaths — they still numbered around 68,000 last year.
And many survivors of the epidemic will face long-term health costs. Addiction recovery can be a lifelong process requiring sustained investments. It has also led to skyrocketing rates of Hepatitis C — some states have seen their infection rates rise by more than 200% over the past decade.
Groundbreaking new treatments offer the first-ever cure for Hepatitis C, but at price tags so high that states are experimenting with entirely new ways of paying for the drugs, fearing the status quo simply can’t bear these costs all at once.
The bottom line: The flaws in the U.S. health care system compound one another.
They reward doctors and hospitals for performing more treatment on sick people, and those treatments are expensive. That leaves big gaps in prevention, which drives the need for more expensive treatment.
That’s how we ended up with the world’s most expensive health care system, but without a particularly healthy population to show for it. And that trajectory isn’t changing.