The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
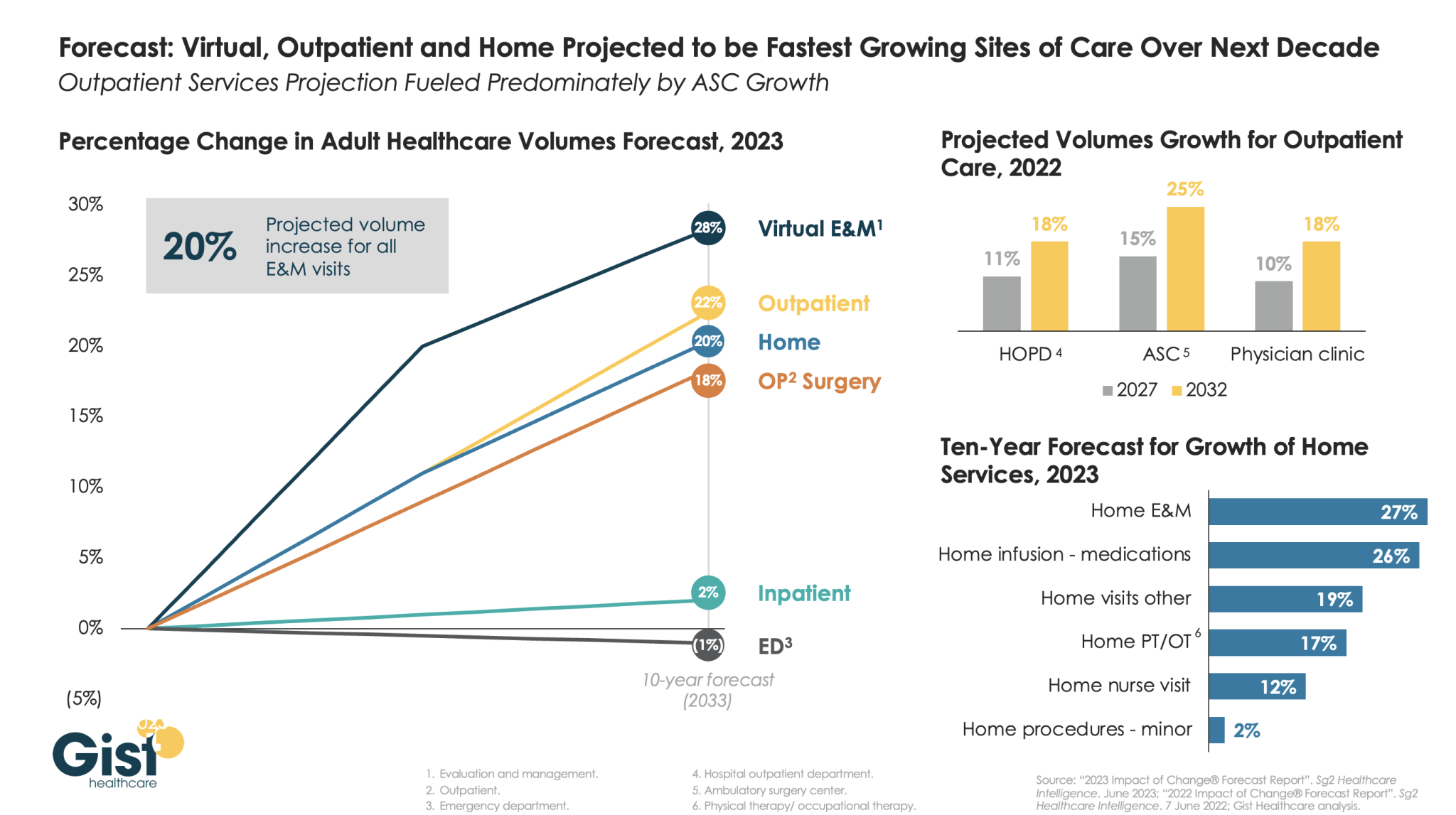
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
Driven in large part by the growth of Medicare Advantage, a number of startups are vying to create the next value-based care model for senior care in patients’ homes, Axios’ Sarah Pringle reports.
Why it matters: As we recently reported in our Elder Care Crisis Deep Dive, there is a shortfall of enough cash and caregivers to handle the massive amount of aging baby boomers reaching their senior years.
“The cool thing about value-based care?” General Atlantic managing director Robb Vorhoff said. “There’s hundreds of business models.”
Reality check: Scaling remains a challenge for new models looking to shake up the senior care market.
“There are a lot of options out there that you don’t know about,” Town Hall Venture’s Andy Slavitt says. “Some are the best-kept secrets; some are not worth knowing about.”
Be smart: While most elderly adults would prefer to age in place, there is still a need for institutional care settings like nursing homes, which presents its own major challenges, Sarah writes.
Amazon and several other major companies have made numerous attempts to “disrupt” health care over the years without much success. But new acquisitions in primary care, home health care, and more may allow them to more successfully expand into the industry, David Wainer writes for the Wall Street Journal.
Competition heats up in the health care industry
According to Wainer, the United States spends a greater proportion of its economy on medical services than any other developed nation, making health care “too big of an opportunity to ignore” for many companies, including those in technology, retail, and more.
For example, Amazon has launched several forays into health care in recent years, although not all of them have been successful. Some of these health care efforts include its now defunct partnership with Berkshire Hathaway and JPMorgan Chase, as well as Amazon Care, the company’s primary care service that will shut down at the end of the year.
Amazon has also acquired several smaller health care companies in an effort to expand its reach. In 2018, Amazon purchased PillPack for $1 billion as a way to expand its online pharmacy business. Similarly, Amazon in July reached an agreement to acquireOne Medical, a primary care company, for roughly $3.9 billion.
Several other companies, including retailers like Walmart and Walgreens and large insurers like UnitedHealth Group* (UHG) and CVS Health‘s Aetna, are also looking to expand their health care offerings. In fact, CVS announced last week that it had purchased home health care company Signify Health for roughly $8 billion—beating out several other competitors.
So far, “[s]hifting social attitudes and market conditions have helped fuel the wave” of health care acquisitions from major companies, Wainer writes, and more are likely to occur going forward.
What companies are targeting in health care
In contrast to the more traditional fee-for-service model, many health care startups are moving toward value-based care, which encourages providers to help prevent illnesses, rather than just treat them.
According to Wainer, UHG, which includes a pharmacy benefit manager, an insurance business, and 60,000 physicians, has made the most progress transitioning to value-based care so far. For example, many of the multi-specialty physician practices UHG has purchased through its medical provider arm Optum Care focus on proactively providing patients home, virtual, and on-site care to help them stay out of the hospital.
In addition, UHG and Walmart last week announced a partnership to provide services and “improve the patient experience” for certain Medicare Advantage enrollees. Through the partnership, UHG will use analytics to help Walmart clinics deliver value-based care to patients.
Aside from value-based care, many companies, including Amazon and CVS, are looking to expand their businesses into primary care. Currently, there is a nationwide shortage of primary care doctors, which has led to worse health outcomes for many Americans.
By providing primary care services directly to consumers, Amazon and other companies are hoping to use the relationship between patients and their providers to sell even more services, such as prescription drug deliveries and more.
Overall, “staying healthy probably will never be the sort of frictionless, one-click experience that Amazon pioneered,” Wainer writes, but the company’s current involvement in the health care industry “is a testament to the fact that there’s a lot of money to be made by fixing America’s broken system.” (Wainer, Wall Street Journal, 9/9)
*Advisory Board is a subsidiary of Optum, a division of UnitedHealth Group. All Advisory Board research, expert perspectives, and recommendations remain independent.
Amazon announced it will shut down Amazon Care—its primary care service sold to employer health plans—by the end of the year. There’s one thing that Amazon’s decision will surely mean: It will continue to be fashionable to mock Amazon.
People may look at this, compare it to Amazon’s Haven misadventure, and say that everyone (including Advisory Board) who speculated that Amazon could succeed in health care is either naïve or delusional.
But there’s more to it.
In looking at what Amazon reportedly said about the challenges facing Amazon Care, we believe that the acquisition of One Medical is the clearest signal yet that Amazon intends to succeed at health care.
The problems with Amazon Care
Amazon Care appears to have struggled to understand the nuances and demands of care delivery, as detailed recently in the Washington Post. Clearly, the tension between expectations for growth and quality were real. This raised questions for us: Was Amazon going to truly “iterate” on its health care capabilities? When it came to care delivery, would Amazon get better, or would it do enough to get by?
Amazon concedes that its product was not comprehensive enough for its employer partners. It’s unclear whether that means it simply wasn’t saving them money, even if employees were using it. At the same time, we wonder how hard it was to persuade employees to embrace Amazon-branded health care or to attract employees to a product centered on virtual and home-based care—or some combination of the two.
Remember: Everyone had to try out telehealth in 2020 because, in many cases, they had no choice. There isn’t any similarly powerful and pervasive force pushing anyone to virtual-first care today. People tend to like virtual visits, but that doesn’t mean that they want to receive all adequately satisfy users or keep care from fragmenting with its mosaic of services, channels, and providers.
What shutting down Amazon Care suggests about Amazon’s health care ambition
Amazon’s willingness to jettison its homegrown but underperforming health care business suggests three things.
One Medical is the centerpiece of Amazon’s health care strategy, not simply one component among many. When viewed this way, the details of the acquisition make more sense than they did four weeks ago. Knowing that a virtual and home-based model wasn’t attractive for employers, we can understand more clearly why Amazon wanted a partner with both in-person and digital health capabilities. Knowing that its own product was struggling, we can see why it was willing to pay a huge premium for One Medical.
Amazon is iterating on its health care capabilities, but it is iterating at an enormous scale. “Fail fast” is axiomatic in technology. It’s usually applied to minimum viable products—applications and services that are quickly built, delivered, and assessed for their ability to meet customer demands and gain traction in the market. Products that don’t meet those demands are replaced as quickly as possible. Obviously, Amazon Care was not a minimum viable product. It was rolled out three years ago, and it offered telehealth services in all 50 states and in-home services in seven markets. But when you look at the pivot Amazon seems to be making from virtual and home-based care with Amazon Care to in-person and virtual with One Medical, it’s hard not to reach for the “fail fast” comparison.
Amazon is a different kind of competitor in health care. We can’t think of another organization that would spend years building out a care delivery enterprise, roll it out in 50 states, and then simply shut it down. We also can’t think of another organization whose alternative care delivery plan is to spend nearly $4 billion on another company. It’s not just the scale and the money—it’s the willingness to throw around those assets that makes Amazon a potentially potent competitor.
There are still enormous execution challenges for Amazon and One Medical. Massive disruption of the industry is not a given, no matter how much money is spent or how many companies are bought and/or fail.
It seems likely that the impact of Amazon on the market will be centered, at least for the immediate future, on the same direct-to-consumer approach that One Medical has taken and at which Amazon is expert in its other lines of business.
That does not mean Amazon can be dismissed as a dilettante or a dabbler in health care. Its mere presence in the market already seems to have sparked a bidding war for Signify Health. Amazon’s continued iteration of its approach to health care demands ongoing attention.
Adult inpatient volumes will recover to pre-pandemic numbers but grow only 2 percent over the next decade, a new report from Sg2 forecasts.
At the same time, adult inpatient days are expected to increase 8 percent and tertiary inpatient days are poised to increase 17 percent, fueled by an increase in chronic conditions.
“While case mix varies by hospital, it is likely this combination of increased inpatient volume, patient complexity and length of stay may require healthcare organizations to rethink service line prioritization, service distribution and investment in care at-home initiatives,” Maddie McDowell, MD, senior principal and medical director of quality and strategy for Sg2, said in a June 7 news release for the report.
Five other key takeaways from Sg2’s forecasts:
1. Outpatient volumes are projected to return to pre-pandemic levels in 2022 and then grow 16 percent through 2032, three percentage points above estimated population growth.
2. Surgical volumes are projected to grow 25 percent at ambulatory surgery centers and 18 percent at hospital outpatient departments and physician offices over the next decade.
3. The pandemic-driven decline in emergency department visits is expected to plateau with a decline in demand projected at -2 percent over the next 10 years.
4. Over the next five years, home care is expected to gain traction, with home evaluation and management visits seeing 19 percent growth, home hospice at 13 percent growth and home physical and occupational therapy at 10 percent growth.
5. Telehealth is expected to resume its climb and by 2032 account for 27 percent of all evaluation and management visits.
UnitedHealth Group’s Optum announced plans to acquire publicly traded, postacute care behemoth LHC Group for $5.4B. The Lafayette, LA-based company, which had $2.2B in revenue last year, operates more than 550 home health locations, 170 hospice sites, and 12 long-term acute care hospitals across 37 states, reaching 60 percent of the country’s Medicare-eligible seniors. LHC also has more than 430 hospital joint venture partners.
The Gist: This deal will greatly expand Optum’s ability toprovide home-based and long-term care, with the goal of moving more care for the insurer’s Medicare Advantage enrollees to lower-cost settings. The acquisition puts Optum’s home healthcare portfolio on par with competitor Humana, which has been the leader in amassing home-based and postacute care assets, and recently moved to take full control of home health provider Kindred at Home. LHC will be part of a growing portfolio of care assets managed by Optum Health, which also includes the company’s owned physician assets.
Success in lowering cost of care will require Optum to integrate referrals and care management across a rapidly expanding portfolio—and ensure its physician base has confidence in these new models of care.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”
Nonprofit payers have used a variety of strategies to address plan affordability throughout the next year, including reducing premiums by as much as 10% in some instances, finds a new report from the Alliance of Community Health Plans.
ACHP’s inaugural Report on Affordability found that when health plans manage premiums, provide enhanced benefits, smooth the way for access and reduce costs for governments and employers, the system – and outcomes – improve.
This is exemplified by some of the strategies employed by ACHP member plans, which largely reduced insurance premiums or held them flat, with some member companies reducing premiums by as much as 10%.
On top of that, every plan added new health benefits, or expanded existing ones, without increasing costs to consumers, the report found. Some of the additional benefits include free vaccines, transportation, hearing aids, reduced insulin costs, nutrition classes and meal services, smoking cessation programs and $0 co-pays for mental health visits.
Roughly three-quarters of ACPH plans moved acute and recovery services out of the hospital setting, which was deemed too expensive in most cases. By establishing hospital-at-home programs and remote patient monitoring, plans have generated significant savings for both consumers and the health system, plus improved consumer satisfaction, results showed.
Meanwhile, about two-thirds of the plans offered price transparency tools meant to allow consumers to make more-informed choices. They included information on inpatient and outpatient services, behavioral health, prescription drugs, lab and imaging services and other fees, and many provided options for several locations and virtual care, a move intended to reduce travel costs.
Priority Health’s cost estimator has tallied $13.8 million in shared savings and paid out roughly $4.1 million in rewards to members.
In a bid to improve access, all plans expanded telehealth offerings, smoothing access to mental healthcare as well as to specialties such as Medication Assisted Treatment, physical and occupational therapy, medication management, speech therapy and dialysis. Most eliminated co-pays and cost sharing.
WHAT’S THE IMPACT?
In the last year, ACHP members expanded the hospital-at-home care model, attempting to offer more efficient ways to provide acute and recovery care as well as care management in a home setting. The expansion of virtual care, complete with remote monitoring and social support, reduces the risk of infection, keeps patients comfortable at home and alleviates inpatient hospital bed shortages, according to the report.
For example, SelectHealth and its owner system, Utah-based Intermountain Healthcare, launched Connect Care Pro, a virtual hospital meant to enable access for patients in remote locations. The online, digital program connects more than 500 caregivers across the Intermountain system, enabling patients to receive both basic medical and specialty care without making a long journey, including by helicopter.
Presbyterian Health of New Mexico’s Complete Care, on the other hand, is a wrap-around program that combines primary, urgent and home care for patients with complex medical needs, including those with functional decline and at risk of needing long-term institutional care. Patients receive and manage their care from home, 24/7, including acute and palliative care, house-call and same-day visits, as well as medication management. In addition, care coordinators and social workers manage social needs, including transportation and food insecurity.
And the Home Care Recovery program from Wisconsin’s Security Health Plan and Marshfield Clinic Health System brings the elements of acute inpatient recovery to a patient’s home, eliminating fixed-cost allocations associated with traditional hospital-level care and reducing post-acute utilization and readmissions for 150 traditional inpatient conditions such as congestive heart failure, pneumonia and asthma.
THE LARGER TREND
A 2016 report from the Centers for Medicare and Medicaid Services found that nonprofit organizations and health plans tend to receive higher star ratings than their for-profit counterparts.
For Medicare Part Ds, about 70% of the nonprofit contracts received four or more stars compared to 39% of the for-profit MA-Part-Ds. Similarly, roughly 63% of nonprofit prescription drug plans received four or more stars, compared to 24% of the for-profit PDPs.
The Democrats’ reconciliation bill includes several major health care pieces backed by different lawmakers and advocates, setting up a precarious game of policy Jenga if the massive measure needs to be scaled back.
Between the lines:Health care may be a priority for Democrats. But that doesn’t mean each member values every issue equally.
Why it matters: As the party continues to hash out the overall price tag of its giant reconciliation bill, it’s worth gaming out which policies are on the chopping block — and which could potentially take the entire reconciliation bill down with them.
There are clear winners of each pillar of Democrat’s health plan:
Seniors benefit from expanding Medicare to cover dental, vision and hearing benefits.
Low-income people — primarily in the South and disproportionately people of color — in non-expansion states benefit if the Medicaid gap is closed, giving them access to health coverage.
Affordable Care Act marketplace enrollees benefit if the increased subsidy assistance that Democrats enacted earlier this year is extended or made permanent.
Elderly and Americans with disabilities benefit from an expansion of their home-based care options, and their caretakers benefit from a pay bump.
Seniors — and potentially anyone facing high drug costs — benefit if Medicare is given the authority to negotiate drug prices, although the drug industry argues it will lead to fewer new drugs.
Yes, but:Each of these groups face real problems with health care access and affordability. But when there’s a limited amount of money on the table — which there is — even sympathetic groups can get left in the dust.
Each policy measure, however, also has powerful political advocates. And when Democrats have a razor-thin margin in both the House and the Senate, every member has a lot of power.
Seniors are disproportionately powerful on their own, due to their voting patterns. But expanding what Medicare covers is extremely important to progressives — including Sen. Bernie Sanders.
Closing the Medicaid gap is being framed as a racial justice issue, given that it disproportionately benefits people of color. And although many Democrats hail from expansion states — particularly in the Senate — some very powerful ones represent non-expansion states.
These members include Sen. Raphael Warnock, who represents Georgia and is up for re-election next year in an extremely competitive seat, and Rep. Jim Clyburn, who arguably is responsible for President Biden winning the 2020 primary.
The enhanced ACA subsidies are scheduled to expire right before next years’ midterm elections. Democrats’ hold on the House is incredibly shaky already, making extending the extra help a political no-brainer.
Expanding home-based care options was one of the only health care components of Biden’s original framework for this package. But aside from the president’s interest in the issue, unions care a lot about it as their members stand to gain a pay raise — and Democrats care a lot about what unions care about.
And finally, giving Medicare the power to negotiate drug prices has the most powerful opponents, theoretically making it vulnerable to the chopping block. But it also polls very highly, and perhaps even more importantly, produces enough government savings to help pay for these other health care policies.
The bottom line: “From a political perspective, none of these health care proposals seem very expendable,” said KFF’s Larry Levitt.
Most — if not all of them — can be scaled to save money.
But there are also powerful constituencies for the other components of the bill that address issues like child care and climate change, meaning these health care measures aren’t only competing against one another.
And, Levitt points out, “there’s always a difference between members of Congress staking out positions and being willing to go to nuclear war over them.”
Hospitals lost 5,800 jobs in April, marking the fourth month of job loss this year, according to the latest jobs report from the U.S. Bureau of Labor Statistics.
Overall, healthcare lost 4,100 jobs last month — compared to 11,500 jobs added in March — and employment in the industry is down by 542,000 since February 2020.
Within ambulatory healthcare services, dentist offices saw 3,700 added jobs; physician offices saw 11,300 job gains; and home healthcare services lost 6,700 jobs in April.
Nursing and residential care facilities lost 19,500 jobs last month, compared to 3,200 jobs lost the month prior.
The U.S. gained 266,000 in April after gaining 916,000 jobs in March. The unemployment rate was 6.1 percent last month, compared to 6 percent in March.