The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
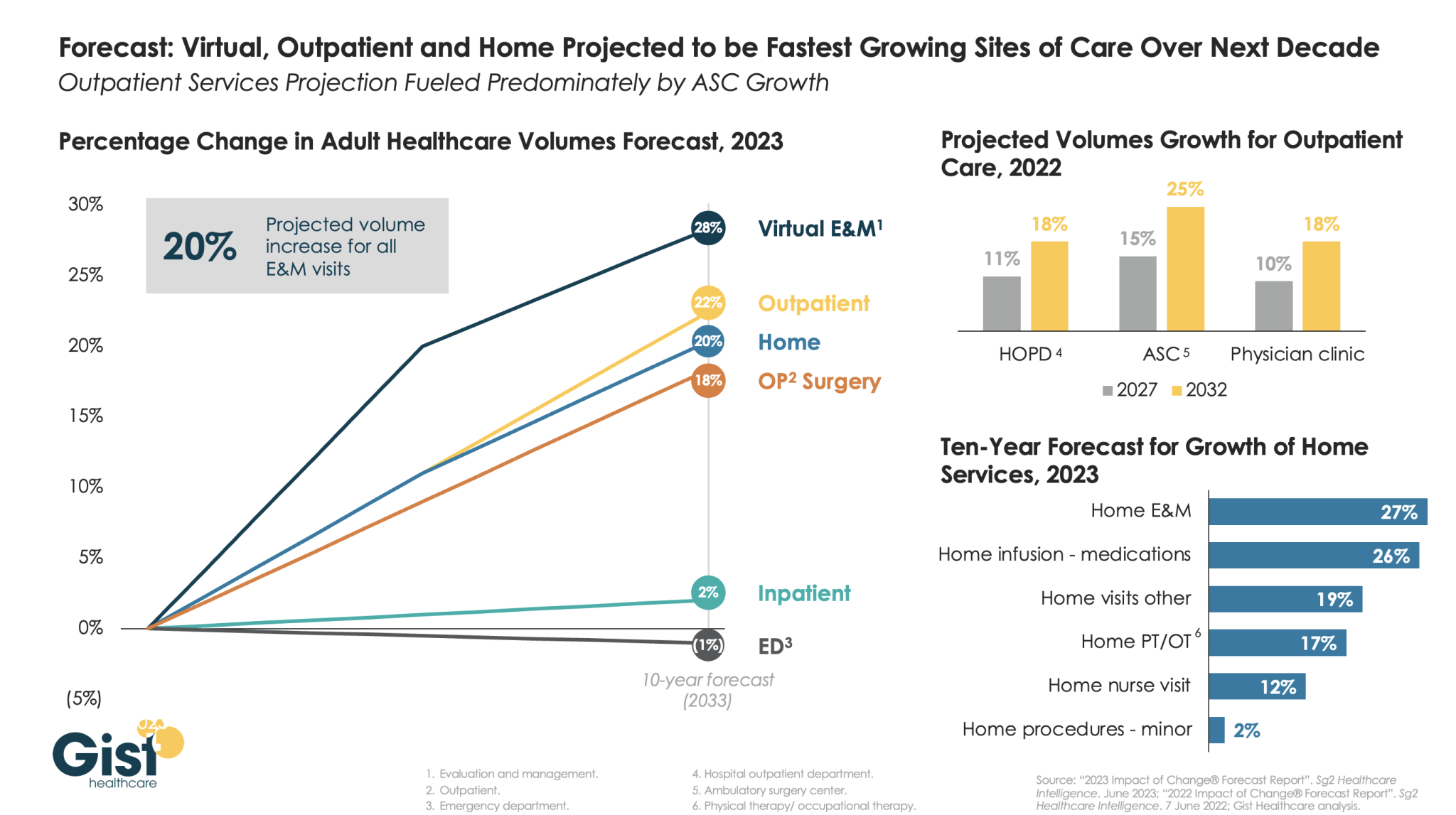
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
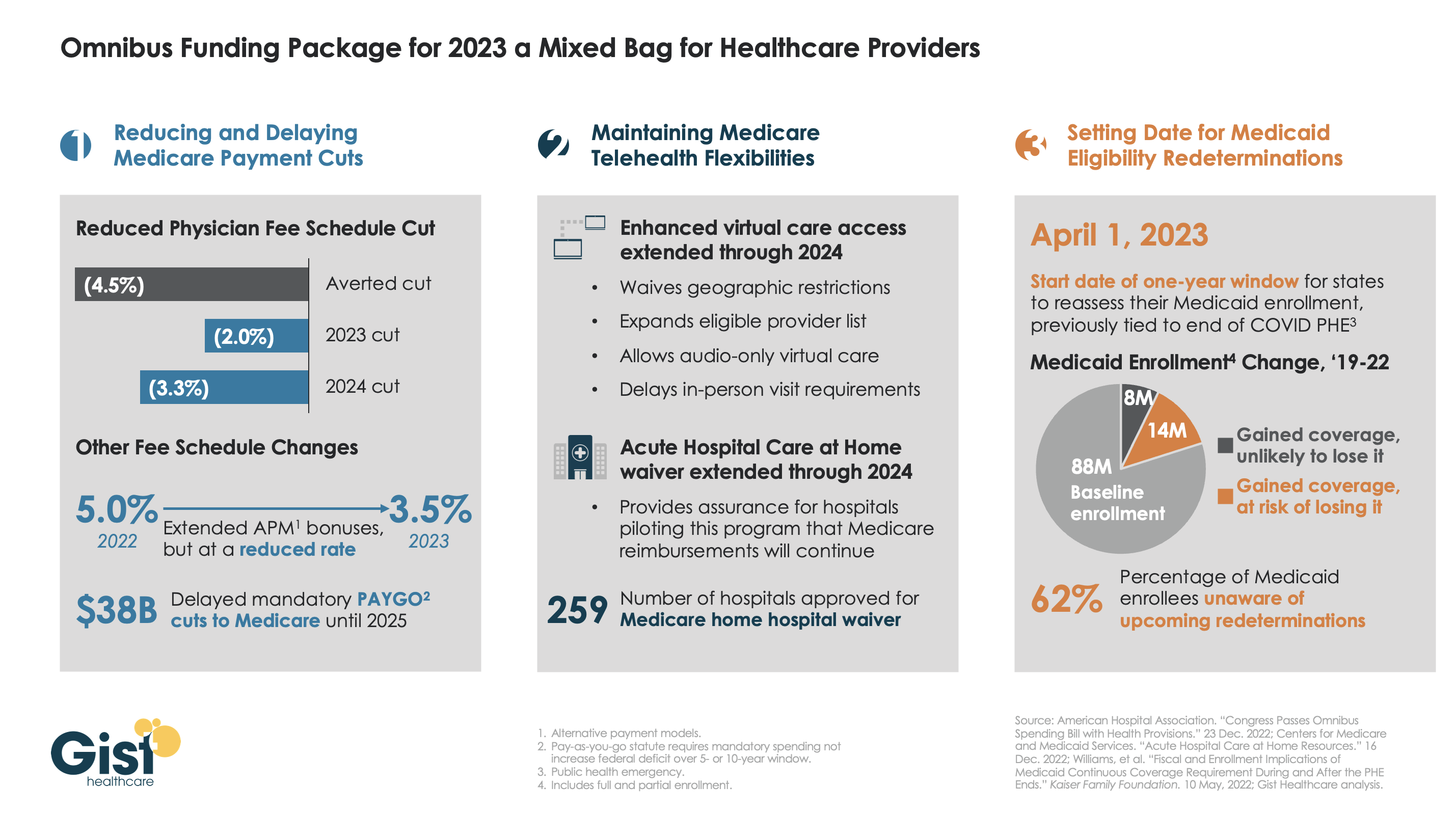
Late last week, President Biden signed a $1.7T spending package to fund the federal government through next September. While around half the funds are dedicated to defense, some important healthcare items made it into the bill, including a reduction in planned Medicare physician pay cuts and a two-year postponement of the $38B Medicare spending cut required by the PAYGO sequester.
The law also decoupled several measures from the end of the federal COVID public health emergency (PHE), setting April 1st as the start date for states to begin Medicaid eligibility redeterminations, and extending Medicare’s telehealth flexibilities and the Acute Hospital Care at Home waiver program through the end of 2024. For more details on these changes, see our graphic below.
The Gist: Medical groups were hoping for more of a reprieve from the Medicare physician fee schedule cuts, but Congress proved unwilling to address concerns over rising practice costs. We’re relieved that Medicare’s new telehealth and hospital at home policies will continue beyond the PHE, given the early interest we’ve seen from the provider community in embracing these new, more consumer-friendly care models.
Once the new Congress finally gets underway, we’re expecting this to be an uneventful two years for federal healthcare legislation, with the emphasis of health policy likely to shift toward states, federal agency rulemaking, and judicial activity.
Amazon and several other major companies have made numerous attempts to “disrupt” health care over the years without much success. But new acquisitions in primary care, home health care, and more may allow them to more successfully expand into the industry, David Wainer writes for the Wall Street Journal.
Competition heats up in the health care industry
According to Wainer, the United States spends a greater proportion of its economy on medical services than any other developed nation, making health care “too big of an opportunity to ignore” for many companies, including those in technology, retail, and more.
For example, Amazon has launched several forays into health care in recent years, although not all of them have been successful. Some of these health care efforts include its now defunct partnership with Berkshire Hathaway and JPMorgan Chase, as well as Amazon Care, the company’s primary care service that will shut down at the end of the year.
Amazon has also acquired several smaller health care companies in an effort to expand its reach. In 2018, Amazon purchased PillPack for $1 billion as a way to expand its online pharmacy business. Similarly, Amazon in July reached an agreement to acquireOne Medical, a primary care company, for roughly $3.9 billion.
Several other companies, including retailers like Walmart and Walgreens and large insurers like UnitedHealth Group* (UHG) and CVS Health‘s Aetna, are also looking to expand their health care offerings. In fact, CVS announced last week that it had purchased home health care company Signify Health for roughly $8 billion—beating out several other competitors.
So far, “[s]hifting social attitudes and market conditions have helped fuel the wave” of health care acquisitions from major companies, Wainer writes, and more are likely to occur going forward.
What companies are targeting in health care
In contrast to the more traditional fee-for-service model, many health care startups are moving toward value-based care, which encourages providers to help prevent illnesses, rather than just treat them.
According to Wainer, UHG, which includes a pharmacy benefit manager, an insurance business, and 60,000 physicians, has made the most progress transitioning to value-based care so far. For example, many of the multi-specialty physician practices UHG has purchased through its medical provider arm Optum Care focus on proactively providing patients home, virtual, and on-site care to help them stay out of the hospital.
In addition, UHG and Walmart last week announced a partnership to provide services and “improve the patient experience” for certain Medicare Advantage enrollees. Through the partnership, UHG will use analytics to help Walmart clinics deliver value-based care to patients.
Aside from value-based care, many companies, including Amazon and CVS, are looking to expand their businesses into primary care. Currently, there is a nationwide shortage of primary care doctors, which has led to worse health outcomes for many Americans.
By providing primary care services directly to consumers, Amazon and other companies are hoping to use the relationship between patients and their providers to sell even more services, such as prescription drug deliveries and more.
Overall, “staying healthy probably will never be the sort of frictionless, one-click experience that Amazon pioneered,” Wainer writes, but the company’s current involvement in the health care industry “is a testament to the fact that there’s a lot of money to be made by fixing America’s broken system.” (Wainer, Wall Street Journal, 9/9)
*Advisory Board is a subsidiary of Optum, a division of UnitedHealth Group. All Advisory Board research, expert perspectives, and recommendations remain independent.
A Massachusetts nurse has pleaded guilty in federal court in Boston in connection with a $100 million healthcare fraud scheme, the Justice Department announced Sept. 13.
Winnie Waruru, a licensed practical nurse, pleaded guilty Sept. 8 to conspiracy to commit healthcare fraud, healthcare fraud – aiding and abetting, conspiracy to pay and receive kickbacks, making false statements and making a false statement in a healthcare matter.
Ms. Waruru was employed by Chelmsford, Mass.-based Arbor Homecare Service. She was charged in February 2021 alongside Faith Newton, who was part owner and operator of the home healthcare company from 2013 to 2017. Ms. Newton has pleaded not guilty, according to the Justice Department.
Prosecutors allege that the duo used Arbor to defraud MassHealth and Medicare of at least $100 million by committing fraud and paying kickbacks to get referrals. Specifically, prosecutors allege that Arbor billed payers for home health services that were never provided or weren’t medically necessary. Arbor billed MassHealth for Waruru’s skilled nursing visits, many of which she did not perform, according to the Justice Department.
Nothing kills the momentum and excitement of race day more than the yellow flag and deployed safety car. Unsafe track conditions, usually caused by an accident, debris on the track or a stopped vehicle, can cause the marshals to slow down the race. Momentum moderates and adrenaline wanes. Drivers are forbidden from overtaking, and victory is temporarily out of sight for all but the lead car. As I watched the Indy 500, 24 Hours at Le Mans and a handful of Formula One grand prix over the last several weeks, it struck me that postacute sector M&A (home health, hospice, Medicaid PCS, pediatric PDN/therapy) is currently racing under yellow flag conditions. Temporary, but nonetheless frustrating for all constituents involved.
The post-acute sector’s two record setting years in terms of transaction activity, valuation multiples and quality of companies acquired, 2020 and 2021, now appear to be in the rearview mirror. In their stead is a sluggish 2022, with companies staying in their lanes, focused inwardly on operations and trying to regain levels of growth and profitability of prior years. It should come as no surprise that sector activity has slowed: (i) the supply of actionable platforms is materially lower than in the prior two years; (ii) the COVID spawned labor market continues to create one of the most challenging operating environments in recent memory; (iii) home health reimbursement faces a potentially challenging outlook when the CY 2023 HH PPS rule is finalized in the Fall; and (iv) buyers are less willing to give credit for COVID-related EBITDA adjustments.
Lower Inventory of Actionable Platforms Many of the most actionable privately-held and sponsor-owned platforms transacted at a kinetic pace in 2019, 2020 and 2021. As a result, the number of available platforms is relatively low, and the sector is currently in a holding pattern, where businesses are (i) focused on operating in a challenging environment, (ii) too early in their hold period, or (iii) waiting for financial performance to improve, before coming to market. There is a large and growing backlog of businesses that we expect to come to market when overall conditions improve, potentially as early as Q4 2022. But in the meantime, the market is generally in wait and see mode.
Labor Market’s Impact on Performance Q4 2021 was one of the most challenging quarters for post-acute operators, particularly hospice, as the Omicron variant wreaked havoc on staffing and admissions volumes. Despite strong referral volumes and demand for post-acute services, the inability to
sufficiently hire and retain clinical staff has had a material impact on monthly sequential growth and TTM performance. For many, Q1 2022 was only marginally better, and for some, Q2 2022 continues to present challenges, although, anecdotally, the clinical labor market appears to be improving and may even accelerate due to the looming recession. As a result, companies are deciding, or being forced, to delay sale processes as they attempt to replace poor financial performance in Q4 2021 and Q1 2022 with improved 2H 2022 growth and profitability.
Pending CY 2023 Home Health PPS Rule Based on the proposed rule released last week, CMS estimates that Medicare payments to home health agencies in CY 2023 would decrease in the aggregate by -4.2%, or -$810 million compared to CY 2022. Without getting too technical and comprehensive, this decrease reflects the effects of the proposed 2.9% home health payment update percentage ($560 million increase), an estimated 6.9% decrease that reflects the effects of the proposed prospective, permanent behavioral assumption adjustment of -7.69% ($1.33 billion decrease), and an estimated 0.2% decrease that reflects the effects of a proposed update to the fixed-dollar loss ratio (FDL) used in determining outlier payments ($40 million decrease). Prospective home health sellers will most likely wait for better clarity on the final rule before coming to market.
Market Push Back on COVID-Related EBITDA Adjustments Buyers and lenders have materially increased their scrutiny of COVID-related volume adjustments to EBITDA. Early in the pandemic, the market was quite willing to pay sellers for normalized volumes and financial performance, as if “COVID had not happened.” 27 months later, the market is taking a harder line. “What if” earnings credit is no longer being given wholesale. The market has taken the position that labor staffing challenges and higher labor wage expense are here to stay (for now), and, unless a seller has clearly demonstrated a trend to the contrary, little to no valuation / leverage credit will be given for such adjustments. As a result, prospective sellers must increasingly rely on actual earnings to ensure the achievement of valuation expectations.
Returning to our racing analogy, post-acute sector M&A is currently under a yellow flag. And while yellow flag conditions produce little to no racing action, and can last for many laps, they are still only temporary. Drivers and their teams can use the time to their advantage – to “box” or “pit” in order to change tires, refuel or tweak the car – so that they are ready to drop the hammer once the yellow flag is lifted. This is exactly what the higher quality post-acute platforms are doing. Some of the most exciting action in a race comes once the safety car exits the track and green flag racing resumes. Given the strong near- and long-term demographic and sector trends supporting the post-acute sector, and the almost unlimited demand for high quality post-acute platforms, there is little doubt that M&A activity will resume with a vengeance.
Adult inpatient volumes will recover to pre-pandemic numbers but grow only 2 percent over the next decade, a new report from Sg2 forecasts.
At the same time, adult inpatient days are expected to increase 8 percent and tertiary inpatient days are poised to increase 17 percent, fueled by an increase in chronic conditions.
“While case mix varies by hospital, it is likely this combination of increased inpatient volume, patient complexity and length of stay may require healthcare organizations to rethink service line prioritization, service distribution and investment in care at-home initiatives,” Maddie McDowell, MD, senior principal and medical director of quality and strategy for Sg2, said in a June 7 news release for the report.
Five other key takeaways from Sg2’s forecasts:
1. Outpatient volumes are projected to return to pre-pandemic levels in 2022 and then grow 16 percent through 2032, three percentage points above estimated population growth.
2. Surgical volumes are projected to grow 25 percent at ambulatory surgery centers and 18 percent at hospital outpatient departments and physician offices over the next decade.
3. The pandemic-driven decline in emergency department visits is expected to plateau with a decline in demand projected at -2 percent over the next 10 years.
4. Over the next five years, home care is expected to gain traction, with home evaluation and management visits seeing 19 percent growth, home hospice at 13 percent growth and home physical and occupational therapy at 10 percent growth.
5. Telehealth is expected to resume its climb and by 2032 account for 27 percent of all evaluation and management visits.
The Justice Department has intervened in a whistleblower lawsuit accusing former executives of San Antonio-based Merida Health Care Group of violating the False Claims Act, according to Law360.
The Justice Department is intervening in the action, which dates back to 2015, alleging the former executives submitted more than $120 million in false claims to Medicare for medically unnecessary home health services and hospice care. The Justice Department is also adding Merida Health Group’s former CEO Henry McInnis to the complaint, according to the report.
The Justice Department alleges Mr. McInnis and Rodney Mesquias, the former owner of Merida Health Care Group, violated the False Claims Act, and the government is also seeking damages under the common law and equitable theories of fraud and payment by mistake, according to court documents filed April 7 in the U.S. District Court for the Southern District of Texas.
Mr. McInnis was sentenced to 15 years in prison in February 2021 for his role in a healthcare fraud and money laundering scheme. Mr. Mesquias was sentenced to 20 years in prison in late 2020.
UnitedHealth Group’s Optum announced plans to acquire publicly traded, postacute care behemoth LHC Group for $5.4B. The Lafayette, LA-based company, which had $2.2B in revenue last year, operates more than 550 home health locations, 170 hospice sites, and 12 long-term acute care hospitals across 37 states, reaching 60 percent of the country’s Medicare-eligible seniors. LHC also has more than 430 hospital joint venture partners.
The Gist: This deal will greatly expand Optum’s ability toprovide home-based and long-term care, with the goal of moving more care for the insurer’s Medicare Advantage enrollees to lower-cost settings. The acquisition puts Optum’s home healthcare portfolio on par with competitor Humana, which has been the leader in amassing home-based and postacute care assets, and recently moved to take full control of home health provider Kindred at Home. LHC will be part of a growing portfolio of care assets managed by Optum Health, which also includes the company’s owned physician assets.
Success in lowering cost of care will require Optum to integrate referrals and care management across a rapidly expanding portfolio—and ensure its physician base has confidence in these new models of care.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”
After months of negotiations, House Democrats on Friday passed their version of the Build Back Better bill—an expansive $1.7 trillion package that contains some of the largest health reforms since the Affordable Care Act’s passage in 2010.
While the overall scope of the bill is roughly half the size of President Biden’s original $3 trillion proposal, many of Democrats’ key health care provisions made it in, albeit with some modifications. What’s more, the Congressional Budget Office projected that while the overall bill would add $367 billion to the deficit over the 10 year period, the health care provisions would all be largely paid for by provisions aimed at lowering drug prices.
Below, I round up the five biggest health care changes included in the House bill.
The House bill leverages the ACA’s exchanges and federal tax credits to expand access to coverage in two ways. First, the bill would extend the American Rescue Plan’s enhanced ACA tax credits through 2025. The enhanced tax credits, which are currently slated to expire in 2023, fully subsidize coverage for people with annual incomes up to 150% of the federal poverty level (FPL) and have enabled people above 400% FPL to qualify for subsidies and capped their premium costs at 8.5% of their incomes.
While Democrats had originally proposed to permanently expand those subsidies, they ultimately had to scale back this—and other proposals—to ensure they could cover the costs. But as we’ve seen in the past, it is much harder to take away an existing benefit or subsidy than it is to create a new one—so while the current bill was able to cover the cost of the health care provisions by making them temporary, lawmakers will have to revisit the tax credits before 2025 and find new money to either further extend them or permanently authorize them. This is one of several health care provisions we could see the Senate take a closer week at in the coming weeks.
Second, the House bill takes aim at the so-called Medicaid coverage gap. The bill would enable residents below 138% FPL who live in states that have not expanded their Medicaid programs to qualify for fully subsidized exchange plans through 2025. While an earlier version of the House bill included language for a new federal Medicaid program covering those below 138% FPL who live in non-expansion states to begin in 2025, the final House bill contains no such program.
Instead, the bill aims to encourage non-expansion states to expand their Medicaid programs by reducing their Disproportionate Share Hospital (DSH) payments by 12.5% beginning in 2023—a significant cut that the American Hospital Association (AHA) estimates would reduce DSH payments in those states by $2.2 billion over five years and $4.7 billion over 10 years. At the same time, expansion states would see their federal match for spending on the Medicaid expansion population rise from 90% to 93% from 2023 through 2025.
While the AHA and others are pushing back against the proposed DSH payment cuts—the move addresses the moral hazard component that critics raised about earlier versions. It no longer rewards holdout states for not expanding their programs—effectively punishing those who did and are now on the hook for 10% of their expansion population’s costs. It’s a clever move, and one we’ll be watching to see if it survives the Senate.
2. New Medicare benefits.
The House bill adds a hearing benefit to Medicare beginning in 2023. The hearing benefits would cover hearing aids and aural rehabilitation, among other services. While this is certainly a win for many Medicare beneficiaries who do not have or cannot afford private Medicare Advantage plans, this is significantly scaled back from the original proposal to add hearing, as well as dental and vision benefits.
However, given that Sen. Bernie Sanders (I-Vt.) has named Medicare benefit expansions as one of his top priorities, it’s possible we could see this topic revisited in the Senate. But any meaningful change would mean Democrats need to find more money to cover the costs—and so far, that has proved challenging.
3. Medicaid home and community care.
The House bill allocates $150 billion for home- and community-based care. The funding would be used to help increase home care provider reimbursement rates and help states bolster home- and community-based care infrastructure.
While the funding is down from an original proposal of $400 billion, the Biden administration—and the Covid-19 pandemic—have made it clear that home-based health care will continue to grow and be a key player in the U.S. health care delivery system. Providers looking at their offerings should keep an eye on how states are investing these funds and building out home-based health care delivery in their areas.
4. Lowering the costs of prescription drugs.
Democrats scored a huge win in the House bill, and that is securing Medicare authority—albeit narrower authority than they sought—to negotiate prices for some of the highest-priced Part B or Part D drugs. Under the bill, HHS would be able to select 10 drugs to negotiation in 2025, up to 15 drugs in 2026 and 2027, and then up to 20 drugs per year in 2028. To be eligible for negotiation, a drug could no longer be subject to market exclusivity.
Drug manufacturers that do not negotiate eligible drug prices could be subject to an excise tax. This was perhaps one of the most contentious provisions debated in the health care portions of this bill. Democrats for years have been seeking to give Medicare drug pricing authority, but intense lobbying and Republican—and some Democrat—objections have kept this proposal on the shelf. While it’s not the first time the House has passed a bill with drug price negotiation—it is the first time we are in a place where the Senate could reasonably pass either this or a modified version of the proposal.
The bill also would redesign the Medicare Part D benefit to create an annual cap of $2,000 on seniors’ out-of-pocket drug costs, and impose an inflation rebate on drug manufacturers’ whose drug prices rise faster than inflation (based on 2021) in a given year.
5. Other notable provisions.
The House bill also includes provisions to permanently fund CHIP, bolster the country’s pandemic preparedness and response, and bolster the health care workforce through new training and workforce programs, the nation’s first permanent federal paid family and medical leave program, investments in childcare, and more.
What’s next?
While the health care provisions in the House bill are notable, it’s important to remember that this is not the end of the road. The House bill now goes to the Senate, where the Senate parliamentarian will check provisions against the Byrd rule—a Senate rule requiring reconciliation bills to meet certain budgetary requirements.
Democrats also will enter a new round of negotiations, and industry groups—including PhRMA and AHA—are expected to launch a new round of lobbying. PhRMA objects to the bill’s drug price negotiation provision and AHA is fighting the provision to reduce DSH payments in non-Medicaid expansion states by 12.5%. Any Senate-passed reconciliation bill will need to go back to the House for final approval before it can go to Biden’s desk.
But this is not the only thing on lawmakers’ plates in December. Members of Congress also face several other deadlines, including addressing looming physician payment cuts and passing end of the year spending bills. The short-version is, while there’s a lot to learn from the House-passed bill, it’s possible the Senate version could look very different—and it may take several weeks before we see that bill take shape.