I fell down a flight of stairs at 4 a.m. last Wednesday.
It was totally my fault.
Since then, I have used hospital emergency departments in 2 states, a freestanding imaging center and a large orthopedic clinic and I’m just getting started. Six days in, I’m lucky to be alive but I still don’t know the extent of my injuries, my chances of playing golf again nor what I will end up spending on this ordeal. But nonetheless, it could have been worse. I’m alive.
Surprises in all aspects of life are never anticipated fully and always disruptive. This one, for me, is no exception. I am frustrated by my accident and uncomfortable with sudden dependence on others to help navigate my recovery.
But this is also a teachable moment., As I am navigating through this ordeal, I find myself reflecting on the system—how it works or doesn’t—based on what I am experiencing as a patient.
Here’s my top three observations thus far:
The patient experience is defined by the support team:
The heroes in every setting I’ve used are the clerks, technicians, nurses and support staff who’ve made the experiences tolerable and/or reassuring. Patients like me are scared. Emotional support is key: some of that is defined by standard operating procedures and checklists but, in other settings, it’s cultural. Genuineness, empathy and personal attention is easy to gauge when pain is a factor. By the time physicians are on the scene, reassurance or fear is already in play. Care teams include not just those who provide hands-on care, but the administrative clerks and processes that either heighten patient anxiety or lessen fear. The health and well-being of the entire workforce—not just those who deliver hands-on care—matters. And it’s easy to see distinctions between organizations that embrace that notion and those that don’t.
Navigation is no-man’s land:
The provider organizations I’ve used thus far have 3 different owners and 3 different EHR systems. Each offers written counsel about ‘patient responsibility’ and each provides a list of do’s and don’ts for each phase of the process. Sharing test results across the 3 provider organizations is near impossible and coordination of care management is problematic unless all parties agree and protocols facilitating sharing in place. Perhaps because it was a holiday weekend, perhaps because staffing levels were less than usual, or perhaps because the organizations are fierce competitors, navigating the system has been unusually difficult. Navigating the system in an emergency is essential to optimal outcomes: processes to facilitate patient navigation are not in place.
What’s clear is hospitals, clinics and imaging facilities on different EHR systems don’t exchange data willingly or proactively. And, at every step, getting approvals from insurers a major step in the processes of care.
Price transparency is a non-issue in emergency care:
The services I am receiving include some that are “shoppable” and many that aren’t. I have no idea what I will end up spending, my out-of-pocket obligations nor what’s to come. I know among the mandatory forms I signed in advance of treatment in all 3 sites were consent forms for treatment and my obligation for payment. But in an emergency, it’s moot: there’s no way to know what my costs will be or my out-of-pocket responsibility. So, the hospital and insurer price transparency rules (2021, 2022) might elevate awareness of price distinctions across settings of care but their potential to bend the cost curve is still suspect.
Patients, like me, have to fend for ourselves. I am a number. Last Wednesday, waiting 85 minutes to be seen was frightening and frustrating though comparatively fast. Duplicative testing, insurer approvals, work-shift transitions, bedside manners, team morale, and sterile care settings seem the norm more than exception.
So, for me, the practical takeaways thus far are these:
Don’t have an accident on a holiday weekend.
Don’t expect front desk and check-out personnel to engage or answer questions. They’re busy.
Don’t expect to start or leave without paying something or agreeing you will.
Don’t expect waiting areas and exam rooms to be warm or inviting.
Do have great neighbors and family members who can help. For me, Joe, Jordan, Erin and Rhonda have been there.
The health system is complicated and relationships between its major players are tense. Not surprisingly and for many legitimate reasons, my experience, thus far, is the norm. We can do better.
Paul
P.S. As I have reflected on the event last week, I found myself recalling the numerous times I called on “my doctors” to help my navigation of the system. They include Charles Hawes (deceased), Ben Womack, Ben Heavrin, David Maron, David Schoenfeld and Blake Garside. And, in the same context, the huge respect I have for clinicians I’ve known through Vanderbilt and Ohio State like Steve Gabbe and Andy Spickard who personify the best the medical profession has to offer. Thanks gentlemen. What you do matters beyond diagnoses and treatments. Who you are speaks volumes about the heart and soul of this industry now struggling to re-discover its purpose.
Prices for non-trauma inpatient admissions were 4.4 percent higher at trauma center hospitals than at hospitals without a trauma designation.
Hospitals designated as trauma centers charged higher prices for non-trauma inpatient admissions and emergency department visits compared to non-trauma center hospitals, a Health Affairs study found.
Hospital prices are the largest driver of rising healthcare spending in the commercial market and are often influenced by the structure of hospital markets. Trauma centers are a critical aspect of the hospital market as they are highly regulated and endowed by regulators with monopoly power over trauma patients in their service areas.
In most states, regulations are designed to encourage the entry of new trauma centers in areas that do not already have one and restrict new entry into areas that already have a trauma center. Additional regulations often require all trauma patients within an area to be transported or transferred to the designated hospital serving the area.
These restrictions create local monopolies for hospitals that are designated as trauma centers. Those in favor of the regulations argue that the monopolies are necessary to ensure each trauma center has sufficient volume to support high-quality and low-cost care. However, this structure could allow hospitals with market power over trauma services to raise prices for non-trauma services.
Researchers used claims data from 2011 to 2018 to assess whether hospitals designated as trauma centers use their market power for trauma services to receive above-market rates for non-trauma services. The sample included 2,000 hospitals with more than two million inpatient admissions and ten million emergency department visits over the study period.
The share of hospitals included in the sample serving as trauma centers increased from 21 percent in 2012 to 28 percent in 2018, resulting in a net addition of 138 trauma centers. The share of non-trauma inpatient admissions and emergency department visits at hospitals serving as trauma centers also increased between 2012 and 2018.
Hospitals serving as trauma centers every year from 2012 to 2018 were categorized as an always trauma center. Opened trauma centers were those not serving as a trauma center in 2012 but serving as one by 2018. Hospitals serving as a trauma center in 2012 but not in 2018 were closed trauma centers, and hospitals that did not serve as a trauma center at all during the study period were called “never trauma centers.”
The average price for non-trauma inpatient admissions among all hospitals was $21,112. Always trauma center hospitals had a higher average price of $22,568 per inpatient admission. The average price per admission was $22,097 at opened centers, $20,589 at closed centers, and $19,769 at never centers. Emergency department prices were similar, with always and opened center hospitals having higher prices than closed and never trauma center facilities.
Always trauma center hospitals were generally larger compared to the other hospital types and were more likely to be in more concentrated hospital markets. The average new injury severity score among emergency department visits in never trauma center hospitals was smaller compared to scores at other hospitals. The average MS-DRG weight for always trauma center hospitals was 1.61 compared to 1.54 for opened and never trauma center hospitals.
Holding these patient and hospital characteristics constant, prices for non-trauma inpatient admissions were 4.4 percent higher in hospitals with trauma center designation than at non-trauma center hospitals. Prices for non-trauma emergency department visits were 5.2 percent higher in trauma center hospitals.
“The results presented here provide an example of an important challenge: How to ensure access to specialized services and protect public health while also accounting for and possibly managing the effects of concomitant market failure,” researchers wrote.
“Our findings provide empirical support for the notion that provider market power in one area can be leveraged to affect prices in other areas.”
The No Surprises Act limits the amounts that hospitals can charge to out-of-network patients for emergency services, including trauma services. This may help limit trauma emergency cross-service leverage pricing, researchers said.
Physician staffing firm Envision Healthcare filed for Chapter 11 bankruptcy this week, but will “continue operating its business as usual” so that the company can “provide patients with the high-quality care they require.”
Envision Healthcare files for Chapter 11 bankruptcy
On Monday, Envision Healthcare filed for Chapter 11 bankruptcy in the U.S. Bankruptcy Court for the Southern District of Texas. Following the filing, all of the company’s debt — except for a revolving credit facility for working capital — will be cancelled, totaling around $5.6 billion.
In a news release, Envision said several events have placed significant pressure on its finances since it was acquired by private equity (PE) firm KKR for $10 billion in 2018.
“The lingering impacts from COVID-19 on volume and labor costs, the delays resulting from tactics and recalcitrance by Envision’s largest insurance payors, and the ongoing regulatory uncertainty caused by the flawed implementation of the No Surprises Act have proven too much,” said Paul Keglevic, Envision’s chief restructuring officer.
Throughout the pandemic, healthcare staffing firms struggled to find enough workers to meet patient demand, especially in the highly competitive contract labor market, Modern Healthcare reports.
While Envision said it filed for bankruptcy because it is not generating enough revenue to cover its expenses and debt, it currently has $665 million of cash in the bank. According to the filing, the company expects those funds to help it exit bankruptcy faster.
“The decision to file these chapter 11 cases now, while the debtors have ample cash on hand, will ensure that the company can continue to provide patients with the high-quality care they require,” Keglevic said in the filings.
The company has entered a Restructuring Support Agreement (RSA), with plans to operate normally during the restructuring. Pending court approval, Envision said it will tap into cash collateral from ongoing operations to cover costs, “including supplier obligations and employee wages, salaries, and benefits during the restructuring process.”
“This will enable the company to continue operating its business as usual throughout the process and provide support to critical partners, including clinicians, hospitals, vendors and suppliers,” the company said.
Under the RSA, the company will divide its primary businesses, AMSURG and Envision Physician Services, which will be owned by their respective lenders.
Does Envision’s bankruptcy spell trouble for other PE investments?
Envision isn’t like other medical group PE investments
As we discussed in a previous expert insight, PE investments in physician practices aren’t a monolith. Many different types of medical groups receive investments, and PE firms have a range of healthcare sector experience and business practices.
Envision is an example of an outlier in all of these areas. First, their physician services are all hospital-based, with a heavy emphasis on emergency medicine — this contrasts with the predominant wave of physician practice investment in ambulatory practices. KKR only has one other physician practice investment, and their healthcare portfolio is rather limited.
Most importantly, Envision’s business model was reliant on exploiting questionable business practices and loopholes, which were heavily impacted by the No Surprises Act.
So, this bankruptcy isn’t an indictment of PE investment in physician groups. It just shows that healthcare organizations are not immune to being caught on their bad business practices — though PE, which is already struggling in the court of public opinion, won’t be helped by Envision’s demise.
What Envision’s bankruptcy means
Envision’s bankruptcy shines a light on trends we’ve been watching with hospital-based medicine that make financial solvency challenging: the strain of uninsured patients on revenue, workforce shortages driving up labor costs, and COVID-related volume impacts, to name a few.
What’s different with the average health system compared to Envision? While clearly rife with inefficiencies, health systems have mechanisms to self-correct.
Envision’s business model was not an innovation on care design or delivery.
It was a model taking advantage of pricing distortions and patients who are not in a position to shop for emergency care. That model inherently has limited running room.
On the physician practice front, Envision’s bankruptcy highlights the challenging business environment PE firms choose to enter when they invest in physician practices. Medical groups are a low-margin business, and the running room on cost savings has a low ceiling.
While many of the highest profile PE investments in physician groups come from firms with a long track record in the physician space, it remains to be seen whether the return on their investments will be high enough to satisfy investors.
The spotlight on large, heavily resourced healthcare organizations is not going away anytime soon. In fact, as consolidation continues, new investors enter the forefront, and organizations diversify the type of assets they acquire, that spotlight is only getting brighter.
With recent residency match data showing a 26 percent drop in applications to emergency medicine training programs since 2021, this article in the Washington Post grapples with why the once sought-after profession is now struggling with recruitment.
Some point to high rates of pandemic burnout and the unappealing nature of the work: emergency departments (EDs) are increasingly overcrowded, understaffed, and violent—turning ED docs into “the cops of medicine,” as one ED residency program leader put it. Others suggest that residents are simply following the money elsewhere, discouraged by reports of an impending oversupply of ED physicians in coming years.
The Gist: The days of the television drama ER, which inspired a generation of would-be doctors to pursue emergency medicine, are gone—most medical students graduating today weren’t even born when the show first aired in 1994. The article fails to note the changes in EDs brought on by investor-backed staffing companies, which now staff anywhere from an estimated quarter to half of the nation’s EDs.
They’re accused of cutting costs by hiring fewer ED docs, as well as funding more ED residency spots in an attempt to flood the market and drive down their future labor costs even further. In the wake of COVID, emergency physicians find themselves in EDs largely staffed by advanced practice providers.
While in the near-term hospitals will surely face challenges in staffing these critical roles, shortages may drive momentum to refine and expand technology- and team-based care models.
The executives featured in this article are all speaking at the Becker’s Healthcare 13th Annual Meeting April 3-6, 2023, at the Hyatt Regency in Chicago.
Question: What will hospitals and health systems look like in 10 years? What will be different and what will be the same?
Michael A. Slubowski. President and CEO of Trinity Health (Livonia, Mich.): In 10 years, inpatient hospitals will be more focused on emergency care, intensive/complex care following surgery or complex medical conditions, and short-stay/observation units. Only the most complex surgical cases and complex medical cases will be inpatient status. Most elective surgery and diagnostic services will be done in freestanding surgery, procedural and imaging centers. Many patients with chronic medical conditions will be managed at home using digital monitoring. More seniors will be cared for in homes and/or in PACE programs versus skilled nursing facilities.
Mark A. Schuster, MD, PhD. Founding Dean and Chief Executive Officer of Kaiser Permanente Bernard J. Tyson School of Medicine (Pasadena, Calif.): The future of hospitals might not actually unfold in hospitals. I expect that more and more of what we now do in hospitals will move into the home. The technology that makes this transition possible is already out there: Remote monitoring of vital signs and lab tests, remote visual exams, and videoconferencing with patients. And all of this technology will improve even more over the next 10 years — turning at-home care from a dream into a reality.
Imagine no longer being kept awake all night by beeps and alarms coming from other patients’ rooms or kept away from family by limited visiting hours. The benefits are especially welcome for people who live in rural places and other areas with limited medical facilities. Who knows? Maybe robotics will make some in-home surgeries not so far off!
Of course, not all patients have a safe or stable home environment where they could receive care, so hospitals aren’t going away anytime soon. I’m not suggesting that most current patients could be cared for remotely in a decade — but I do think we’re moving in that direction. So those of us who work in education will need to train medical, nursing, and other students for a healthcare future that looks quite different from the healthcare present and takes place in settings we couldn’t imagine 10 years ago.
Shireen Ahmad. System Director, Operations and Finance of CommonSpirit Health (Chicago): The biggest change I anticipate is a continuation in the decentralization of health services delivery that has typically been provided by hospitals. This will result in a reduction of hospitals with fewer services performed in acute settings and with more services provided in non-acute ones.
With recent reimbursement changes, CMS is helping to set the tone of where care is delivered. Hospitals are beginning to rationalize services, including who and where care is delivered. For example, pharmacies often carry clinics that provide vaccinations, but in France, one can go to a pharmacy for care and sterilization of minor wounds while only paying for bandages, medication and other supplies used in the visit. I would not be surprised if, in 10 years, one could get an MRI at their local Walmart or schedule routine screenings and tests at the grocery store with faster, more accurate results as they check out their produce.
If the pandemic has taught us anything, there will always be a need for acute care and our society will always need hospitals to provide care to sick patients. This is not something I would anticipate changing. However, the need to provide most care in a hospital will change with the result leading to fewer hospitals in total. Far from being a bleak outlook, however, I believe that healthier, sustainable health systems will prevail if they are able to provide a greater spectrum of care in broader settings focussing on quality and convenience.
Gerard Brogan. Senior Vice President and Chief Revenue Officer of Northwell Health (New Hyde Park, N.Y.): Operationally, hospitals and health systems will be more designed around the patient experience rather than the patient accommodating to the hospital design and operations. Specifically, more geared toward patient choice, shopping for services, and price competition for out-of-pocket expenses. In order to bring costs down, rational control of utilization will be more important than ever. Hopefully, we will be able to shrink the administrative costs of delivering care. Structurally, more care will continue to be done ambulatory, with hospitals having a greater proportion of beds having critical care capability and single rooms for infection control, putting pressure on the cost per square foot to operate. Sustainable funding strategies for safety net hospitals will be needed.
Mike Gentry. Executive Vice President and COO of Sentara Healthcare (Norfolk, Va.): During the next 10 years, more rural hospitals will become critical assessment facilities. The legislation will be passed to facilitate this transition. Relationships with larger sponsoring health systems will support easy transitions to higher acuity services as required. In urban areas, fewer hospitals with greater acuity and market share will often match the 50 percent plus market share of health plans. The ambulatory transition will have moved beyond only surgical procedures into outpatient but expanded historical medical inpatient status in ED/observation hubs.
The consumer/patient experience will be vastly improved. Investments in mobile digital applications will provide greatly enhanced communication, transparency of clinical status, timelines, the likelihood of expected outcomes and cost. Patients will proactively select from a menu of treatment options provided by predictive AI. The largest 10 health systems will represent 25 percent of the total U.S. acute care market share, largely due to consumer-centric strategic investments that have outpaced their competitors. Health systems will have vastly larger pharma operations/footprints.
Ketul J. Patel. CEO of Virginia Mason Franciscan Health (Seattle) and Division President, Pacific Northwest of CommonSpirit Health (Chicago): This is a transformative time in the healthcare industry, as hospitals and healthcare systems are evolving and innovating to meet the growing and changing needs of the communities we serve. The pandemic accelerated the digital transformation of healthcare. We have seen the proliferation of new technologies — telemedicine, artificial intelligence, robotics, and precision medicine — becoming an integral part of everyday clinical care. Healthcare consumers have become empowered through technology, with greater control and access to care than ever before.
Against this backdrop, in the next decade we’ll see healthcare consumerism influencing how health systems transform their hospitals. We will continue incorporating new technologies to improve healthcare delivery, offering more convenient ways to access high-quality care, and lowering the overall cost of care.
SMART hospitals, including at Virginia Mason Franciscan Health, are utilizing AI to harness real-time data and analysis to revolutionize patient and provider experiences and improve the quality of care. VMFH was the first health system in the Pacific Northwest to introduce a virtual hospital nearly a decade ago, which provides virtual services in the hospital across the continuum of care to improve quality and safety through remote patient monitoring and care delivery.
As hospitals become more high-tech, more nimble, and more efficient over the next 10 years, there will be less emphasis on brick-and-mortar buildings as we continue to move care away from the hospital toward more convenient settings for the patient. We recently launched VMFH Home Recovery Care, which brings all the essential elements of hospital-level care into the comfort and convenience of patients’ homes, offering a safe and effective alternative to the traditional inpatient stay.
Health systems and hospitals must simplify the care experience while reducing the overall cost of care. VMFH is building Washington state’s first hybrid emergency room/urgent care center, which eliminates the guesswork for patients unsure of where to go for care. By offering emergent and urgent care in a single location, patients get the appropriate level of care, at the right price, in one convenient location.
As healthcare delivery becomes more sophisticated in this digital age, we must not lose sight of why we do this work: our patients. There is no device or innovation that can truly replace the care and human intelligence provided by our nurses, APPs and physicians. So, while hospitals and health systems might look and feel different in 2033, our mission will remain the same: to provide exceptional, compassionate care to all — especially the most vulnerable.
David Sylvan. President of University Hospitals Ventures (Cleveland): American healthcare is facing an imperative. It’s clear that incremental improvements alone won’t manifest the structural outcomes that are largely overdue. The good news is that the healthcare industry itself has already initiated the disruption and self-disintermediation. I would hope that in the next 10 years, our offerings in healthcare truly reflect our efforts to adopt consumerism and patient choice, alleviate equity barriers and harness efficiencies while reducing time waste.
We know that some of this will come about through technology design, build and adoption, especially in the areas of generative artificial intelligence. But we also know that some of this will require a process overhaul, with learnings gleaned from other industries that have already solved adjacent challenges. What won’t change in 10 years will be the empathy and quality of care that the nation’s clinicians provide to patients and their caregivers daily.
Joseph Webb. CEO of Nashville (Tenn.) General Hospital: The United States healthcare industry operates within a culture that embraces capitalism as an economic system. The practice of capitalism facilitates a framework that is supported by the theory of consumerism. This theory posits that the more goods and services are purchased and consumed, the stronger an economy will be. With that in mind, healthcare is clearly a driver in the U.S. economy, and therefore, major capital and technology are continuously infused into healthcare systems. Healthcare is currently approaching 20 percent of the U.S. gross domestic product and will continue to escalate over the next 10 years.
Also, in 10 years, there will be major shifts in ownership structures, e.g., mergers, acquisitions, and consolidations. Many healthcare organizations/hospitals will be unable to sustain operations due to shrinking profit margins. This will lead to a higher likelihood of increasing closures among rural hospitals due to a lack of adequate reimbursement and rising costs associated with salaries for nurses, respiratory therapists, etc., as well as purchasing pharmaceuticals.
Aging baby boomers with chronic medical conditions will continue to dominate healthcare demand as a cohort group. To mitigate the rising costs of care, healthcare systems and providers will begin to rely even more heavily on artificial intelligence and smart devices. Population health initiatives will become more prevalent as the cost to support fragmented care becomes cost-prohibitive and payers such as CMS will continue to lead the way toward value-based care.
Because of structural and social conditions that tend to drive social determinants of health, which are fundamental causes of health disparities, achieving health equity will continue to be a major challenge in the U.S. Health equity is an elusive goal that can only be achieved when there is a more equitable distribution of SDOH.
Gary Baker. CEO, Hospital Division of HonorHealth (Scottsdale, Ariz.): In 10 years, I would expect hospitals in health systems to become more specialized for higher acuity service lines. Providing similar acute services at multiple locations will become difficult to maintain. Recruiting and retaining specialty clinical talent and adopting new technologies will require some redistribution of services to improve clinical quality and efficiency. Your local hospital may not provide a service and will be a navigator to the specialty facilities. Many services will be provided in ambulatory settings as technology and reimbursement allow/require. Investment in ambulatory services will continue for the next 10 years.
Michael Connelly. CEO Emeritus of Bon Secours Mercy Health (Cincinnati): Our society will be forced to embrace economic limits on healthcare services. The exploding elderly population, in combination with a shrinking workforce to fund Medicare/Medicaid and Social Security, will force our health system to ration care in new ways. These realities will increase the role of primary care as the needed coordinator of health services for patients. Diminishing fragmented healthcare and redundant care will become an increasing focus for health policy.
David Rahija. President of Skokie Hospital, NorthShore University HealthSystem (Evanston, Ill.): Health systems will evolve from being just a collection of hospitals, providers, and services to providing and coordinating care across a longitudinal care continuum. Health systems that are indispensable health partners to patients and communities by providing excellent outcomes through seamless, coordinated, and personalized care across a disease episode and a life span will thrive. Providers that only provide transactional care without a holistic, longitudinal relationship will either close or be consolidated. Care tailored to the personalized needs of patients and communities using team care models, technology, genomics, and analytics will be key to executing a personalized, seamless, and coordinated model of care.
Alexa Kimball, MD. President and CEO of Harvard Medical Faculty Physicians at Beth Israel Deaconess Medical Center (Boston): Ten years from now, hospitals will largely look the same — at least from the outside. Brick-and-mortar buildings aren’t going away anytime soon. What will differ is how care is delivered beyond the traditional four walls. Expect to see a more patient-centered and responsive system organized around what individuals need — when and where they need it.
Telehealth and remote patient monitoring will enable greater accessibility for patients in underserved areas and those who cannot get to a doctor’s office. Technology will not only enable doctors to deliver more personalized treatment plans but will also dramatically reshape physician workflows and processes. These digital tools will streamline administrative tasks, integrate voice commands, and provide more conducive work environments. I also envision greater access to data for both providers and patients. New self-service solutions for care management, scheduling, pricing, shopping for services, etc., will deliver a more proactive patient experience and make it easier to navigate their healthcare journey.
Ronda Lehman, PharmD. President of Mercy Health – Lima (Ohio):
This is a highly challenging question to address as we continue to reevaluate how healthcare is being delivered following several difficult years and knowing that financial challenges still loom. That said, when I am asked what it will look like, I am keenly aware of the fact that it only will look that way if we can envision a better way to improve the health of our communities. So 10 years from now, we need to have easier and more patient-driven access to care.
We will need to stop doing ‘to people’ and start caring ‘with people.’ Artificial intelligence and proliferous information that is readily available to consumers will continue to pave the way to patients being more empowered and educated about their options. So what will differentiate healthcare of the future? Enabling patients to make informed decisions.
Undoubtedly, technology will continue to advance, and along with it, the associated costs of research and development, but healthcare can only truly change if providers fundamentally shift their approach to how we care for patients. It is imperative that we need to transform from being the gatekeepers of valuable resources and services to being partners with patients on their journey. If that is what needs to be different, then what needs to be the same? We need the same highly motivated, highly skilled and perhaps most importantly, highly compassionate caregivers selflessly caring for one another and their communities.
Mike Young. President and CEO of Temple University Health System (Philadelphia): Cell therapy, gene therapy, and immunotherapy will continue to rapidly improve and evolve, replacing many traditional procedures with precise therapies to restore normal human function — either through cell transfer, altering of genetic information, or harnessing the body’s natural immune system to attack a particular disease like cancer, cystic fibrosis, heart disease, or diabetes. As a result, hospitals will decrease in footprint, while the labs dedicated to defining precision medicine will multiply in size to support individual- and disease-specific infusion, drug, and manipulative therapies.
Hospitals will continue to shepherd the patient journey through these therapies and also will continue to handle the most complex cases requiring high-tech medical and surgical procedures. Medical education will likely evolve in parallel, focusing more on genetic causation and treatment of disease, as well as proficiency with increasingly sophisticated AI diagnostic technologies to provide adaptive care on a patient-by-patient basis.
Tom Siemers. Chief Executive Officer of Wilbarger General Hospital (Vernon, Texas): My predictions include the national healthcare landscape will be dominated by a dozen or so large systems. ‘Consolidation’ will be the word that describes the healthcare industry over the next 10 years. Regional systems will merge into large, national systems. Independent and rural hospitals will become increasingly rare. They simply won’t be able to make the capital investments necessary to replace outdated facilities and equipment while vying with other organizations for scarce, licensed personnel.
Jim Heilsberg. CFO of Tri-State Memorial Hospital & Medical Campus (Clarkston, Wash.): Tri-State Hospital continues to expand services for outpatient services while maintaining traditionally needed inpatient services. In 10 years, there will be expanded outpatient services that include leveraged technology that will allow the patient to be cared for in a yet-to-be-seen care model, including traditional hospital settings and increasing home care setting solutions.
Jennifer Olson. COO of Children’s Minnesota (St. Paul, Minn.): I believe we will see more and better access to healthcare over the next 10 years. Advances in diagnostics, monitoring, and artificial intelligence will allow patients to access services at more convenient times and locations, including much more frequently at home, thereby extending health systems’ reach well beyond their walls.
What I don’t think will ever change is the heart our healthcare professionals bring with them to work every day. I see it here at Children’s Minnesota and across our industry: the unwavering commitment our caregivers have to help people live healthier lives.
If I had one wish for the future, it would be that we become better equipped to address the social determinants of health: all of the factors outside the walls of our hospitals and clinics that affect our patients’ well-being. Part of that means relaxing regulations to allow better communication and sharing of information among healthcare providers and public and private entities, so we can take a more holistic approach to improve health and decrease disparities. It also will require a fundamental shift in how health and healthcare are paid for.
Stonish Pierce. COO of Holy Cross Health, Trinity Health Florida: Over the next decade, many health systems will pivot from being ‘hospital’ systems to true ‘health’ systems. Based largely on responding to The Joint Commission’s New Requirements to Reduce Health Care Disparities, many health systems will place greater emphasis on reducing health disparities, enhanced attention to providing culturally competent care, addressing social determinants of health (including, but not limited to food, housing and transportation) and health equity. I’m proud to work for Trinity Health, a system that has already directed attention toward addressing health disparities, cultural competency and health equity.
Many systems will pivot from offering the full continuum of services at each hospital and instead focus on the core services for their respective communities, which enables long-term financial sustainability. At the same time, we will witness the proliferation of partnerships as adept health systems realize that they cannot fulfill every community’s needs alone. Depending upon the specialty and region of the country, we may see some transitioning away from the RVU physician compensation model to base salaries and value-based compensation to ensure health systems can serve their communities in the long term.
Driven largely by continued workforce supply shortages, we will also see innovation achieve its full potential. This will include, but not be limited to, virtual care models, robots to address functions currently performed by humans, and increased adoption of artificial intelligence and remote monitoring. Healthcare overall will achieve parity in technological adoption and innovation that we take for granted and have grown accustomed to in industries such as banking and the consumer service industries.
For what will remain the same, we can anticipate that government reimbursement will still not cover the cost of providing care, although systems will transition to offering care models and services that enable the best long-term financial sustainability. We will continue to see payers and retail pharmacies continue to evolve as consumer-friendly providers. We will continue to see systems make investments in ambulatory care and the most critically ill patients will remain in our hospitals.
Jamie Davis. Executive Director, Revenue Cycle Management of Banner Health (Phoenix): I think that we will see a continued shift in places of service to lower-cost delivery sources and unfavorable payer mix movement to Medicare Advantage and health exchange plans, degrading the value of gross revenue. The increased focus on cost containment, value-based care, inflation, and pricing transparency will hopefully push payers and providers to move to a more symbiotic relationship versus the adversarial one today. Additionally, we may see disruption in the technology space as the venture capital and private equity purchase boom that happened from 2019 to 2021 will mature and those entities come up for sale. If we want to continue to provide the best quality health outcomes to our patients and maintain profitability, we cannot look the same in 10 years as we do today.
James Lynn. System Vice President, Facilities and Support Services of Marshfield Clinic Health System (Wis.): There will be some aspects that will be different. For instance, there will be more players in the market and they will begin capturing a higher percentage of primary care patients. Walmart, Walgreens, CVS, Amazon, Google and others will begin to make inroads into primary care by utilizing VR and AI platforms. More and more procedures will be the same day. Fewer hospital stays will be needed for recovery as procedures become less invasive and faster. There will be increasing pressure on the federal government to make healthcare a right for all legal residents and it will be decoupled from employment status. On the other hand, what will stay the same is even though hospital stays will become shorter for some, we will also be experiencing an ever-aging population, so the same number of inpatient beds will likely be needed.
The December issue of Health Affairs included an intriguing study that sought to explain the recent trend toward more high-intensity billing in emergency departments (EDs). Using ED visit data for “treat-and-release” visits (i.e. ED patients who were not admitted to the hospital), the study found that visits deemed high-intensity, as defined by certain high-complexity or critical care billing codes, rose from around 5 percent of visits in 2006 to 19 percent in 2019.
The authors conclude that while about half of this increase can be explained by changes in patient case mix and available care services that were visible in claims data, the other half is due to the adoption of sophisticated revenue cycle management programs, and industry-wide changes to billing practices that include upcoding.
The Gist: At first blush, an increase in high-intensity ED billing may not be a bad thing, if it means that greater numbers of people with low-acuity needs are going to urgent care centers, and avoiding EDs for needs that can be managed elsewhere. But the study finds thattreat-and-release rates are going up for high-intensity patients.
Though the authors list many potential reasons for this—including the changed role of the ED as a diagnostic referral center used by primary care physicians for quick workups of complex patients, the growing number of multimorbid seniors, and value-based care’s pressure to reduce hospital admission rates in favor of more resource-intensive ED visits—we have a strong suspicion that good old-fashioned upcoding also plays a role, especially as the percentage of emergency medicine practices managed by private equity companies increased from four percent to over eleven percent across the same time period as the study.
At a recent health system retreat, the CFO shared data describing a trend we’ve observed at a number of systems: for the past few months, emergency department (ED) volumes have been up, but the percentage of patients admitted through the ED is precipitously down.
The CFO walked to through a run of data to diagnose possible causes of this “uncoupling” of ED visits and inpatient admissions. Overall, the severity of patients coming to the ED was higher compared to 2019, so it didn’t appear that the ED was being flooded with low-level cases that didn’t merit admission. Apart from the recent spike in respiratory illness brought on by the “tripledemic” of flu, COVID and RSV, there wasn’t a noteworthy change in case mix, or the types of patients and conditions being evaluated in the emergency room. (Fewer COVID patients were admitted compared to 2021, but that wasn’t enough to account for the decline.) The physicians staffing the ED hadn’t changed, so a shift in practice patterns was also unlikely.
A physician leader attending the retreat spoke up from the audience: “I can diagnose this for you. I work in the ED, and the problem is we can’t move them. Patients are sitting in the ED, in hallways, in observation, sometimes for days, because we can’t get a bed on the floor. The whole time we are treating them, and many of them get better, and we’re able to discharge them before a bed frees up.”
With nursing shortages and other staffing challenges, many hospitals have been unable to run at full capacity even if the demand for beds is there. So total admissions may be down, even if the hospital feels like it’s bursting at the seams.
The current staffing crisis not only presents a business challenge, but also adversely impacts patient experience, and makes it more difficult to deliver the highest quality care. A good reminder of the complexity of hospital operations, where strain in one part of the system will quickly impact the performance of other parts of the care delivery continuum.
St. Francis Medical Center in Trenton, N.J., on Dec. 21 transitioned to a freestanding emergency room that offers various outpatient services after Capital Health acquired the hospital from Trinity Health, according to PBS affiliate WHYY.
The campus, renamed Capital Health – East Trenton, must feature a primary family health clinic and a women’s OB/GYN clinic, according to terms of the transaction.
Other services, such as cardiac surgery, are moving to Capital Health Regional Medical Center in Trenton, where “extensive capital projects” are being planned, the health system said in a Dec. 8 news release.
A St. Francis spokesperson told the news outlet that the hospital had been financially struggling for years.
“St. Francis has done many great things for the Trenton community, but the current healthcare landscape has made it unsustainable,” Capital Health President and CEO Al Maghazehe said. “Without these key approvals, Trenton would have lost desperately needed healthcare services, including emergency services, behavioral health and cardiac surgery.”
Capital Health said it has taken “a significant risk” to try and prevent a healthcare crisis for Trenton’s 90,000 residents, according to the report.
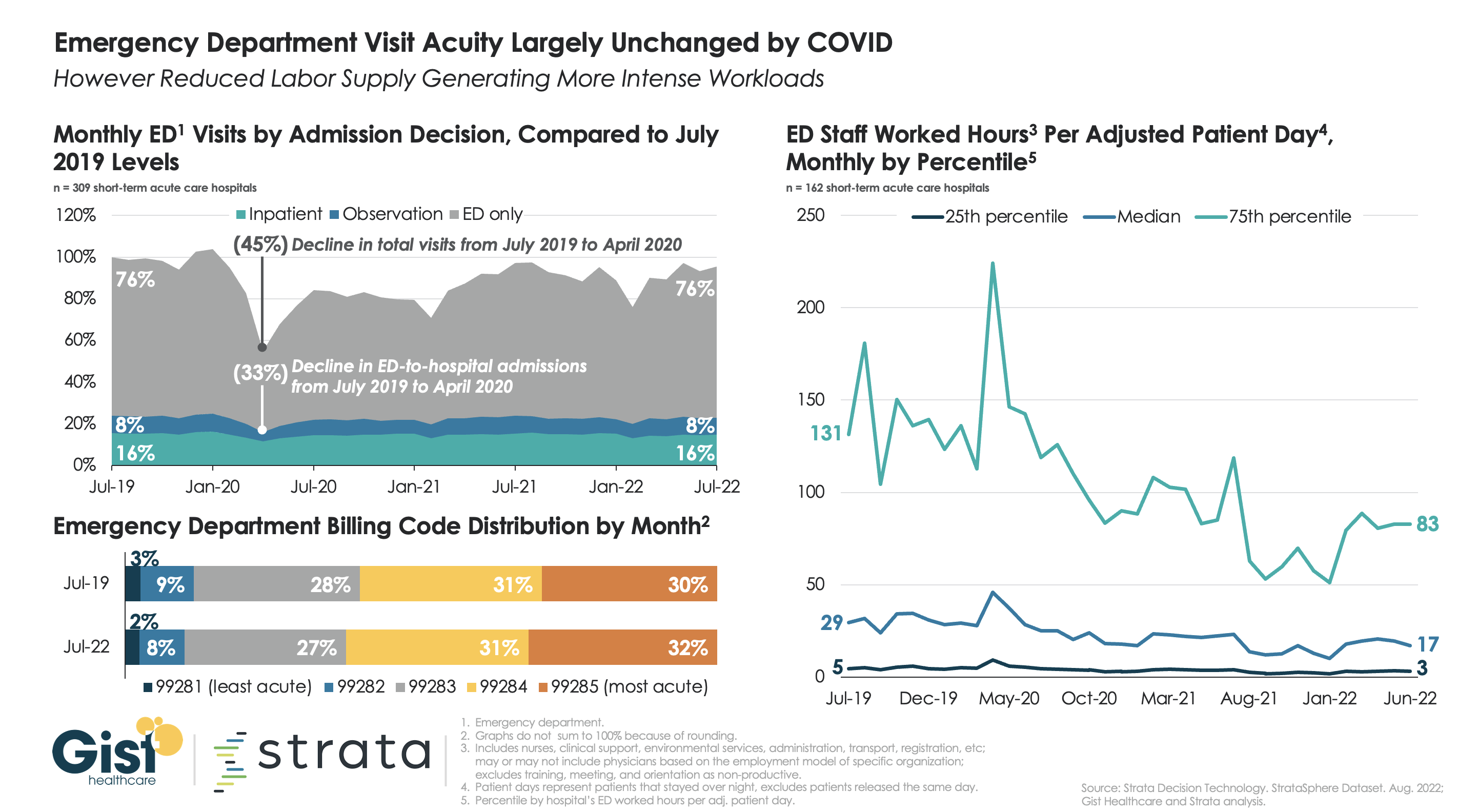
Many health systems are wondering if consumers are now leveraging new access points, including telemedicine, for low-acuity urgent care instead of going to the emergency department (ED), something which many experts are forecasting. For the graphic above, we partnered with healthcare software and analytics firm Strata Decision Technology to try to answer this question.
Using their national StrataSphere dataset for short-term acute care hospitals, we found that ED patient acuity levels in July 2022 were virtually identical to those in July 2019, though 2022 volumes were down by four percent.Admission and observation decisions across the two groups were also largely the same. We’ll be keeping our eye on the data to see if the story changes, as individuals who have delayed care over the last two and a half years now return, presenting to the ED with more advanced disease.
While current ED patients may not be more acute than before, the ongoing shortage of clinical labor may explain why some hospitals tell us that their EDs feel busier than ever. Measured by total worked hours of ED employees per adjusted patient day, the amount of labor dedicated to each patient requiring an overnight ED stay isdown around forty percent from 2019 across hospital EDs of all staffing levels. With fewer labor hours to go around, each team member on the floor now has more to do.
We’ve been noticing a disconnect recently in our conversations with health system executives. When we share national data that shows that emergency department visits are still down substantially from pre-COVID levels, the reaction is often one of surprise.
As one CEO recently put it to us, “We’re seeing exactly the opposite. Our ED feels busier than ever.” It appears that, upon further examination, what’s going on is a shift in the mix of patients who are visiting the ED. The lower-acuity, urgent-care level cases do seem to have shifted away from traditional hospital settings toward virtual visits and urgent care centers. That’s good news from an overall cost of care perspective, but it means that hospital EDs are increasingly filled with sicker, more acute patients.
One sure sign the mix has shifted: many systems are now telling us that the percentage of ED visitors who end up getting admitted is rising. But staffing-driven capacity constraints mean that it’s taking longer to find an inpatient bed for those patients, or to discharge them from the ED to other settings (or back home)—so the average length of stay in the ED is going up.
On top of that, many EDs are now seeing an increase in psych patients, who stay longer and require greater staff attention. All of that, along with staff who are completely exhausted and demoralized after the pandemic, has combined to make many EDs feel swamped these days—despite what the national data are showing.