In the rapidly evolving landscape of U.S. healthcare, the tug-of-war between payers and providers is continually intensifying, raising the stakes on the strategic maneuvers that shape the industry’s financial and operational dynamics.
The crux of the issue lies in the increasingly sophisticated strategies employed by insurance companies to deny claims: a move that ostensibly aims to safeguard their bottom lines, often at the expense of provider sustainability and patient access.
The rise in denial rates is more than a mere statistic; it’s a symptom of a broader systemic challenge that calls for strategic foresight and robust expertise. In this intricate environment, providers face numerous administrative challenges, working to balance clinical decisions with financial sustainability.
Drawn from in-depth proprietary analytics, clinical regulatory expertise and decades of experience, CorroHealth addresses what is needed to successfully combat payer denial tactics. Broader industry trends, such as the shift towards value-based care and the increasing emphasis on patient-centric models, will continue to disrupt the historic provider business model. CorroHealth’s insights offer a beacon for steering through these turbulent waters. Their strategic recommendations, from optimizing contract negotiations to leveraging data analytics to managing payer denials, to formalizing escalation paths, reflect a comprehensive approach to mitigating the adverse effects of ever-shifting payer denial tactics.
Delving deeper into the anatomy of payer denials reveals a long-term pattern of deliberate complexity designed to wear down provider resilience. By dissecting the layers of denial management, from initial claim submission to final resolution, CorroHealth uncovers pivotal areas where targeted interventions dramatically shift outcomes in favor of healthcare providers.
This process involves a granular analysis of denial codes, predictive analytics to pre-empt possible denials and rigorous training staff to maneuver through the intricate appeals process effectively.
Taking a proactive stance towards payer contract management, their approach emphasizes the importance of scrutinizing the fine print and negotiating terms that anticipate and mitigate denial strategies. CorroHealth advocates on the providers’ behalf for clearer definitions of medical necessity, timely filing limits and transparent appeal processes. By equipping providers with negotiation tactics grounded in comprehensive data analysis and a deep understanding of payer methodologies, their contracts become a tool for protection against denials, rather than a source of vulnerability.
Woven throughout this work is CorroHealth’s commitment to advancing the dialogue between payers and providers toward a more equitable healthcare system. Through forums, partnerships and collaborative initiatives, CorroHealth bridges the gap between these two entities, fostering an environment where mutual understanding and respect pave the way for innovative solutions to longstanding challenges.
Hospitals and health systems require an experienced partner to navigate the complexities of the healthcare landscape, balancing financial sustainability with top-tier patient care. CorroHealth offers a comprehensive suite of solutions to address challenges associated with payer denials, enabling providers to recover lost revenues and uphold the fundamental goal of accessible, high-quality patient care. Beyond financial strategies and operational adjustments, the narrative calls for a more productive and transparent dialogue between payers and providers. This aims to encourage an ecosystem where financial sustainability and high-quality patient care are complementary facets of holistic healthcare delivery.
Facing these challenges, the importance of strategic partnerships becomes increasingly vital for healthcare providers. Such alliances are indispensable in maneuvering through the complex healthcare landscape and are strengthened by CorroHealth’s comprehensive understanding of the payer-provider dynamic and dedication to fostering innovation. A collaborative approach is essential for progressing towards a healthcare system characterized by greater equity and efficiency.
The industry stands at an existential crossroads. The insights and strategies shared by CorroHealth serve as a testament to the company’s expertise and its dedication to shaping a future where healthcare is accessible, affordable and effective for all.
It’s no secret I feel strongly that “Medicare Advantage for All” is not a healthy end goal for universal health care coverage in our country. But I also recognize there are many folks, across the political spectrum, who see the program as one that has some merit. And it’s not going away anytime soon. To say the insurance industry has clout in Washington is an understatement.
As politicians in both parties increase their scrutiny of Medicare Advantage, and the Biden administration reviews proposed reforms to the program, I think it’s important to highlight common-sense, achievable changes with broad appeal that would address the many problems with MA and begin leveling the playing field with the traditional Medicare program.
1. Align prior authorization MA standards with traditional Medicare
Since my mother entered into an MA plan more than a decade ago, I’ve watched how health insurers have applied practices from traditional employer-based plans to MA beneficiaries. For many years, insurers have made doctors submit a proposed course of treatment for a patient to the insurance company for payment pre-approval — widely known as “prior authorization.”
While most prior authorization requests are approved, and most of those denied are approved if they are appealed, prior authorization accomplishes two things that increase insurers’ margins.
The practice adds a hurdle between diagnosis and treatment and increases the likelihood that a patient or doctor won’t follow through, which decreases the odds that the insurer will ultimately have to pay a claim. In addition, prior authorization increases the length of time insurers can hold on to premium dollars, which they invest to drive higher earnings. (A considerable percentage of insurers’ profits come from the investments they make using the premiums you pay.)
Last year, the Kaiser Family Foundation found the level of prior authorization requests in MA plans increased significantly in recent years, which is partially the result of the share of services subject to prior authorization increasing dramatically. While most requests were ultimately approved (as they were with employer-based insurance plans), the process delayed care and kept dollars in insurers’ coffers longer.
The outrage generated by older Americans in MA plans waiting for prior authorization approvals has moved the Biden administration to action.
Beginning in 2024, MA plans may be no more restrictive with prior authorization requirements than traditional Medicare.
That’s a significant change and one for which Health and Human Services Secretary Xavier Becerra should be lauded.
But as large provider groups like the American Hospital Association have pointed out, the federal government must remain vigilant in its enforcement of this rule. As I wrote about recently with the implementation of the No Surprises Act, well-intentioned legislation and implementation rules put in place by regulators can have little real-world impact if insurers are not held accountable. It’s important to note, though, that federal regulatory agencies must be adequately staffed and resourced to be able to police the industry and address insurers’ relentless efforts to find loopholes in federal policy to maximize profits. Congress needs to provide the Department of Health and Human Services with additional funding for enforcement activities, for HHS to require transparency and reporting by insurers on their practices, and for stakeholders, especially providers and patients, to have an avenue to raise concerns with insurers’ practices as they become apparent.
2. Protect seniors from marketing scams
If it’s fall, it’s football season. And that means it’s time for former NFL quarterback Joe Namath’s annual call to action on the airwaves for MA enrollment.
As Congresswoman Jan Schakowsky and I wrote about more than a year ago, these innocent-appearing advertisements are misleading at their best and fraudulent at their worst. Thankfully, this is another area the Biden administration has also been watching over the past year.
CMS now prohibits the use of ads that do not mention a specific plan name or that use the Medicare name and logos in a misleading way, the marketing of benefits in a service area where they are not available, and the use of superlatives (e.g., “best” or “most”) in marketing when not substantiated by data from the current or prior year.
As part of its efforts to enforce the new marketing restrictions, the Center for Medicare and Medicaid Services for the first time evaluated more than 3,000 MA ads before they ran in advance of 2024 open enrollment. It rejected more than 1,000 for being misleading, confusing, or otherwise non-compliant with the new requirements. These types of reviews will, I hope, continue.
CMS has proposed a fixed payment to brokers of MA plans that, if implemented, would significantly improve the problem of steering seniors to the highest-paying plan — with the highest compensation for the insurance broker. I think we can all agree brokers should be required to direct their clients to the best product, not the one that pays the broker the most. (That has been established practice for financial advisors for many years.) CMS should see this rule through, and send MA brokers profiteering off seniors packing.
A bonus regulation in this space to consider: banning MA plan brokers from selling the contact information of MA beneficiaries. Ever wonder why grandma and grandpa get so many spam calls targeting their health conditions? This practice has a lot to do with it. And there’s bipartisan support in Congress for banning sales of beneficiary contact information.
In addition, just as drug companies have to mention the potential side effects of their medications, MA plans should also be required to be forthcoming about their restrictions, including prior authorization requirements, limited networks, and potentially high out-of-pocket costs, in their ads and marketing materials.
3. Be real about supplemental benefits
Tell me if this one sounds familiar. The federal government introduced flexibility to MA plans to offer seniors benefits beyond what they can receive in traditional Medicare funded primarily through taxpayer dollars.
Those “supplemental” benefits were intended to keep seniors active and healthy. Instead, insurers have manipulated the program to offer benefits seniors are less likely to use, so more of the dollars CMS doles out to pay for those benefits stay with payers.
Many seniors in MA plans will see options to enroll in wellness plans, access gym memberships, acquire food vouchers, pick out new sneakers, and even help pay for pet care, believe it or not — all included under their MA plan. Those benefits are paid for by a pot of “rebate” dollars that CMS passes through to plans, with the presumed goal of improving health outcomes through innovative uses.
There is a growing sense, though, that insurers have figured out how to game this system. While some of these offerings seem appealing and are certainly a focus of marketing by insurers, how heavily are they being used? How heavily do insurers communicate to seniors that they have these benefits, once seniors have signed up for them? Are insurers offering things people are actually using? Or are insurers strategically offering benefits that are rarely used?
Those answers are important because MA plans do not have to pay unused rebate dollars back to the federal government.
CMS in 2024 is requiring insurers to submit detailed data for the first time on how seniors are using these benefits. The agency should lean into this effort and ensure plan compliance with the reporting. And as this year rolls on, CMS should be prepared to make the case to Congress that we expect the data to show that plans are pocketing many of these dollars, and they are not significantly improving health outcomes of older Americans.
4. Addressing coding intensity
If you’re a regular reader, you probably know one of my core views on traditional Medicare vs. Medicare Advantage plans. Traditional Medicare has straightforward, transparent payment, while Medicare Advantage presents more avenues for insurers to arbitrarily raise what they charge the government. A good example of this is in higher coding per patient found in MA plans relative to Traditional Medicare.
An older patient goes in to see their doctor. They are diagnosed, and prescribed a course of treatment. Under Traditional Medicare, that service performed by the doctor is coded and reimbursed. The payment is generally the same no matter what conditions or health history that patient brought into the exam room. Straightforward.
MA plans, however, pay more when more codes are added to a diagnosis.
Plans have advertised this to doctors, incentivizing the providers to add every possible code to a submission for reimbursement. So, if that same patient described above has diabetes, but they’re being treated for an unrelated flu diagnosis, the doctor is incentivized by MA to add a code for diabetes treatment. MA plans, in turn, get paid more by the government based on their enrollee’s health status, as determined based on the diagnoses associated with that individual.
Extrapolate that out across tens of millions of seniors with MA plans, and it’s clear MA plans are significantly overcharging the federal government because of over-coding.
One solution I find appealing: similar to fee-for-service, create a new baseline for payments in MA plans to remove the incentive to add more codes to submissions. Proposals I’ve seen would pay providers more than traditional Medicare but without creating the plan-driven incentive for doctors to over-code.
5. Focusing in on Medicare Advantage network cuts in rural areas
Rural America is older and unhealthier than the national average. This should be the area where MA plans should experience the highest utilization.
Instead, we’re seeing that the aggressive practices insurers use to maximize profits force many rural hospitals to cancel their contracts with MA plans. As we wrote about at length in December, MA is becoming a ghost benefit for seniors living in rural communities. The reimbursement rates these plans pay hospitals in rural communities are significantly lower than traditional Medicare. That has further stressed the low margins rural hospitals face.
As Congressional focus on MA grows, I predict more bipartisan recommendations to come forth that address the growing gap between MA plan payments and what hospitals need to be paid in rural areas.
If MA is not accepted by providers in older, rural America, then truly, what purpose does it serve?
Generative AI applications can already help health systems improve margins, yet only 6% have a strategy ready.
At a Glance
In the wake of their most challenging financial year since 2020, US hospitals are desperately searching for margin improvements.
Generative AI can increase productivity and cost efficiency, but only 6% of health systems currently have a strategy.
Leading providers and payers will start with highly focused, low-risk generative AI use cases, generating the funds and experience for more transformative future applications.
While Covid-19 may no longer be dominating the global news cycle, healthcare providers and payers are still feeling its reverberations. More than half of US hospitals ended 2022 with a negative margin, marking the most difficult financial year since the start of the pandemic.
CEOs and CFOs remember the challenges all too well: The Omicron surge halted nonurgent procedures in the first half of the year, government support tapered off, and labor expenses ballooned amid staffing shortages. There was also the record-high inflation that continues to intensify margin pressures today. According to a recent Bain survey of health system executives, 60% cite rising costs as their greatest concern.
Payers and providers are now on the hunt for margin improvements. In our experience, the most successful companies won’t merely reduce costs, but also ramp up productivity. When done right, modest technology investments can accomplish both.
Artificial intelligence (AI) may hold part of the answer. With the costs to train a system down 1,000-fold since 2017, AI provides an arsenal of new productivity-enhancing tools at a low investment.
Many executives recognize the growing opportunity, especially with the recent rise of generative AI, which uses sophisticated large language models (LLMs) to create original text, images, and other content. It’s inspiring an explosion of ideas around use cases, from reviewing medical records for accuracy to making diagnoses and treatment recommendations.
Our survey reveals that 75% of health system executives believe generative AI has reached a turning point in its ability to reshape the industry. However, only 6% have an established generative AI strategy.
It’s time to play offense—or be forced to play defense later. But choosing from the laundry list of generative AI applications is daunting. Companies are at high risk of overinvesting in the wrong opportunities and underinvesting in the right ones, undermining future profitability, growth, and value creation. A wait-and-see approach is a tempting prospect.
However, we believe the next generation of leading healthcare companies will start today, with highly focused, low-risk use cases that boost productivity and cost efficiency. Over the next three to nine months, these companies will improve margins and learn how to implement a generative AI strategy, building up the funds and experience needed to invest in a more transformative vision.
Endless potential—and high hurdles
The excitement around generative AI may feel akin to the hype around other recent digital and technology developments that never quite rose to their promised potential. Well-intentioned, well-informed individuals are debating how much change will truly materialize in the next few years. While developments over the past six months have been a testament to the breakneck speed of change, nobody can accurately predict what the next six months, year, or decade will look like. Will new players emerge? Will we rely on different LLMs for different use cases, or will one dominate the landscape?
Despite the uncertainty, generative AI already has the power to alleviate some of providers’ biggest woes, which include rising costs and high inflation, clinician shortages, and physician burnout. Quick relief is critical, considering that the heightened risk of a recession will only compound margin pressures, and the US could be short 40,800 to 104,900 physicians by 2030, according to the Association of American Medical Colleges.
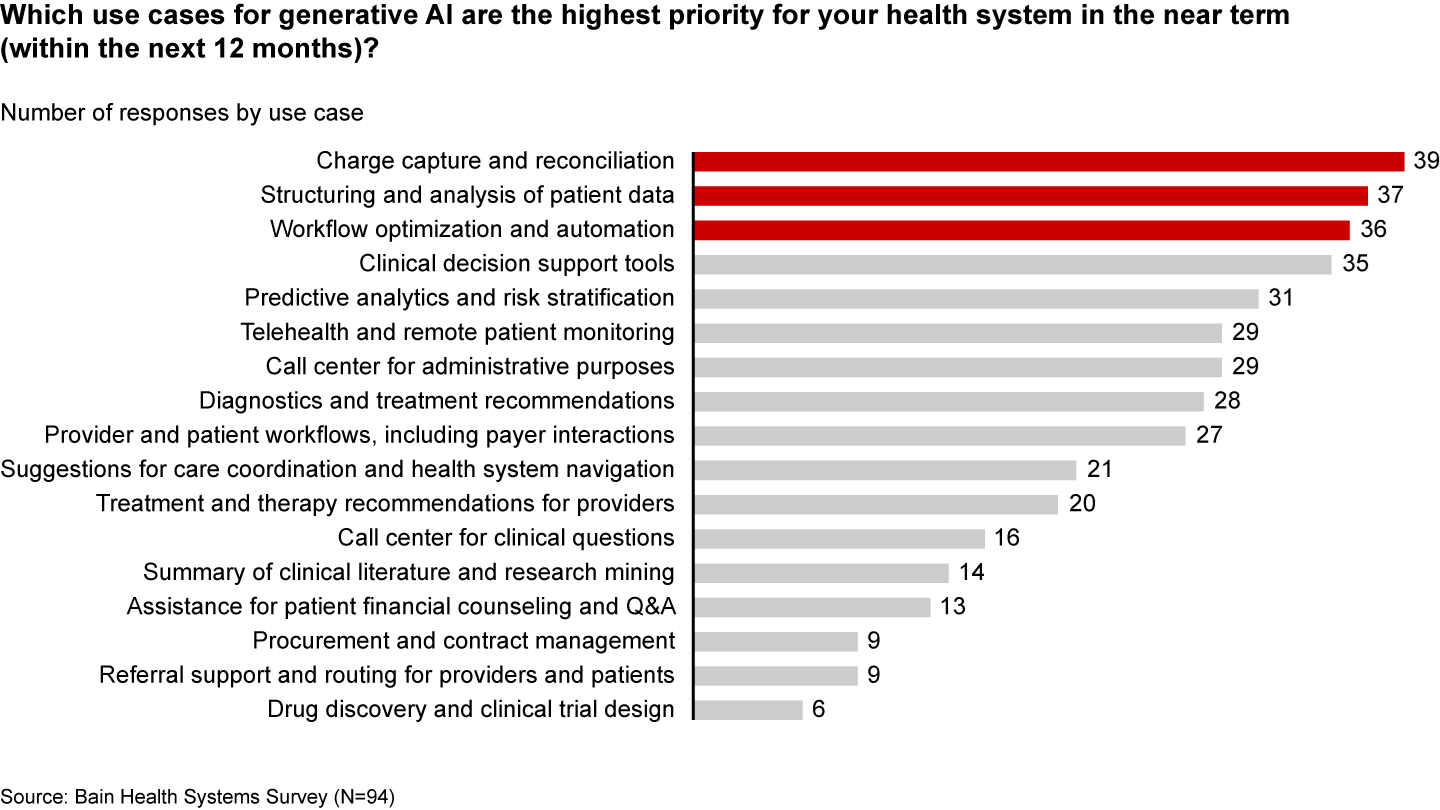
Many health systems are eyeing imminent opportunities to reduce administrative burdens and enhance operational efficiency. They rank improving clinical documentation, structuring and analyzing patient data, and optimizing workflows as their top three priorities (see Figure 1).
Figure 1
In the near term, generative AI can reduce administrative burdens and enhance efficiency
Some generative AI applications are already streamlining administrative tasks and allowing thinly stretched physicians to spend more time with patients. For instance, Doximity is rolling out a ChatGPT tool that can draft preauthorization and appeal letters. HCA Healthcare partnered with Parlance, a conversational AI-based switchboard, to improve its call center experience while reducing operators’ workload. And there are new announcements seemingly every week: Consider how healthcare software company Epic Systems is incorporating ChatGPT with electronic health records (EHRs) to draft response messages to patients, or how Google Cloud is launching an AI-enabled Claims Acceleration Suite for prior authorization processing.
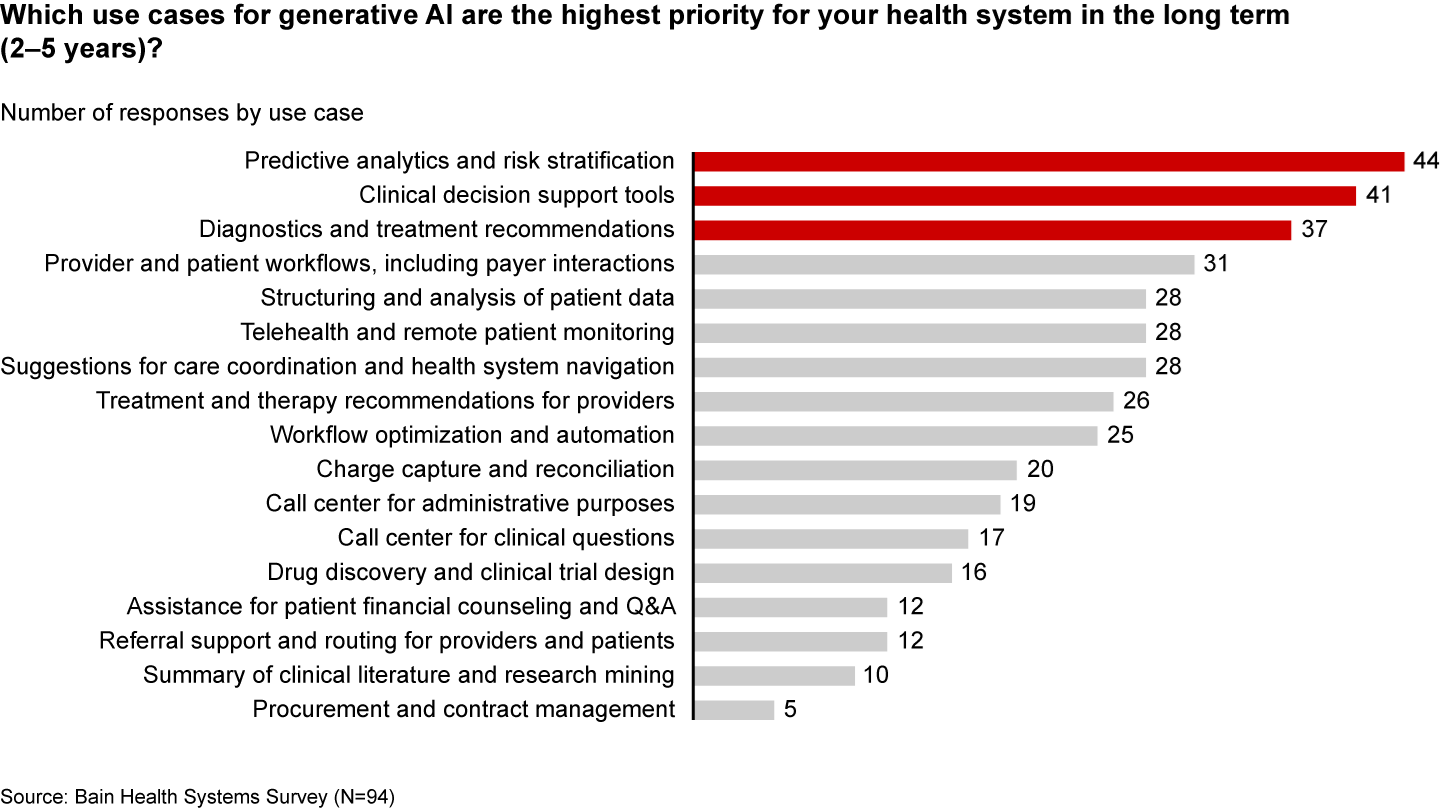
These applications only scratch the surface of potential. In the future, generative AI could profoundly transform care delivery and patient outcomes. Looking ahead two to five years, executives are most interested in predictive analytics, clinical decision support, and treatment recommendations (see Figure 2).
Figure 2
Predictive analytics, clinical decisions, and care recommendations are long-term generative AI priorities
It’s hard not to catch AI “fever.” But there are real challenges ahead. Some are already tackling the biggest questions: Organizations such as Duke Health, Stanford Medicine, Google, and Microsoft have formed the Coalition for Health AI to create guidelines for responsible AI systems. Even so, solutions to the greatest hurdles aren’t yet keeping up with the rapid technology development.
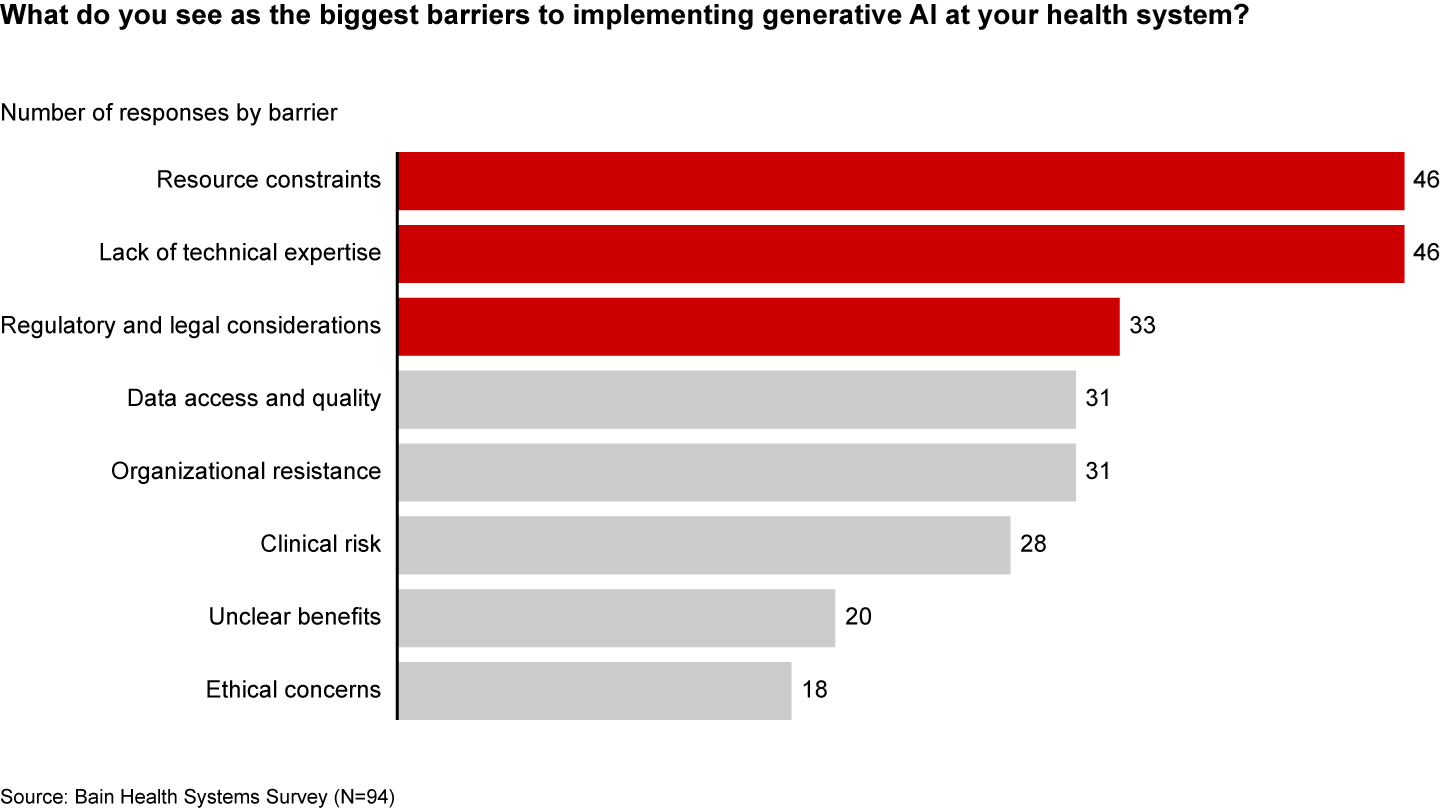
Resource and cost constraints, a lack of expertise, and regulatory and legal considerations are the largest barriers to implementing generative AI, according to executives (see Figure 3).
Figure 3
A lack of resources, expertise, and regulation are the biggest barriers to generative AI in healthcare
Even when organizations can overcome these hurdles, one major challenge remains: focus and prioritization. In many boardrooms, executives are debating overwhelming lists of potential generative AI investments, only to deem them incomplete or outdated given the dizzying pace of innovation. These protracted debates are a waste of precious organizational energy—and time.
Starting small to win big
Setting the bar too high is setting up for failure. It’s easy to get caught up, betting big on what seems like the greatest opportunity in the moment. But 12 months later, leaders often find themselves frustrated that they haven’t seen results or feeling as if they’ve made a misplaced bet. Momentum and investments slow, further hindering progress.
Leading companies are forming a more pragmatic strategy that considers current capabilities, regulations, and barriers to adoption. Their CEOs and CFOs work together to enforce four guiding principles:
Pilot low-risk applications with a narrow focus first. Tomorrow’s leaders are making no-regret moves to deliver savings and productivity enhancements in short order—at a time when they need it most. Gaining experience with currently available technology, they are testing and learning their way to minimum viable products in low-risk, repeatable use cases. These quick wins are typically in areas where they already have the right data, can create tight guardrails, and see a strong potential return on investment. Some, like call center and chatbot support, can improve the patient experience. However, given the current challenges around regulation and compliance, the most successful early initiatives are likely to be internally focused, such as billing or scheduling. Most importantly, executives prioritize initiatives by potential savings, value, and cost.
Decide to buy, partner, or build. CEOs will need to think about how to invest in different use cases based on availability of third-party technology and importance of the initiative.
Funnel cost savings and experience into bigger bets. As the technology matures and the value becomes clear, companies that generate savings, accumulate experience, and build organizational buy-in today will be best positioned for the next wave of more sophisticated, transformative use cases. These include higher-risk clinical activities with a greater need for accuracy due to ethical and regulatory considerations, such as clinical decision support, as well as administrative activities that require third-party integration, such as prior authorization.
Remember generative AI isn’t a strategy unto itself. To build a true competitive advantage, top CEOs and CFOs are selective and discerning, ensuring that every generative AI initiative reinforces and enables their overarching goals.
Some health systems are already seeing powerful results from relatively small, more practical investments. For instance, recognizing that clinicians were spending an extra 130 minutes per day outside of working hours on administrative tasks, the University of Kansas Health System partnered with Abridge, a generative AI platform, to reduce documentation burden. By summarizing the most important points from provider-patient conversations, Abridge is improving the quality and consistency of documentation, getting more patients in the door, and cutting down on pervasive physician burnout.
Although it will require some upfront investment, in the long run it will be more costly to underestimate the level and speed at which generative AI will transform healthcare. The next generation of leaders will start testing, learning, and saving today, putting them on a path to eventually revolutionize their businesses.
Hospitals can decrease denials by having physicians involved in the mid-revenue cycle review process.
Involving physicians in the mid-revenue cycle process can increase hospital ROI by 700%, according to Enjoin CEO Dr. James Fee.
Hospitals and health systems can improve revenue through a pre-bill review prior to claims submission, according to Fee. Enjoin does this work as a revenue cycle consulting business focused on documentation and coding.
One of the first things Enjoin physicians check is that the care of the patient has been properly recorded.
“We’re never taught how to communicate with those who record our work, so it can be captured in the coding system,” said Fee, who continues to practice as a physician in Baton Rouge, Louisiana.
Secondly, hospitals need to check the accuracy of the representation of that patient.
“You want to make sure the severity of the patient is justified to get appropriately reimbursed,” Fee said.
WHY THIS MATTERS
Documentation and coding falls in the middle of the revenue cycle. Through a pre-bill review of the estimated 30-50% of cases that are chosen for review at this stage because of their complexity, organizations can ensure the documentation supports coding compliance, MS-DRG accuracy, quality performance data and other measures.
Results have shown an impressive 700% percent ROI on average and in some cases, 1,000%, according to Fee. On average, the process shows a 17% decline in denial rates.
Hospitals already have clinical staff in the rev cycle. Physicians add a layer of review.
“We have practicing physicians who understand the disease process,” Fee said. “We look at a case to make sure the diagnosis is correct. What was the focus of care for that hospital stay? That takes a level of clinical interpretation.”
Enjoin, which has been around for about 30 years, does not offer a software product, but uses an analytics platform. It partners with clients as consultants in a technically agnostic way.
Fee will speak on the topic “Mid-Revenue Cycle Drives Financial Stability During COVID19: How One Academic Medical Center Prospered,” in-person during the Healthcare Financial Management Association annual conference, Monday, November 8, in Minneapolis.
AUTOMATION
As revenue cycle directors look to automate, this is more easily done on the front and back ends of the revenue cycle rather than the mid-cycle process, according to Fee. This is one area that will have to wait until AI makes it possible to interpret the data seen by physicians and other clinicians, he said.
“Automation is easy to say as one-stop shopping for an easy solution, but you need to understand what you’re automating,” he said.
There can be an automation component to the prioritization of reviews, something Enjoin plans to bring to market soon.
“Automation will continue to rapidly grow,” Fee said, “but there will always be that people component.”
THE LARGER TREND
As in other areas of healthcare, COVID-19 brought a level of uncertainty about the proper testing and diagnosis recorded in the revenue cycle.
During the most recent wave of COVID-19, many hospital ICU beds were again full, and health systems once again were canceling elective surgeries, with a resulting loss of revenue.
Higher expenses for labor, drugs and supplies, as well as a continuation of delayed care, are projected to cost hospitals an estimated $54 billion in net income over the course of this year, according to Kaufman Hall analysis released last month by the American Hospital Association.
“The biggest impact for reimbursement was the loss of patient care,” Fee said. “We were in a fee-for-service model and margins were driven by elective surgeries.”
COVID-19 also shifted the commercial dominance of margins to lower-paying government reimbursement as employees lost their jobs, according to Fee.
During the first COVID-19 wave in 2020, CFOs were asking he said, “How do I adapt to that?” Many looked to prevent financial leakage in employing resources they already had.
“That’s where CDI (Clinical Documentation Improvement) is helpful,” Fee said.