

Cartoon – OK, I’m sensing a lot of negativity


Steward Health now owns and operates 36 hospitals across the United States, making it the country’s largest private hospital operator.
The Boston-based physician-led organization’s merger with IASIS Healthcare was completed late last week.
Steward Health did not disclose the cost of the deal, but Boston Business Journal reported that Medical Properties Trust contributed $1.4 billion of the $1.9 billion purchase of the acquired hospital’s real estate that was part of the agreement. The organization projected the deal will lead to revenues of almost $8 billion in 2018.
Steward will now oversee 36 individual hospitals across 10 states, managed care operations in Arizona, Utah and Massachusetts, and employ 37,000 people, including 1,400 physicians and 4,700 integrated network physicians.
“This merger enables Steward to expand our successful, physician-led, integrated care model. We look forward to providing the highest quality of care through keeping patients healthy and being available with advanced care in their community, should they need it,” said Ralph de la Torre, M.D., chairman and CEO of Steward Health Care, in an announcement. “Steward will be introducing patients, physicians, and employees in six new states to our innovative programs and community commitment model.”
Iasis Healthcare CEO W. Carl Whitmer stepped down from his position on Friday after the deal closed. “I’m leaving proud of what we together have accomplished and excited about the possibilities that lie ahead for all of us,” Whitmer said in a written statement to the hospital chain’s employees, according to The Tennessean. Whitmer served as CEO for 17 years.
The acquisition includes four hospitals in Arizona, one hospital in Arkansas, one hospital in Colorado, one in Louisiana, six hospitals in Texas and five in Utah.

Inpatient drug costs will continue to rise for nonprofit and public U.S. hospitals, but the pace of drug price increases will likely slow down amid growing scrutiny of drug manufacturers’ pricing practices.
But even with the slowing rate of price increases, the rising drug costs and potential changes to Medicare 340B payments for outpatient drugs would further reduce hospital margins, according to a new report from Moody’s Investors Service.
Pharmaceutical costs have outpaced hospital revenue growth in recent years, contributing to weaker operating margins, Moody’s finds. “Price increases in recent years were extraordinarily high for certain branded hospital inpatient drugs, but drug manufacturers are pulling back on these increases,” said Diana Lee, a Moody’s vice president. “On the generic drug side, we expect that some of the pressure will ease as the U.S. Food and Drug Administration approves more generic drugs for the first time.”
However, the government’s proposed reduction of Medicare Part B outpatient drug reimbursement to 340B hospitals by roughly 30% would hurt hospital margins.
“Hospitals and health systems of varying size and across the rating spectrum have noted anecdotally that they have benefited from cost savings from this discount drug program,” Lee says. “In some instances, the savings and income gained from this program can be meaningful relative to total operating cash flow. While about half of hospitals in the nation are 340B providers, those that have limited financial flexibility would be most exposed to possible changes to the 340B program.”
Hospitals and industry trade groups have urged the Centers for Medicare & Medicaid Services to withdraw its proposal to cut the drug payments to hospitals in the federal drug discount program. Hospitals use the savings to waive copays and provide drugs and other services for free or reduced costs to low-income patients.
Last week a bipartisan group of more than 220 members of the House of Representatives also told CMS in a letter (PDF) they oppose the proposal.
“This program is a lifeline for the hospitals that serve our most vulnerable patients. These arbitrary cuts will do nothing to improve patient care, or address rising costs in the Medicare program. Instead they simply jeopardize access to the treatments and services that 340B hospitals provide,” said Rep. Mike Thompson (D-Calif.) in an announcement. “There is robust bipartisan agreement that CMS should go back to the drawing board to prevent harm to patients across the country.”
Rep. David P. McKinley (R-W.Va.) said CMS’ proposal was “misguided.” “Our letter shows strong bipartisan opposition to this proposed rule, and hopefully will convince CMS to change course. We must address the high costs of drugs, but this is not the way to do it,” he said.
Meanwhile, the Health Resources and Services Administration has once again delayed (PDF) the effective date of a different 340B final rule that would set drug price ceilings and penalties for drug manufacturers that knowingly overcharge hospitals for drugs purchased under the program. The Department of Health and Human Services said it has delayed the effective date to July 1, 2018, to give more time to make changes to facilitate compliance. “After reviewing the comments received from stakeholders regarding objections on the timing of the effective date and challenges associated with the complying with the final rule, HHS has determined that delaying the effective date to July 1, 2018, is necessary to consider some of the issues raised.”
https://www.axios.com/vitals-2492155989.html
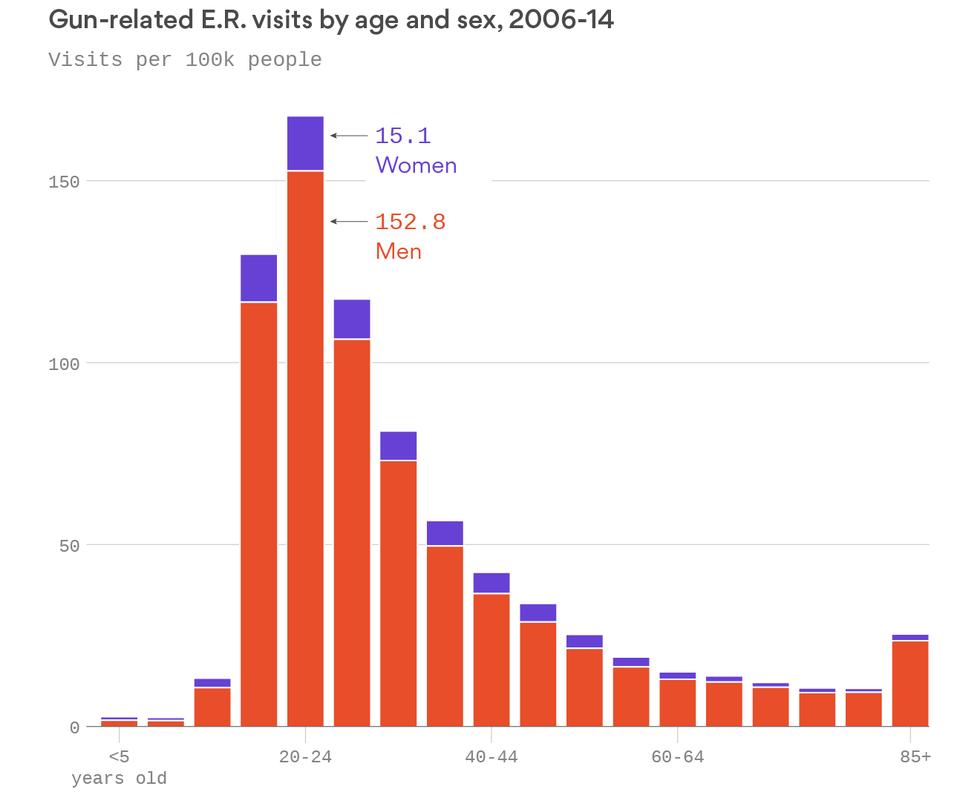
Good morning … Our thoughts are with the victims of the horrific mass shooting in Las Vegas, and their families. If you haven’t yet, spend a minute with this graphic, from the Axios visuals team. Whatever your opinions about gun control, mental health interventions, or any other questions of public policy, it’s a stark look at the human toll of mass shootings.
Gun-related injuries send thousands of people to emergency rooms every year, even aside from mass shootings like the tragedy in Las Vegas. In 2015 alone, almost 35,000 people died from gun-related homicides and suicides, and the “clinical burden” from non-fatal gun injuries was three times higher, according to new research published in Health Affairs.
Go deeper: Health Affairs is providing free access to this study. You can read the whole thing here.
https://www.axios.com/the-fuzzy-math-around-community-health-systems-hospital-sales-2491001792.html

Why it matters: The discrepancy between CHS’ words and actions raises questions. If CHS sold profitable hospitals for low prices, the company could continue to struggle paying down its mountain of debt because it will have fewer facilities to generate cash. Some investors already believe CHS could default on its debt.
The background: Hospitals are often sold based on a measure of profitability called earnings before interest, tax, depreciation and amortization, or EBITDA. Prices vary based on location, profit, insurance contracts and other factors, but the average hospital today could be sold at 8.5 times its EBITDA, according to one industry estimate.
CHS CEO Wayne Smith and former CFO Larry Cash both have frequently said during earnings calls over the past 18 months the company was getting rid of low-performing and low-margin hospitals. Smith also declared CHS was getting “attractive prices” and “very good value for the facilities that we’re selling, and we’re getting about 10 times (EBITDA) in a market for single-digit (margin) hospitals.” Smith later said “the multiple from our 30-hospital divestiture plan is approximately 12 times EBITDA.”
The gritty details: Eight of the 30 hospitals in CHS’ fire sale are in two states, Pennsylvania and Washington, that have reported financial statements to the public. And the numbers don’t line up with what Smith and Cash said. Here’s the quick synopsis of our analysis, which focused on deals that had publicly announced financial terms:
CHS had a few gripes with the analysis:
Underlying concern: Although CHS defended the statements and numbers from earnings calls, some people who follow the company believe the discrepenacies are representative of a long pattern. “There’s a history of deceptive communication practices,” said one CHS investor, who asked not to be named given the sensitivity of the issue.
What to watch for: How much debt CHS still has at the end of the third quarter, and what executives tell investors about the status of the company.
The bottom line: The “medical bills score” is the single most important measure of how we are doing in health care from the public’s perspective. And ultimately, if Congress ever passes a new health care bill, it is how the public will evaluate that plan — from Graham-Cassidy to Medicare for All and everything in between.
The numbers that matter: As we found in a Kaiser Family Foundation poll in February:
It makes sense that people who use more care have more health care bills, but it also reveals how poorly our system performs from a consumer perspective when people who need care the most are protected the least by insurance coverage.
The impact: People are not just whining about necessary cost sharing. In a survey we did with the New York Times, we found that:
Not surprisingly, the uninsured (41%) are more likely to have problems paying medical bills. But this is not a problem limited to the uninsured: 30% of the insured – think voters — have problems with medical bills.
The back story: The share of the public reporting problems paying their medical bills has not moved much in recent years. The Affordable Care Act has extended coverage and better financial protection to tens of millions, but it doesn’t have much of an impact on affordability beyond people covered by the Medicaid expansion and the marketplaces.
In the far larger employer-based health insurance sector, deductibles and other forms of cost sharing have been growing about five times faster than wages, and deductibles have been growing especially sharply for people who work for smaller employers. .
What to watch: Health care is a pocketbook issue for most of the public and the American people have their own scoring system. They may give this or that mostly partisan response about a health reform idea on a poll, but until they see how they’ll get help paying their health care bills, they will ultimately be disappointed by every health reform plan.

The opportunity and ability to step into a tipping point makes us feel responsible, powerful, and apprehensive.
Every decision both responds to and creates a tipping point.
Ease:
The pursuit of ease makes you matter less.
Ease in small doses expands capacity, but in large doses destroys us.
Please know that I’m not encouraging workaholism. However, making a difference requires getting your hands dirty.
Direction:
Every decision contributes to trajectory.
The consequence of decisions is real direction, not intended direction. You’re always heading somewhere.
Long-term or short-term:
The appeal of short-term perspectives is immediate gratification, sometimes at the expense of long-term value.
Crisis requires short-term perspective. Put the fire out! But constant “crisis mode” sacrifices the future on the altar of urgency.
Relationships:
Life is relationships, nothing more, nothing less.
Service:
Tipping points include opportunities to both receive and give value.
5 general questions:
What questions might leaders ask when facing tipping points?

Senate Republicans’ fiscal year 2018 budget resolution suggests that they have put their goal of broadly unwinding the Affordable Care Act on the back burner—yet they could still use it to repeal key parts of the law.
The budget resolution (PDF), released by Senate Budget Committee Chairman Mike Enzi, R-Wyo., on Friday, contains reconciliation instructions that direct the Senate Finance Committee to “reduce revenues and change outlays to increase the deficit by not more than $1.5 trillion over the next 10 years.”
Since that reconciliation instruction is rather broad, the GOP could potentially use it to repeal some ACA-related taxes and other provisions that make health insurance affordable under the law, argued a post from the left-leaning Center for American Progress (CAP).
With their new budget resolution, Republicans could also still roll back other portions of the ACA, including the individual mandate, a Bloomberg article noted.
But because the budget resolution doesn’t include any instructions for the Senate Health, Education, Labor and Pensions Committee or the House Energy and Commerce Committee to craft reconciliation legislation, that may indicate that broader ACA repeal efforts are on hold, The Hill reported.
In addition to the reconciliation instructions, the budget resolution includes deficit-neutral reserve funds for legislation that would allow Congress to repeal or replace the ACA. This primarily just signals rhetorical support for rolling back the healthcare law, the CAP post noted, but that’s significant since it shows the GOP isn’t giving up on repeal.

