

Tag Archives: ACA
Rolling Back the ACA’s Medicaid Expansion: What Are the Costs for States?
http://www.commonwealthfund.org/publications/blog/2017/feb/states-roll-back-aca-medicaid-expansion

Millions of people have gained health insurance coverage though the Affordable Care Act’s (ACA) Medicaid eligibility expansion, adopted by 31 states and Washington, D.C., over the past three years. Should Congress decide to eliminate or reduce federal funding for this coverage as part of ACA repeal, states that expanded will be faced with the prospect of either maintaining coverage out of their own funds or dropping the new beneficiaries from the program. Along with the loss of coverage or the creation of large budget holes, rolling back Medicaid benefits would present states with expensive and complex administrative challenges.
Were Congress to repeal federal funding for the expansion group, coverage for these newly eligible enrollees—estimated at 11 million as of 2015—inevitably would disappear. No state is in a position to support this population without considerable federal funding. For example, were ACA Medicaid expansion funding to disappear, California would lose more than 27 percent of the total federal Medicaid funding the state is projected to receive over the 2019 to 2028 time period; federal funding would drop from $364 billion to $265 billion, a $99 billion loss.
If a repeal bill retains the Medicaid expansion but reduces federal funding for the expansion group to traditional Medicaid funding levels,1 some states might seek flexibility to roll back coverage to a lower level such as 75 percent of poverty, rather than the eligibility standard used under the expansion (138 percent of poverty). Rather than terminate insurance eligibility altogether for populations without an alternative source of coverage, states also might try to trim benefits or reduce or freeze provider payments.
But even if funding is eliminated completely, federal laws place important brakes on the process. For example, federal Medicaid rules dating back decades require states to determine if there is another basis of eligibility prior to terminating coverage. At least some of the people covered as part of the expansion population may qualify for Medicaid on other grounds such as pregnancy, being the parent of a minor child, or disability.
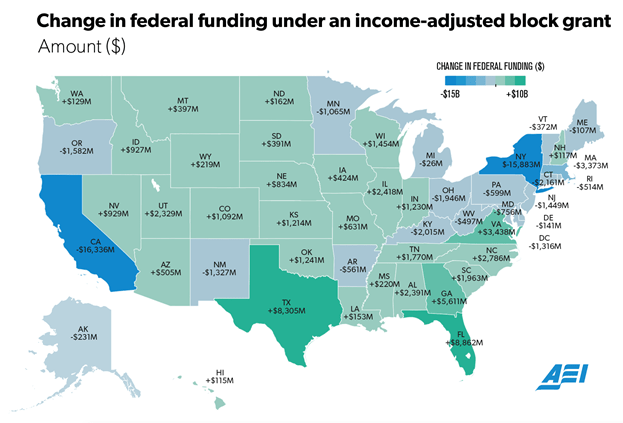
How Would Republican Plans for Medicaid Block Grants Actually Work?
How Would Republican Plans for Medicaid Block Grants Actually Work?

There are only so many ways to cut Medicaid spending.
You can reduce the number of people covered. You can reduce the benefit coverage. You can also pay less for those benefits and get doctors and hospitals to accept less in reimbursement. Or you can ask beneficiaries to pay more.
None of those are attractive options, which is why Medicaid reform is so hard. Medicaid already reimburses providers at lower rates than other insurance programs. How do you reduce the number of beneficiaries when the vast majority of people covered are poor children, poor pregnant women, the disabled, and poor older people? Which of those would you cut?
Reducing benefit coverage has always been difficult because most of the spending has been on the disabled and poor older people, who need a lot of care. Beneficiaries don’t have much disposable income, so asking them to pick up more of the bill is almost impossible.
That doesn’t mean that states haven’t tried. As I’ve discussed in past columns, a number are attempting to increase cost sharing. But this isn’t really a solution because it doesn’t change overall spending much at all.
Part of the challenge lies in the way Medicaid was set up in the first place. The federal government picks up between 50 percent and 100 percent (depending on the population and the per-person income) of whatever it costs to provide health care to a state’s population. Many, if not most, Republican plans would like to change that.
They are pushing for what many refer to as a block grant program. The federal government would give a set amount of money to each state for Medicaid; it would be up to the states to spend it however they like. These block grants could be set based on overall past state needs or based on the number of beneficiaries in the state, referred to as a “per capita” block grant. Some per-capita block grants function more like “ceilings” than outright grants, allowing the state to be paid at normal Medicaid rates, but with a maximum each state could get based on the per-capita calculation.
The feds have been ordered to cough up risk corridor money.

A judge on the Court of Federal Claims has entered a $214 million judgment against the United States in favor of Moda Health, an Oregon insurer. Moda sued to recover money owed to it under the risk corridor program, a three-year program that was supposed to protect insurers from excessive losses on the exchanges. In emphatic language, the court ordered the government to pay up.
The Court finds that the ACA requires annual payments to insurers, and that Congress did not design the risk corridors program to be budget-neutral. The Government is therefore liable for Moda’s full risk corridors payments under the ACA. In the alternative, the Court finds that the ACA constituted an offer for a unilateral contract, and Moda accepted this offer by offering qualified health plans on the [exchanges]. …
Today, the Court directs the Government to fulfill [its] promise. After all, “to say to [Moda], ‘The joke is on you. You shouldn’t have trusted us,’ is hardly worthy of our great government.” Brandt v. Hickel, 427 F.2d 53, 57 (9th Cir. 1970).
http://www.nejm.org/doi/full/10.1056/NEJMp1612486#t=article
Everything You Need to Know About Block Grants: The Heart of GOP’s Medicaid Plans

President Donald Trump’s administration made explicit this weekend its commitment to an old GOP strategy for managing Medicaid, the federal-state insurance plan that covers low-income people — turning control of the program to states and capping what the federal government spends on it each year.
It’s called “block granting.” Right now, Medicaid, which was expanded under the 2010 health reform to insure more people, covers almost 75 million adults and children. Because it is an entitlement, everyone who qualifies is guaranteed coverage and states and the federal government combine funds to cover the costs. Conservatives have long argued the program would be more efficient if states got a lump sum from the federal government and then managed the program as they saw fit. But others say that would mean less funding for the program —eventually translating into greater challenges in getting care for low-income people.
Block granting Medicaid is a centerpiece of health proposals supported by House Speaker Paul Ryan and Rep. Tom Price, Trump’s nominee to run the Department of Health and Human Services. This weekend, Trump adviser Kellyanne Conway emphasized the strategy as key to the administration’s health policy.
But what would this look like, and why is it so controversial? Let’s break down how this policy could play out, and its implications — both for government spending and for accessing care.
Q: How would a block grant work?
Medicaid Reform: The Elephant in the Room
While headlines fixate on the future of the Affordable Care Act’s health insurance exchanges, a more consequential fight is brewing over the future of Medicaid. Proposed reforms would affect tens of millions of Americans and state governments across the country. Previous attempts have failed, however, and longstanding roadblocks may sink this administration’s efforts as well.
With over 70 million enrollees, Medicaid covers more Americans than any other insurer. Responsibility for funding the program – which accounts for nearly 20 percent of all healthcare spending – is shared between states and the federal government. At a minimum, the federal government covers 50 percent of costs, with that share rising to nearly 75 percent in the poorest states and more than 90 percent for those covered through ACA Medicaid expansions. This amounts to nearly $350 billion in federal funding per year.
Importantly, this money is allocated in an open-ended manner. As states increase the generosity of their Medicaid programs, the federal government is obliged to pay its portion of the higher costs.
During his campaign, Donald Trump joined a long list of Republican lawmakers who argue that this gives states the wrong incentives. Because the federal government covers at least half of each dollar spent, they argue, states may take less care to weed out inappropriate and inefficient spending as they otherwise would.
To eliminate this open-ended feature, Trump’s plan calls for federal money to be allocated in fixed lump sum payments known as block grants.
First proposed in 1981 by President Reagan, block granting of Medicaid hardly represents a novel policy option. Why then has the current system endured, and what does this portend for the resistance Trump’s efforts may encounter?
To understand, consider the most basic decision for any block grant policy: How should each state’s grant be initially determined?
Conservatives Urge Speed Up Of Health Law Repeal, Dismiss Calls for Caution
![]()
Leading conservative Republicans from the House and Senate say Congress is moving too slowly on efforts to “repeal and replace” the Affordable Care Act. But their potential resistance to compromise — even with other members of their own party — underscores just how hard a task Republicans have set for themselves.
“We think it’s time to do something, and that’s to get rid of this law,” Rep. Jim Jordan, R-Ohio, told reporters at an event sponsored by the conservative Heritage Foundation. “The biggest problem with waiting is that’s not what we told the voters.”
Sen. Mike Lee, R-Utah, one of the leading conservative voices in that chamber, said he will vigorously oppose efforts for Republicans to wait until they have a plan ready to replace the law before they repeal it. “There is a lot less agreement about what comes next,” he said. “If we load down the repeal bill with what comes next, it’s harder to get both of them passed.”
After getting off to a quick start, GOP efforts to dismantle the health law appear to have slowed considerably. House and Senate committees have already missed a deadline of Jan. 27 to write and pass their proposed repeal and replace provisions, although Senate leaders acknowledged early this year that marker would likely not be met. At a party retreat last month, Republicans still seemed uncertain exactly how and when they would proceed.
And in an interview that aired just before the Super Bowl, President Donald Trump for the first time acknowledged that the effort to remake the health law could last into next year.
Conservatives, however, are pushing back.
Since the Election, Americans Grow More Supportive of ACA

There are now more people who think Obamacare is a good idea than those who don’t. It’s basic human nature: People tend to get upset if they think they are about to lose something they feel entitled to or previously had. It’s also the idea that fueled Donald Trump’s electoral base, and ironically, now fuels those who are opposed to him.
Centene to stay on ACA exchanges; WellCare grows Medicaid membership

Unlike some of the other major for-profit health insurers, Centene has no plans to consider exiting the Affordable Care Act exchanges in 2018.
“I’m not backing off at all,” CEO Michael Neidorff said during the company’s fourth-quarter earnings call Tuesday. In recent discussions with the company’s board members, he said, “everybody is of one mind; you maintain business as usual.”
Recently, the CEOs of Anthem and Cigna both indicated they are still deciding whether to participate on the exchanges in 2018. Aetna, meanwhile, does not plan to re-enter any markets in 2018 after pulling out of many in 2017.
As of Dec. 31, Centene served about 540,000 exchange members, in line with its expectations, and it anticipates having a little more than 1 million paid members in 2017. Indications are that the demographics of these members will be consistent with years past, with 90% of them subsidy-eligible and most on silver-tier plans, Neidorff said.
While Centene is folding an “extra level of conservativism” into its expectations for its exchange products to guard against any uncertainty, it continues to expect that line of business to be profitable this year, he added.
Another ACA provision, Medicaid expansion, has also proved profitable for Centene. At the end of 2016, it had 1,080,500 members in Medicaid expansion programs in 10 states, compared to 449,000 members at the end of 2015, according to the company’s earnings statement.
Is 3.49 more than 3?

HHS has already submitted a proposal of new rules to OMB. [Under the proposal,] insurers would have more leeway to vary prices by age, so that premiums for the oldest customers could be 3.49 times as large as those for younger customers. Today, premiums for the old can be only three times as high as premiums for the young, which is what the Affordable Care Act stipulates. According to sources privy to HHS discussions with insurers, officials would argue that since 3.49 “rounds down” to three, the change would still comply with the statute.
This is kinda dumb. It’s also not so legal. The ACA says that “the rates” for health plans “shall not vary by more than 3 to 1 for adults.” The statute couldn’t be clearer. As I said to Jonathan: ”If I told you not to sell something for more than $3.00, and you went ahead and sold it for $3.49, then you’ve disregarded my instruction. It doesn’t matter if it rounds to $3.00. It’s more than $3.00.”
Under Chevron, agencies have lots of room to interpret ambiguous statutes. But there’s no ambiguity here. The statute says no more than 3, period. As Monty Python might say, 3.49 is right out. (Here’s where I insert the standard caveat that the administration hasn’t offered a legal argument—or any public comment, for that matter—and it’s possible I’m missing something. Also, the rule could easily be amended during OMB review.)
