https://www.healthleadersmedia.com/first-time-employed-docs-outnumber-self-employed-docs

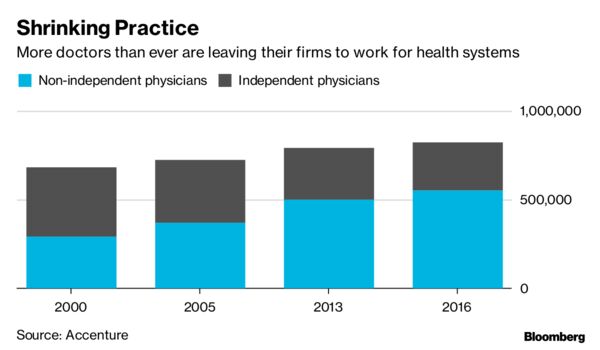
The milestone continues a long-term trend that has shifted the distribution of physicians away from ownership of private practices.
KEY TAKEAWAYS
Employed physicians were 47.4% of all patient care physicians in 2018, up 6% points since 2012.
Self-employed physicians were 45.9% of all patient care physicians in 2018, down 7% points since 2012.
In the aggregate, 34.7% of physicians worked either directly for a hospital or in a practice at least partly owned by a hospital in 2018, up from 29.0% in 2012.
Employed physicians outnumber self-employed physicians for the first time in the United States, according to an updated study on physician practices by the American Medical Association.
“Transformational change continues in the delivery of healthcare and physicians are responding by reevaluating their practice arrangements,” AMA President Barbara L. McAneny, MD, said in a media release.
Employed physicians were 47.4% of all patient care physicians in 2018, up 6% points since 2012.
Self-employed physicians were 45.9% of all patient care physicians in 2018, down 7% points since 2012.
Such a dramatic shift is not unprecendented. Older AMA surveys show the share of self-employed physicians fell 14% points during a six-year span between 1988 and 1994.
Given the rate of change in the early 1990s, it appeared a point was imminent when employed physicians would outnumber self-employed physicians, but the shift took much longer than anticipated.
The AMA’s researchers said that history suggests that “caution should be taken in assuming current trends will continue indefinitely.”
The majority of patient care physicians (54%) worked in physician-owned practices in 2018 either as an owner, employee, or contractor. Although this share fell from 60% in 2012, the trend away from physician-owned practice appears to be slowing since more than half of the shift occurred between 2012 and 2014, the study said.
At the same time, there was an increase in the share of physicians working directly for a hospital or in a practice at least partly owned by a hospital.
Physicians working directly for a hospital were 8% of all patient care physicians, an increase from 5.6% in 2012. Physicians in hospital-owned practices were 26.7% of all patient care physicians, an increase from 23.4% in 2012.
In the aggregate, 34.7% of physicians worked either for a hospital or in a practice at least partly owned by a hospital in 2018, up from 29.0% in 2012.
Younger physicians and women physicians are more likely to be employed. Nearly 70% of physicians under age 40 were employees in 2018, compared to 38.2% of physicians age 55 and over.
Among female physicians, more were employees than practice owners (57.6% vs. 34.3%). The reverse is true for male physicians, more were practice owners than employees (52.1% vs. 41.9%).
As in past AMA studies, physicians’ employment status varied widely across medical specialties in 2018.
The surgical subspecialties had the highest share of owners (64.5%) followed by obstetrics/gynecology (53.8%) and internal medicine subspecialties (51.7%).
Emergency medicine had the lowest share of owners (26.2%) and the highest share of independent contractors (27.3%). Family practice was the specialty with the highest share of employed physicians (57.4%).
Most physicians still work in small practices, but this share has fallen slowly but steadily since 2012. In 2018, 56.5% of physicians worked in practices with 10 or fewer physicians compared to 61.4% in 2012.
The AMA report said the transition has been driven primarily by the shift away from very small practices, especially solo practices, in favor of very large practices of 50 or more physicians.
The new study is the latest addition to the AMA’s Policy Research Perspective series that examines long term changes in practice arrangements and payment methodologies.
“Transformational change continues in the delivery of healthcare and physicians are responding by reevaluating their practice arrangements. ”