https://www.managedhealthcareexecutive.com/healthcare-leadership/biggest-growth-opportunities-healthcare?rememberme=1&elq_mid=5658&elq_cid=876742&GUID=A13E56ED-9529-4BD1-98E9-318F5373C18F

Healthcare growth opportunities for 2019 should pivot around the three big themes: digital transformation, value-based care, and patient-centricity, according to a new report.
According to Frost & Sullivan’s report, “Global Healthcare Market Outlook, 2019,” digitization of products, services, and commerce models are democratizing current healthcare systems, manifesting a new era of healthcare consumerism.
“Now the new vision for healthcare is not just about access, quality, and affordability but also about predictive, preventive, and outcomes-based care models promoting social and financial inclusion,” says Kamaljit Behera, transformational health industry analyst at Frost & Sullivan, and author of the report. “This makes digital transformation and realization of long-pending policies reform a key growth priority for healthcare executives and major health systems during 2019 globally.”
According to Behera, increasing pricing pressure and shifting the focus of the healthcare industry from a volume- to value-based care model demands that drug and device manufacturers elevate their business models beyond products to customer-centric intelligent platforms and solutions.
“In 2019, the healthcare market will continue to transit and stick into the value-based model,” Behera says. “More sophisticated outcomes-based models will get deployed in developed markets, and emerging nations will start following the best practices suited to their local needs.”
Despite the promise of digital transformation, the potential promise and actual commercial application still remain the poles apart from some of the most touted technologies like AI and blockchain, according to Behera.
“Current technology is often perceived to increase the barriers between patient and providers,” he says. “In order to bridge these gaps, healthcare executives need to change the debate around digital transformation and start look beyond the mirage of technology novelty and really focus on the outcomes.”
Behera predicts that these five areas will be the biggest areas of growth for healthcare in 2019:
1. Meaningful small data
Healthcare data analytics focus will shift from ‘big data’ to ‘meaningful small data’ by hospital specialty, according to Behera. “Increasing digitization of healthcare workflows is leading us to a data explosion along the care cycle, globally,” he says. “This makes insights generation from existing healthcare data for targeted use cases a relatively low-hanging opportunity relative to other emerging technologies. Additionally, health data being the ‘holy grail,’ the analytics solutions are considered the first foundational step to catalyze complementing technology promises leveraging healthcare data (e.g., artificial intelligence, cloud computing, and blockchain).”
Entailing this, Frost & Sullivan research projects the healthcare analytics market revenue to cross $7.4 billion in the United States by the end of 2020.
“The key pivotal theme driving this growth opportunity includes population health management, financial performance improvement, and operational automation by patients, payers, physicians, and procedures,” Behera says. “Also, the rise of value-based care and outcomes-based reimbursement programs will continue to boost the demand for specialized analytics solutions.”
In 2019, payers and providers will continue to prioritize and leverage the potential of specialty-specific analytics solutions to investigate drug utilization, treatment variability, clinical trial eligibility, billing discrepancy, and self-care program attribution specific to major chronic conditions, according to Beherea.
2. Digital health coming of age with increased focus on individual care
“During 2019, we project application of digital health will continue to go far beyond the traditional systems and empower individuals to be able to manage their own health,” Behera says.
Favorable reimbursement policies (e.g., toward clinically relevant digital health applications) will expand care delivery models beyond physical medicine to include behavioral health, digital wellness therapies, dentistry, nutrition, and prescription management, according to Behera.
“For example, major insurance bodies are already using digital health services to communicate with patients,” he says. “Traditionally, lack of formal reimbursement processes is actually a deterrent to the uptake of these—wearables, telehealth etc. The next 12 months will see a relaxation of reimbursement rules for digital health solutions.”
The global aging population and an expanding middle class are major contributors to the chronic disease epidemic and surging healthcare costs, Behera says. “This year will be a pivotal year for defining value for healthcare innovation and technology for digital health solutions catering to aged care and chronic conditions management to bending healthcare cost curve,” he says.
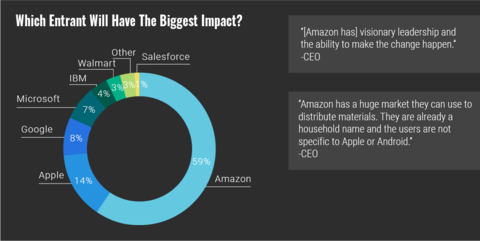
“Telemedicine in emerging markets will become more mainstream and will aim to become a managed services provider [rather] than being just a telemedicine platform,” he says. “Telemedicine will move into the public health space as well, with countries like Singapore is testing the platforms in a regulatory sandbox. Finally, as the lines between retail, IT, and healthcare continue to blur, non-traditional players such as Amazon, Apple, Google, Ali Health, Microsoft, and IBM, among others, will continue to make further headway into the individual care space— providing the required impetus to public health systems to ensure accessibility and affordability of care-leveraging, patient-centric digital health tools and solutions.”
Healthcare executives should prioritize their roadmap for growing IoMT and connected health ecosystems (device-, wearables-, and mHealth-generated individual health data) in order to monetize these new sources of innovation and service-oriented future revenue streams, according to Behera. “The future focus should shift from drug and device mind-set to intelligent solutions/services, demonstrating outcomes-based health benefits to individuals and their caregivers,” he says.
3. AI
In next 12 to 18 months, the priority will be to bring AI/cognitive platform technology use cases closer to clinical care to augment the physicians and even patients with actionable decision-making ability, according to Behera. “In next two to three years, AI will become a common theme across all digital initiative and platforms.”
AI-based work flow optimization use cases will represent more than 80% of the workflow market contribution. These include:
- The elimination of unnecessary procedures and costs
- In-patient care and hospital management
- Patient data and risk analytics
- Claim processing
- Optimizing the drug discovery process
“For example, Google is already at work to use machine learning for predicting patients’ deaths, and the results boast a flattering figure of 95% accuracy, which is better than hospitals’ in-house warning systems,” says Behera. “AI application across clinical and non-clinical use cases will continue to show hard results and further bolster the growth in the healthcare space in 2019.”
AI-powered IT tools that manage payers’ and providers’ business risks (including clinical, operational, financial, and regulatory) continue to be important for the market, according to Behera. “Across all regions in the world, AI-based cognitive technologies are proving to be the most useful for medical imaging and clinical diagnostics—as a decision-support tool—followed by AI application to derive intelligence on remote patient monitoring data to promote outcomes-based personalized care.”
4. Regenerative medicine
Cell-gene therapy combinations are rapidly gaining momentum, which make use of gene-editing tools and vector delivery systems to devise innovative curative therapies, according to Behera.
“There is also a pipeline of induced pluripotent stem cells (IPSCs), mesenchymal stem cells (MSCs), and adipose-derived stem cells (ADSCs) for novel therapeutic treatments for neurological, musculoskeletal, and dermatological conditions, among others,” he says.
These are poised for growth because rising pressures to decrease healthcare cost globally, the emergence of value-based reimbursement models, and healthcare digitization trends are transitioning the treatment model from “one-size-fits-all” to stratified and outcomes-based targeted therapies, according to Behera.
“Many factors determine the rate at which the stem cell therapy market advances,” he says. “It is driven by the success of stem cell treatments in curing life-threatening diseases such as cancer, heart diseases and neuromuscular diseases in the world’s aging populations. Emerging gene-editing techniques such as CRISPR/Cas9 that offer high precision, accessibility, and scalability, compared to other genome editing methods, such as ZFNs and TALENs for cell and gene therapy applications will continue to attract high investment both from venture capital and pharma companies.”
As regenerative medicine is redefining medical technology synergies by combining stem cell technology with tissue engineering, market participants should be investing in innovative models such as risk sharing, in-licensing/out-licensing deals, fast-to-market models, and in-house expansions, according to Behera.
“With cell-therapy manufacturing being time sensitive, biopharma companies should implement IT-based solutions for improved manufacturing capabilities,” he says. “Despite the promises with novel cell and gene therapies such as CRISPR/Cas9, questions around ethical application challenge its future potential. This makes it necessary for the life science research executives to work closely with regulators in developing guidelines and regulations [that will] guide ethical and real-word unmet needs of the healthcare industry.”
5. Digital therapeutics
“Digital therapeutics are about to become a true medical alternative that will utilize communication-based technologies, apps, and software to improve patient outcomes and help to lower the cost of healthcare,” Behera says. “Digital therapeutics offer the benefit to improve patient outcomes and reduce treatment cost by replacing the need for a drug or augmenting a standard of care, but they are not endorsed by a regulatory body, such as the FDA.”
Frost & Sullivan projects that the overall digital therapeutics market is to grow at a CAGR of 30.7% from 2017 to 2023.
“Digital therapeutics will become an exciting healthcare option that adds a curative dimension to technology,” he says. “As care for these chronic diseases expands in scope, prevention and recovery are becoming the new focus areas—apart from diagnosis and treatment. This demands a holistic view of individual health, lifestyle, and environmental data beyond the clinical health records to efficiently stratify at-risk patients for a preventive and targeted treatment paradigm.”
Defining digital therapeutics appears at first glance to be a simple task, but challenges develop when attempting to define digital therapeutics as a market opportunity, according to Behera.
“Healthcare executives exploring the growth opportunities should prioritize their market positioning, which is often dictated by focused use cases (e.g., condition management vs. behavior management) rather than the technology novelty,” he says. “At present, many companies are either claiming to be or cited in the media as digital therapeutics, but only a small number of early-stage participants are seeking FDA certification based on randomized clinical trials. They make it critical for healthcare executives to keep a close watch on progressing regulatory developments, such as the FDA precertification program.”












{kind=link}