According to the DOJ, this is the ninth consecutive year that the organizations’ civil healthcare fraud settlements and judgments have exceeded $2 billion.
As part of the federal government’s increasing focus on issues of healthcare fraud, particularly in the Medicare space, the U.S. Department of Justice recovered $2.5 billion in settlements and judgments from False Claims Act Cases over the past year.
According to the DOJ, this is the ninth consecutive year that the organizations’ civil health care fraud settlements and judgments have exceeded $2 billion.
While the $2.5 billion number represents federal losses, the DOJ also said it also helped recover significant funds for state Medicaid programs
“Every year, the submission of false claims to the government cheats the American taxpayer out of billions of dollars,” Principal Deputy Associate Attorney General Jesse Panuccio said in a statement.
“In some cases, unscrupulous actors undermine federal healthcare programs or circumvent safeguards meant to protect the public health … The nearly three billion dollars recovered by the Civil Division represents the Department’s continued commitment to fighting fraudsters and cheats on behalf of the American taxpayer.”
The False Claims Act has its roots in groups trying to defraud the military during and after the Civil War and was significantly strengthened since 1986 when Congress increased incentives for whistleblowers to file lawsuits alleging false claims.
In healthcare, organizations across the industry were hit with False Claims cases including drug companies, medical device manufacturers, payer organizations and healthcare providers.
The single largest recovery over the past year was a $625 million settlement paid by drug wholesaler AmerisourceBergen to resolve a number of claims including that the company illegally repackaged injectable cancer drugs into pre-filled syringes and billing multiple doctors for individual drug vials.
The DOJ also brought cases against drug companies who increased drug prices by funding Medicare co-payments meant to serve as a check on healthcare costs.
One major case against Massachusetts-based medical device company Alere resulted in a $33.2 million settlement over allegations that it sold unreliable diagnostic devices meant to detect acute coronary syndromes, heart failure, drug overdose and other serious conditions.
When it comes to health plans, the government’s case against UnitedHealth Group over allegations that it knowingly obtained inflated risk adjustment payments for its Medicare Advantage beneficiaries is still ongoing.
Healthcare providers know that inpatient volumes are down over historic levels. (But let’s not talk […]
Healthcare providers know that inpatient volumes are down over historic levels. (But let’s not talk about emergency department volumes—those are WAY up.) They know this trend originates mostly with Medicare beneficiaries. They also know the causes: migration to outpatient services, observation day rules, intense focus on decreasing length of stay, and reduced readmissions as part of their quality initiatives.
What they may miss, however, is that this trend also has something to do with the declining average age of our nation’s senior population—a phenomenon that first began in 2005 and will continue until about 2020. In 2005, the average age of our nation’s senior population was 75.2 years; in 2020, the average age is expected to be 74.4 years.
This fact is important because older seniors consume significantly greater healthcare resources than younger seniors. Today, those over 65 represent about 15 percent of the total U.S. population. By 2020, one out of six Americans will be 65 or older, rising to 22 percent by 2040. Understanding how this population is distributed among age cohorts is critically important not only in understanding current trends in reduced utilization, but also in preparing for the future.
Taking a Closer Look
This increasing proportion of the population that are seniors is important because the average Medicare beneficiary consumes about four times the hospital-based services as the average commercially insured person. But it is just as important to look more closely at consumption patterns within the senior population. Those between ages 75 and 84 consume about 60 percent more services than seniors ages 65 to 74. Those age 85 and above consume about two-and-a-half times as much.
According to U.S. Census forecasts, in 2021, the over-75 population will make up the lowest percentage of the senior Medicare population in recent history, at about 41 percent. By 2040, seniors older than 75 will constitute 55 percent of the total senior population. This fact alone would suggest that we are in for a reversal of declining volume patterns—but by how much?
The answer is that if nothing is done to further reduce admissions and days per 1,000 for the senior Medicare population, inpatient days should almost double from about 70 million today to about 130 million in 2040 on the basis of demographic changes alone. That represents a need for some 220,000 additional beds at 75 percent capacity by 2040—never mind all the other healthcare services that will be needed. But even as there is general recognition among healthcare leaders of the advent of an aging population, there is also the general sense that somehow, we will not need the same level of resources to meet that demand as we do today.
Where does that sense of assurance come from? Apparently, it stems from the belief that unnecessary and excess utilization exists purely due to financial reasons, and that even more of the care delivered on an inpatient basis could be performed on an outpatient basis or at home with better monitoring and intervention through new technologies. But there also appears to be an ignoring of the well-known trend for the population becoming increasingly co-morbid at ever-younger ages. Additionally, some believe that increased focus on addressing social determinants of health, which impact 64 percent of health outcomes, will reduce need for medical services.
All of these assumptions may be true, in theory. In practice, however, as a senior healthcare executive and registered nurse said to me recently, “People are really sick. You have no idea.” There is also the enormous question of how one staffs and gets paid for programs and investments that might reduce demand for hospital-based services. The economics of today’s medicalized approach to health care is unprepared to address this.
A Critical Issue for Leadership This is an issue that should be of paramount importance to healthcare providers. As seniors comprise a greater portion of our population, demand for inpatient and post-acute services will significantly increase. The hope and dream expressed in the view that hospital-based utilization might be reduced springs from a terrible reality: Hospitals in general, with the possible exception of high-end tertiary/quaternary services, lose money on government-reimbursed volume—and this will only get worse as cost inflation continues to exceed government reimbursement trends.
The prospect of the demand for inpatient days nearly doubling over the next 20 years paints a horrifying financial picture. Who, then, would not want to hope that something magical will happen to prevent a scenario that logic and data tell us is likely to occur?
It’s time for healthcare leaders to take a hard look at the trends around senior aging and have tough discussions with their executive teams and boards about the impact these trends could have on their organizations’ futures—and what they should be doing now to prepare.
Across December we have been sharing our framework for helping health systems rethink their approach to investment in delivery assets, built around a functional view of the enterprise. We’ve encouraged our clients to take a consumer-oriented approach to planning, starting by asking what consumers need and working backward to what services, programs and facilities are required to meet those needs. That led us to break the enterprise into component parts that perform different “jobs” for the people they serve. We think of each of those parts as a “business”, located at either the market, regional or national level depending on where the best returns to scale are found (and on the geographic scale of any particular system). First we shared our view of the “access business”, pushing systems to create a broad web of access points across their market, with the goal of building consumer loyalty over time. Last week we described our vision for the “senior care” business, where an array of assets traditionally providing postacute care, including rehabilitation and skilled nursing facilities (SNFs), home health, and even hospital-at-home programs, could expand their capabilities to manage chronic disease exacerbations in elderly patients in lower-acuity, lower-cost settings. This week we’ll describe how the changes in these outpatient care settings will affect the profile of the traditional acute care hospital. Shifting demographics will dramatically change the patient mix of American hospitals across the next decade. As Baby Boomers age into their Medicare years, ED and hospital beds will fill with elderly patients admitted for exacerbations of chronic diseases like congestive heart failure and diabetes, their care reimbursed at public-payer rates. Over time it’s easy to imagine hospitals starting to look like giant SNFs, filled with elderly patients receiving nursing care and drugs. With current cost and labor structures, this shift will be financially unsustainable for hospitals, as Medicare payment for many medical admissions does not cover the cost of the inpatient admission, forcing hospitals to pursue alternative care settings for these patients. As we described last week, as many as half of chronic disease admissions could be managed by an expanded “senior care” platform. Adding to this potential shift of medical admissions to an outpatient setting, we anticipate that an expanded postacute and home care platform could also accelerate the shift of inpatient surgeries to an ambulatory setting. If surgery centers could manage patients for 24- to 48-hour stays, and hospital-at-home capabilities supported recovery at home, some experts believe that a majority of non-emergent inpatient surgeries—including many orthopedic and general surgery cases—could shift away from the hospital. If this shift to alternative settings bears out, demand for traditional “med-surg” beds could decline significantly, even in the face of demographic shifts. The graphic below describes an alternative vision for the future acute-care hospital that takes into account these changes. This “hospital of the future” will be asset-light, focused on providing higher levels of emergency, medical and surgical care, with capacity weighted toward more intensive patient management. The acute care facility will be supported by a network of connected and expanded ambulatory resources, including outpatient surgery, postacute services, home care and access services, all enabled by remote monitoring technology. While payment changes covering expanded outpatient care will accelerate this movement, we believe that payer and patient mix shifts alone will provide motivation for hospitals to pursue these strategies. The cost of adding a new med-surg bed now tops $2M in most markets—trimming even a few beds that may not be needed will provide capital that can go a long way in expanding outpatient capabilities to support lower-acuity care.
Mobile health records and nurse protests also grabbed readers this year.
This year in healthcare was marked by sweeping changes, including seemingly constant vertical and horizontal consolidation, led by the $69 billion CVS grab of Aetna and Cigna’s $67 billion acquisition of Express Scripts.
As 2018 wound down, a federal judge took an ax to the Affordable Care Act as the Trump administration kept up its efforts to undermine the law, with CMS expanding short-term health plans many say are built to subvert the ACA. Elimination of the individual mandate penalty, Medicaid expansion and rising premiums all likely contributed to declined enrollment on ACA exchanges as well.
The administration encouraged states to use waivers to expand controversial Medicaid work requirements and proposed site-neutral payments, rattling health systems of all sizes that were already struggling under ferocious operating headwinds. Hospitals cut back on services and invested heavily in lucrative outpatient facilities in an attempt to reclaim volume.
Tech companies Apple and Amazon pushed further into the space, with the former focusing on mobile health apps and the latter focusing on, well, almost everything.
But that’s just scratching the surface. Here is a curated list of Healthcare Dive’s top stories from the last year.
Some smart observers saw a predecessor to these unions in UnitedHealth Group’s Optum: a pharmacy benefit manager plus a care services unit that employs over 30,000 physicians, using data analytics to capitalize on consumerism and value-based care.
Our piece on Optum’s solid foothold in the space, and its likelihood of staying ahead of the nascent competition, was Healthcare Dive’s most-read article in 2018. Read More »
A novel Medicare Advantage rule giving payers more flexibility to sell supplemental benefits to chronically ill enrollees sparked a fair amount of interest in our readers.
The rule offered up a slate of new opportunities for insurers such as UnitedHealthcare and Humana that can now work with rideshare companies to provide transportation to medical appointments, air conditioners for beneficiaries with asthma and other measures around issues like food insecurity in a broad shift to recognizing social determinants of health. Read More »
Outside players such as Apple, Amazon and Google moved forward in their bids to disrupt healthcare in 2018. Apple rang in the New Year with its announcement that customers would now be able to access their medical records on the Health app following months of speculation and buzz.
The move looks to put access to personal, sensitive data back in the patients’ hands, an objective a lot of the entrenched healthcare ecosystem can get behind as well. Heavy hitters on the EHR side (Epic, Cerner, athenahealth) and the provider side (Johns Hopkins, Cedars-Sinai, Geisinger) are taking place in the initiative. Read More »
At least 14 states have legislation addressing safe staffing currently, but California is the only one to implement a strict ratio at one nurse per every five patients. Looking to 2019, in Pennsylvania voters elected a governor who has voiced support for state legislation. Read More »
Employers ramped up their cost-containment creativity in 2018. One method? Cutting out the middleman and forging direct relationships with providers themselves, whether it’s contracting with an accountable care organization to manage an entire employee population or a simple advocacy role to fight for payment reform.
Although only 6% of employers are doing so currently, 22% are considering solidifying some sort of provider relationship for next year according to a Willis Towers Watson survey. It’s also likely the Amazon-J.P. Morgan-Berkshire Hathaway venture will look at direct contracting in its (still vague) mission to lower employer costs. Read More »
Under intense operating headwinds, supply chain professionals looked to trim the fat from traditional distribution and supplier models in 2018. Some looked to Amazon Business, which generated more than a billion dollars in sales its first year alone by relying on its marketplace model, streamlined ordering and a “tail spend” strategy.
Healthcare Dive discussed this and more with global healthcare leader at Amazon Chris Holt in an exclusive interview that drove a lot of interest. Read More »
Value-based care was a buzzword over the past year, with providers, payers and healthcare execs across the board looking (or saying they’re looking) for ways to cut costs and improve quality.
Although legal barriers stemming from the Anti-Kickback Statute and Stark Law persist, medical technology companies jumped on the bandwagon, with big names like GE, Philips and Medtronic coupling with hospitals to promote VBC initiatives. Read More »
The combination of the e-commerce giant, a 200-year-old multinational investment bank and Warren Buffet’s redoubtable holding company joining forces to take on healthcare costs spooked investors in traditional industry players. The venture added a slew of big names to its C-suite, including Atul Gawande and Jack Stoddard for CEO and COO, respectively. Read More »
We learned that when hospitals combine, patients can end up paying more.
Everywhere in the United States, hospitals are merging. Instead of creating savings that get passed on to consumers, an analysis found that in some regions, the opposite occurred. From 2010 through 2013, the price of an average hospital stay soared, with prices in most areas going up between 11 percent and 54 percent.
We learned how one city has started to turn the corner on the opioids epidemic.
Dayton, Ohio, had one of the highest opioid overdose death rates in the nation. Now, it may be at the leading edge of a waning phase of the epidemic. While the data are preliminary, a variety of factors contributed to the reduction in deaths: Medicaid expansion paying for treatment; dwindling availability of one particular drug; greater use of naloxone, which can reverse overdoses; a large network of recovery support groups; and, law enforcement and public health workers improving their coordination.
We learned the disease may no longer be “a lifelong thing,” as one patient put it.
People with hemophilia, the inability to form blood clots, spend their lives menaced by the prospect of uncontrolled bleeding into a muscle or joint, or even the brain. Experimental gene therapy treatments have rid a few patients — for now, at least — of the condition. It does not yet amount to a cure, and the treatment is imperfect. But some who received the treatments are finding themselves uneasily adjusting to a life with new freedoms.
We learned untreated strep throat leads to heart failure in poor countries.
In the United States and other rich countries, cheap antibiotics cure children with strep throat easily. But in poor countries, strep can result in rheumatic heart disease and a long, slow death sentence. In Rwanda, doctors from a group called Team Heart visit once a year to perform heart valve-replacement surgery for 16 people. But there are thousands more people who need the procedure in a country that has no heart surgeons.
We learned how public health research can be compromised by private interests.
In June, the National Institutes of Health shut down a study of the effects of moderate drinking on heart attacks and stroke, following an investigation by The Times. The researchers who proposed the study sought funding from beer and liquor companies, and suggested that the results would support a daily drink as a healthy choice. The N.I.H.’s director, Dr. Francis Collins, said the trial seemed to be “set up in a way that would maximize the chances of showing a positive effect of alcohol.”
The National Labor Relations Board (NLRB) is preparing to prosecute health system Kaiser Permanente for refusing bargain with SEIU United Healthcare Workers West, according to the union. SEIU-UHW, part of the Coalition of Kaiser Permanente Unions, filed a complaint with the NLRB in the spring charging Kaiser for refusing to negotiate a new contract that covers 85,000 employees across eight states and D.C. Hearings for case will likely begin in the spring.
In their complaint, SEIU-UHW and the Coalition of Kaiser Permanente Unions claimed Kaiser tried to set conditions on bargaining that would ban unions from engaging in political action that could affect the healthcare organization. Kaiser issued a statement last week arguing the delay was due to a split that occurred within the coalition earlier this year, and said it is “confident the NLRB will agree that Kaiser Permanente has acted lawfully and in good faith” in dealings with SEIU-UHW.
That may not be the case. SEIU-UHW is planning on proposing a new arrangement. If Kaiser doesn’t agree to enter into that settlement proposed by the union, the NLRB is expected to issue charges by the end of the month — if not sooner, according to an email obtained by Healthcare Dive.
Dive Insight:
Kaiser has been wracked with labor woes this year. The health system reached an agreement with the Alliance of Health Care Unions — the 21 unions that broke off from the Coalition of Kaiser Permanente Unions — earlier this year. That split occurred the day before bargaining was scheduled to begin, and negotiations with the coalition did not move forward.
That contract, according to SEIU-UHW, included a condition prohibiting those unions from taking any kind of political action against Kaiser, including ballot initiatives, legislation or public policy campaigns. That’s the same condition that led SEIU-UHW to file its complaint earlier this year.
“The Coalition of Kaiser Permanente Unions strongly opposes such a proposal,” SEIU-UHW said in a statement, “and believes this condition violates their free speech rights.”
Healthcare Dive reached out to the NLRB for confirmation on its reported decision to prosecute Kaiser, but did not receive a response in time for publishing.
“The decision confirms what has been clear to workers for months now: Kaiser isn’t the labor friendly employer it claims to be, nor is it as committed to patient care as it claims to be,” Lanette Griffin, a laboratory assistant at Kaiser Permanente, said in a statement. “If Kaiser was committed to improving patient care, you would expect it to want to negotiate a contract to retain and attract the outstanding caregivers who have driven the corporation’s success. But Kaiser is showing its true colors when it avoids bargaining and wants to silence our voices.”
Last week, 4,000 mental health workers represented by National United Healthcare Workers engaged in a five-day strike against Kaiser, causing the system to postpone some surgeries. Kaiser has attributed the cancellations to California Nurses Association nurses joined the picket line in an authorized sympathy strike.
“The determination by the district 32 office of the National Labor Relations Board is not a verdict. It is the beginning of the NLRB’s process to hold evidentiary hearings to fully understand this complicated case,” Kaiser said in its statement.
“In my whole life, I have known no wise people (over a broad subject matter area) who didn’t read all the time — none. Zero.”
— Charlie Munger, Self-made billionaire & Warren Buffett’s longtime business partner
Why did the busiest person in the world, former president Barack Obama, read an hour a day while in office?
Why has the best investor in history, Warren Buffett, invested 80% of his time in reading and thinking throughout his career?
Why has the world’s richest person, Bill Gates, read a book a week during his career? And why has he taken a yearly two-week reading vacation throughout his entire career?
Why do the world’s smartest and busiest people find one hour a day for deliberate learning (the 5-hour rule), while others make excuses about how busy they are?
What do they see that others don’t?
The answer is simple: Learning is the single best investment of our time that we can make. Or as Benjamin Franklin said, “An investment in knowledge pays the best interest.”
This insight is fundamental to succeeding in our knowledge economy, yet few people realize it. Luckily, once you do understand the value of knowledge, it’s simple to get more of it. Just dedicate yourself to constant learning.
Knowledge is the new money
“Intellectual capital will always trump financial capital.” — Paul Tudor Jones, self-made billionaire entrepreneur, investor, and philanthropist
We spend our lives collecting, spending, lusting after, and worrying about money — in fact, when we say we “don’t have time” to learn something new, it’s usually because we are feverishly devoting our time to earning money, but something is happening right now that’s changing the relationship between money and knowledge.
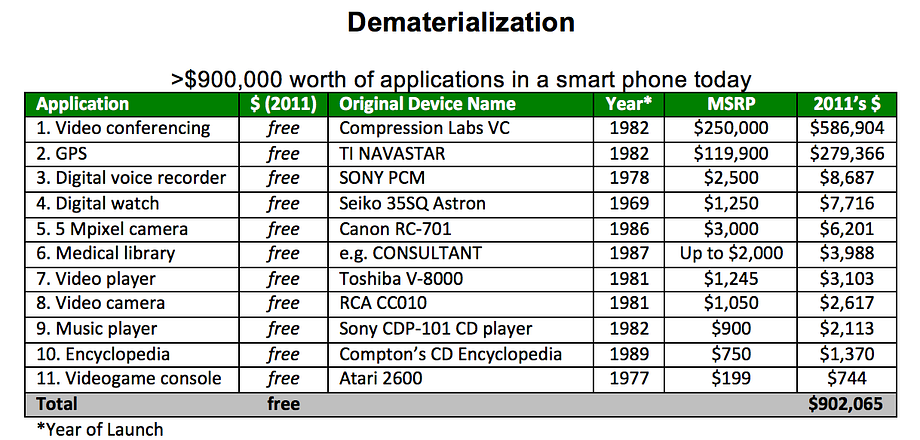
We are at the beginning of a period of what renowned futurist Peter Diamandis calls rapid demonetization, in which technology is rendering previously expensive products or services much cheaper — or even free.
This chart from Diamandis’ book Abundance shows how we’ve demonetized $900,000 worth of products and services you might have purchased between 1969 and 1989.
This demonetization will accelerate in the future. Automated vehicle fleets will eliminate one of our biggest purchases: a car. Virtual reality will make expensive experiences, such as going to a concert or playing golf, instantly available at much lower cost. While the difference between reality and virtual reality is almost incomparable at the moment, the rate of improvement of VR is exponential.
While education and health care costs have risen, innovation in these fields will likely lead to eventual demonetization as well. Many higher educational institutions, for example, have legacy costs to support multiple layers of hierarchy and to upkeep their campuses. Newer institutions are finding ways to dramatically lower costs by offering their services exclusively online, focusing only on training for in-demand, high-paying skills, or having employers who recruit students subsidize the cost of tuition.
Finally, new devices and technologies, such as CRISPR, the XPrize Tricorder, better diagnostics via artificial intelligence, and reduced cost of genomic sequencing will revolutionize the healthcare system. These technologies and other ones like them will dramatically lower the average cost of healthcare by focusing on prevention rather than cure and management.
While goods and services are becoming demonetized, knowledge is becoming increasingly valuable.
“The central event of the twentieth century is the overthrow of matter. In technology, economics, and the politics of nations, wealth in the form of physical resources is steadily declining in value and significance. The powers of mind are everywhere ascendant over the brute force of things.” —George Gilder (technology thinker)
Perhaps the best example of the rising value of certain forms of knowledge is the self-driving car industry. Sebastian Thrun, founder of Google X and Google’s self-driving car team, gives the example of Uber paying $700 million for Otto, a six-month-old company with 70 employees, and of GM spending $1 billion on their acquisition of Cruise. He concludes that in this industry, “The going rate for talent these days is $10 million.”
That’s $10 million per skilled worker, and while that’s the most stunning example, it’s not just true for incredibly rare and lucrative technical skills. People who identify skills needed for future jobs — e.g., data analyst, product designer, physical therapist — and quickly learn them are poised to win.
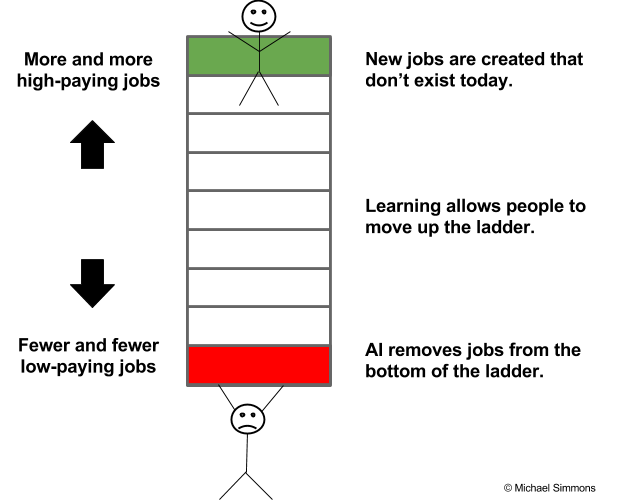
Those who work really hard throughout their career but don’t take time out of their schedule to constantly learn will be the new “at-risk” group. They risk remaining stuck on the bottom rung of global competition, and they risk losing their jobs to automation, just as blue-collar workers did between 2000 and 2010 when robots replaced 85 percent of manufacturing jobs.
Why?
People at the bottom of the economic ladder are being squeezed more and compensated less, while those at the top have more opportunities and are paid more than ever before. The irony is that the problem isn’t a lack of jobs. Rather, it’s a lack of people with the right skills and knowledge to fill the jobs.
An Atlantic article captures the paradox: “Employers across industries and regions have complained for years about a lack of skilled workers, and their complaints are borne out in U.S. employment data. In July [2015], the number of job postings reached its highest level ever, at 5.8 million, and the unemployment rate was comfortably below the post-World War II average. But, at the same time, over 17 million Americans are either unemployed, not working but interested in finding work, or doing part-time work but aspiring to full-time work.”
In short, we can see how at a fundamental level knowledge is gradually becoming its own important and unique form of currency. In other words, knowledge is the new money. Similar to money, knowledge often serves as a medium of exchange and store of value.
But, unlike money, when you use knowledge or give it away, you don’t lose it. In fact, it’s the opposite. The more you give away knowledge, the more you:
Remember it
Understand it
Connect it to other ideas in your head
Build your identity as a role model for that knowledge
Transferring knowledge anywhere in the world is free and instant. Its value compounds over time faster than money. It can be converted into many things, including things that money can’t buy, such as authentic relationships and high levels of subjective well-being. It helps you accomplish your goals faster and better. It’s fun to acquire. It makes your brain work better. It expands your vocabulary, making you a better communicator. It helps you think bigger and beyond your circumstances. It connects you to communities of people you didn’t even know existed. It puts your life in perspective by essentially helping you live many lives in one life through other people’s experiences and wisdom.
Former President Obama perfectly explains why he was so committed to reading during his Presidency in a recent New York Times interview:
“At a time when events move so quickly and so much information is transmitted,” he said, reading gave him the ability to occasionally “slow down and get perspective” and “the ability to get in somebody else’s shoes.” These two things, he added, “have been invaluable to me. Whether they’ve made me a better president I can’t say. But what I can say is that they have allowed me to sort of maintain my balance during the course of eight years, because this is a place that comes at you hard and fast and doesn’t let up.”
6 essentials skills to master the new knowledge economy
“The illiterate of the 21st century will not be those who cannot read and write, but those who cannot learn, unlearn, and relearn.” — Alvin Toffler
So, how do we learn the right knowledge and have it pay off for us? The six points below serve as a framework to help you begin to answer this question. I also created an in-depth webinar on Learning How To Learn that you can watch for free.
Identify valuable knowledge at the right time. The value of knowledge isn’t static. It changes as a function of how valuable other people consider it and how rare it is. As new technologies mature and reshape industries, there is often a deficit of people with the needed skills, which creates the potential for high compensation. Because of the high compensation, more people are quickly trained, and the average compensation decreases.
Learn and master that knowledge quickly. Opportunity windows are temporary in nature. Individuals must take advantage of them when they see them. This means being able to learn new skills quickly. After reading thousands of books, I’ve found that understanding and using mental models is one of the most universal skills that EVERYONE should learn. It provides a strong foundation of knowledge that applies across every field. So when you jump into a new field, you have preexisting knowledge you can use to learn faster.
Communicate the value of your skills to others. People with the same skills can command wildly different salaries and fees based on how well they’re able to communicate and persuade others. This ability convinces others that the skills you have are valuable is a “multiplier skill.” Many people spend years mastering an underlying technical skill and virtually no time mastering this multiplier skill.
Convert knowledge into money and results. There are many ways to transform knowledge into value in your life. A few examples include finding and getting a job that pays well, getting a raise, building a successful business, selling your knowledge as a consultant, and building your reputation by becoming a thought leader.
Learn how to financially invest in learning to get the highest return. Each of us needs to find the right “portfolio” of books, online courses, and certificate/degree programs to help us achieve our goals within our budget. To get the right portfolio, we need to apply financial terms — such as return on investment, risk management, hurdle rate, hedging, and diversification — to our thinking on knowledge investment.
Master the skill of learning how to learn. Doing so exponentially increases the value of every hour we devote to learning (our learning rate). Our learning rate determines how quickly our knowledge compounds over time. Consider someone who reads and retains one book a week versus someone who takes 10 days to read a book. Over the course of a year, a 30% difference compounds to one person reading 85 more books.
To shift our focus from being overly obsessed with money to a more savvy and realistic quest for knowledge, we need to stop thinking that we only acquire knowledge from 5 to 22 years old, and that then we can get a job and mentally coast through the rest of our lives if we work hard. To survive and thrive in this new era, we must constantly learn.
Working hard is the industrial era approach to getting ahead. Learning hard is the knowledge economy equivalent.
Just as we have minimum recommended dosages of vitamins, steps per day, and minutes of aerobic exercise for maintaining physical health, we need to be rigorous about the minimum dose of deliberate learning that will maintain our economic health. The long-term effects of intellectual complacency are just as insidious as the long-term effects of not exercising, eating well, or sleeping enough. Not learning at least 5 hours per week (the 5-hour rule) is the smoking of the 21st century and this article is the warning label.
Don’t be lazy. Don’t make excuses. Just get it done.
“Live as if you were to die tomorrow. Learn as if you were to live forever.” — Mahatma Gandhi
Before his daughter was born, successful entrepreneur Ben Clarke focused on deliberate learning every day from 6:45 a.m. to 8:30 a.m. for five years (2,000+ hours), but when his daughter was born, he decided to replace his learning time with daddy-daughter time. This is the point at which most people would give up on their learning ritual.
Instead of doing that, Ben decided to change his daily work schedule. He shortened the number of hours he worked on his to do list in order to make room for his learning ritual. Keep in mind that Ben oversees 200+ employees at his company, The Shipyard, and is always busy. In his words, “By working less and learning more, I might seem to get less done in a day, but I get dramatically more done in my year and in my career.” This wasn’t an easy decision by any means, but it reflects the type of difficult decisions that we all need to start making. Even if you’re just an entry-level employee, there’s no excuse. You can find mini learning periods during your downtimes (commutes, lunch breaks, slow times). Even 15 minutes per day will add up to nearly 100 hours over a year. Time and energy should not be excuses. Rather, they are difficult, but overcomable challenges. By being one of the few people who rises to this challenge, you reap that much more in reward.
We often believe we can’t afford the time it takes, but the opposite is true: None of us can afford not to learn.
Learning is no longer a luxury; it’s a necessity.
Start your learning ritual today with these three steps
The busiest, most successful people in the world find at least an hour to learn EVERY DAY. So can you!
Just three steps are needed to create your own learning ritual:
Find the time for reading and learning even if you are really busy and overwhelmed.
Stay consistent on using that “found” time without procrastinating or falling prey to distraction.
Increase the results you receive from each hour of learning by using proven hacks that help you remember and apply what you learn.
Over the last three years, I’ve researched how top performers find the time, stay consistent, and get more results. There was too much information for one article, so I spent dozens of hours and created a free masterclass to help you master your learning ritual too!












{kind=link}
{kind=link}