
Cartoon – The short one is the Surgeon
http://www.commonwealthfund.org/publications/blog/2016/jul/value-based-drug-pricing

What would penicillin cost under value-based pricing, a system in which drug makers set prices based on the benefits of their products to consumers and the larger society, rather than drugs’ costs of production? Penicillin has saved millions of lives since its first use in 1942, and it still works for many patients despite growing bacterial resistance to the drug. (Fortunately, many fewer patients get infections with pneumococcus now because we have a good vaccine for it.) Surely, under value-based pricing, penicillin would sell for thousands or tens of thousands of dollars a dose.
Medicine depends on many cheap generic drugs like penicillin to treat conditions as diverse as acne, gout, hypertension, heart disease, and cancer. Pricing these drugs according to their value would make them unaffordable to uninsured and underinsured patients and dramatically increase the aggregate costs of pharmaceuticals.
There is a compelling superficial logic to value-based pricing. Why shouldn’t manufacturers charge the full value of the products they produce? Why shouldn’t consumers have to pay it? That logic begins to fray, however, when you think about how other markets work in our capitalist system.
http://www.commonwealthfund.org/publications/issue-briefs/2016/may/on-medicare-but-at-risk
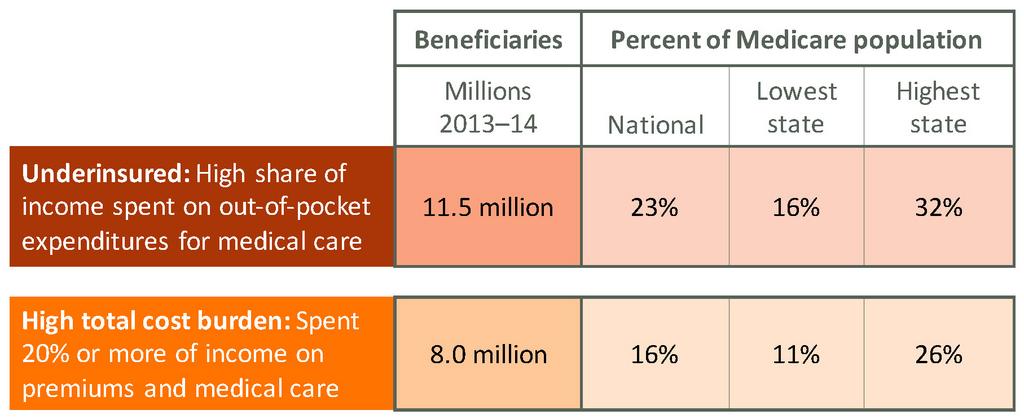
Medicare provides essential health coverage for older and disabled adults, yet it does not limit out-of-pocket costs for covered benefits and excludes dental, hearing, and longer-term care. The resulting out-of-pocket costs can add up to a substantial share of income. Based on U.S. Census surveys, nearly a quarter of Medicare beneficiaries (11.5 million) were underinsured in 2013–14, meaning they spent a high share of their income on health care. Adding premiums to medical care expenses, we find that 16 percent of beneficiaries (8 million) spent 20 percent or more of their income on insurance plus care. At the state level, the proportion of beneficiaries underinsured ranged from 16 percent to 32 percent, while the proportion with a high total cost burden ranged from 11 percent to 26 percent. Low-income beneficiaries were most at risk. The findings underscore the need to assess beneficiary impacts of any proposal to redesign Medicare.
http://www.commonwealthfund.org/publications/fund-reports/2015/dec/aiming-higher-2015

The fourth Commonwealth Fund Scorecard on State Health System Performance tells a story that is both familiar and new. Echoing the past three State Scorecards, the 2015 edition finds extensive variation among states in people’s ability to access care when they need it, the quality of care they receive, and their likelihood of living a long and healthy life. However, this Scorecard—the first to measure the effects of the Affordable Care Act’s 2014 coverage expansions—also finds broad-based improvements. On most of the 42 indicators, more states improved than worsened.
“On most of the 42 indicators, more states improved than worsened.”
By tracking performance measures across states, this Scorecard can help policymakers, health system leaders, and the public identify opportunities and set goals for improvement. The 50 states and the District of Columbia are measured and ranked on 42 indicators grouped into five domains: access and affordability, prevention and treatment, avoidable hospital use and cost, healthy lives, and equity. Individual indicators measure things like rates of children or adults who are uninsured, hospital patients who get information about how to handle their recovery at home, hospital admissions for children with asthma, and breast and colorectal cancer deaths, among many others.

Issue: Finding ways to improve outcomes and reduce spending for patients with complex and costly care needs requires an understanding of their unique needs and characteristics.
Goal: Examine demographics and health care spending and use of services among adults with high needs, defined as people who have three or more chronic diseases and a functional limitation in their ability to care for themselves or perform routine daily tasks.
Methods:Analysis of data from the 2009–2011 Medical Expenditure Panel Survey.
Key findings: High-need adults differed notably from adults with multiple chronic diseases but no functional limitations. They had annual health care expenditures that were nearly three times higher—and which were more likely to remain high over two years of observation—and out-of-pocket expenses that were more than a third higher, despite their lower incomes. On average, rates of hospital use for high-need adults were more than twice those for adults with multiple chronic conditions only; high-need adults also visited the doctor more frequently and used more home health care.
Conclusion: Wide variation in costs and use of services within the high-need group suggests that interventions should be targeted and tailored to those individuals most likely to benefit.

High-need, high-cost (HNHC) patients account for a disproportionate share of health care spending, and the complex care they need can be fraught with quality and safety issues. Any effort to address quality and cost challenges must focus on improving care for this population. The Commonwealth Fund’s David Blumenthal, M.D., and Melinda Abrams highlighted six key opportunities in this JAMA “Viewpoint.”




