https://www.washingtonpost.com/news/powerpost/paloma/the-health-202/2019/05/20/the-health-202-large-employers-don-t-want-medicare-for-all/5ce1aa38a7a0a435cff8c0d4/?utm_term=.47900c042418

Medicare-for-all advocates argue enacting their plan would lift a heavy burden off employers to provide their workers with health-care coverage, which is the way 180 million Americans get their insurance.
But large employers are just fine with being the suppliers of insurance and don’t want to give up that role, according to an association that represents them.
“Overwhelmingly they would like to continue doing it,” Jim Klein, president of the American Benefits Council, told me. “They think they’re doing a good job.”
The American Benefits Council — which represents the country’s largest employers including Walmart, ExxonMobil and Apple — hasn’t joined the large industry coalition of insurers, pharmaceutical makers and hospitals who are vigorously fighting every iteration of Medicare-for-all proposals coming from Capitol Hill (we’ve written about that partnership here).
But its leaders are plenty skeptical of the prospect of a single-payer system, stressing it would upend the way most people in the United States get their coverage and potentially subject employers to big new taxes so the government could pay for the whole thing.
“I think they’re very concerned about sort of a blank check which the government would be filling in the blank, in terms of cost,” Klein said of his members.
The future of employer-sponsored coverage is one of the stickiest questions raised by the Medicare-for-all debate. The shortcomings — and merits — of the system got a lot of airtime during last month’s Medicare-for-all hearing at the House Rules Committee and probably will be part of the debate at a similar hearing House Budget Chairman John Yarmuth (D-Ky.) has scheduled for Wednesday.
Just look at how some of the Democrats running for president have recently danced around the issue.
Sens. Cory Booker (D-N.J.) and Kamala Harris (D-Calif.) are co-sponsors of the latest Medicare-for-all bill from Sen. Bernie Sanders (I-Vt.), which would upend the country’s health insurance system, replacing virtually all private plans with a generous set of benefits provided by the federal government. But both candidates have tried to take a softer stance on what would happen to workplace coverage.
—“I stand by supporting Medicare-for-all, but I’m also that pragmatist that, when I’m chief executive of the country … I’m going to find the immediate things that we can do,” Booker told CNN’s Jake Tapper this month.
“Because I’m telling you right now, we’re not going to pull health insurance from 150 million Americans who have private insurance who like their insurance — my union friends, brothers and sisters, who have negotiated for their health insurance,” Booker added.
—Sen. Kamala Harris (D-Calif.) told Tapper last week “that’s not what I meant” when he asked her to clarify previous comments in which she said she supports eliminating the private insurance industry.
“I support Medicare-for-all but I really do need to clear up what happened on that stage,” Harris said. “It was in the context of saying let’s get rid of all the bureaucracy.”
— Yarmuth poured cold water on the idea of Medicare-for-all being law anytime soon, despite the hearing he’s holding on the issue this week.
“A lot of people, I think, co-sponsored Pramila’s bill for the same reason they co-sponsored H.R. 676; it was the metaphor for Medicare-for-all,” Yarmuth told my colleague Dave Weigel last week. Yarmuth was referring to the House bill proposed by Rep. Pramila Jayapal (D-Wash.).
“Now, people have seen some of the details and said, ‘Okay, we need to look at this.’ There doesn’t seem to be much of a sense of urgency because it’s not going anywhere,” Yarmuth added.
Rep. Donna Shalala (D-Fla.), former Health and Human Services secretary under President Bill Clinton, is also a Medicare-for-all skeptic:
Perhaps these Democrats recall President Barack Obama’s infamous “if you like it, you can keep it,” pledge, where Obama learned the hard way what happens when people lose insurance they wanted to keep. Obama repeatedly promised people they could retain coverage they liked under his 2010 Affordable Care Act. When around 4 million people got notices their plans were being canceled — because they weren’t ACA-compliant — the administration came under heavy fire. The website PolitiFact dubbed Obama’s promise its “Lie of the Year” in 2013.
Yet employer-sponsored plans are still far from perfect. In fact, many health policy wonks have said many of the problems with health insurance in the United States stem from people getting it through the workplace instead of shopping for it on their own.
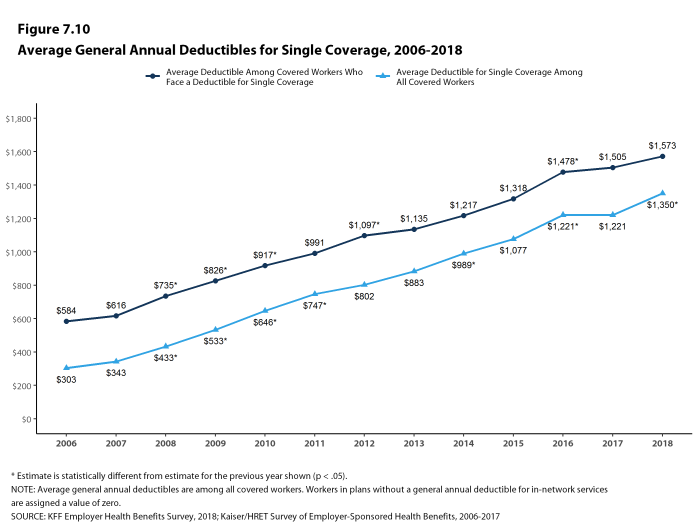
Costs are a big problem for both employers and their workers. For years, employers have grappled with rapid health-care cost inflation, resulting in higher monthly premiums and annual deductibles. Last year, health benefits for the average employee at a large company cost more than $13,000, according to a Mercer survey of employer-sponsored plans.
In response, employers have trended toward high-deductible plans or asked their workers to contribute more to their monthly premiums. Some have also invested in workplace wellness programs, in hopes of creating a healthier, lower-cost workforce.
“It puts a huge burden on employers,” House Rules Committee Chairman James McGovern (D-Mass.) said at his committee’s Medicare-for-all hearing.
Then there’s the issue of portability — the problem created when people change jobs and are forced to also change their health plan. This can be especially costly for those with chronic health conditions, who can’t afford any gaps in coverage and may find themselves having to satisfy an annual deductible for the second time in one year.
Yet to those enmeshed in the system, such as large employers, overhauling the whole thing is a daunting prospect. While health-care costs continue to rise, employers are more fearful of having to help fund the expensive single-payer system proposed in the Sanders and Jayapal bills.
Sanders argues his Medicare-for-all plan would be net cheaper for employers. He has proposed charging them either 75 percent of what they’re paying for each of their employees enrolling in Medicare-for-all or a 7.5 percent payroll tax, whichever is higher.
This would result in a net savings for employers, Sanders argues. Large employers don’t appear convinced.
Klein said the council isn’t necessarily opposed to expanding Medicare to more people — and stresses that its members are deeply interested in reining in cost growth.
But he said employers don’t want a health insurance overhaul, arguing they spend more than $4 on health benefits for every dollar the government loses by exempting the benefits from taxes.
“Our employers are not calling for Uncle Sam,” he said.