Medicaid is critical to our nation’s healthcare system, providing necessary care for more than 72 million Americans – including our neighbors and friends.
Who it Affects
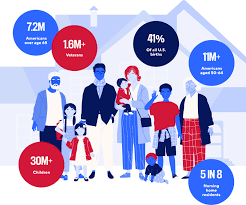
Medicaid covers children, seniors in nursing homes, veterans, people with long-term chronic illnesses, those with mental health issues and working families.
The program helps keep Americans healthy at all stages of life, providing healthcare to families in need — especially as the country continues to recover from record-high inflation.
The Problem
Some policymakers are considering Medicaid cuts that would undermine coverage for countless patients and threaten Americans’ access to comprehensive, 24/7 hospital care.
Medicaid covers health services for patients who otherwise wouldn’t be able to pay for care. Coverage of services is essential for hospitals, and helps ensure all Americans have access to high-quality, 24/7 care, no matter where they live.
Who Medicaid covers
Providing Lifesaving Healthcare Services
Medicaid covers patients with complex and chronic illnesses in need of long-term care, as well as emergency services and prescription coverage.
As the nation faces a growing mental health crisis, Medicaid also ensures millions of Americans — including veterans — have access to mental healthcare and substance abuse services.
Without access to affordable mental healthcare through Medicaid, veterans often lack the long-term support they deserve, and are left to deal with complex health issues years after their service.
In these areas, where primary care providers are few and far between, hospitals become even more vital sites of care — and in some cases, the only sites of care available.
Rural hospitals, already more likely to be at risk of closure, rely on Medicaid funding to stay open and to continue providing lifesaving care to their patients. Nearly 150 rural hospitals have closed or converted since 2010 alone. Further cuts to care would eliminate a lifeline for Americans across the country — with devastating consequences for rural communities.
The Solution
Cuts to Medicaid funding will create irreparable harm for our nation’s most vulnerable communities, including millions of children, veterans, those with chronic illnesses, seniors in nursing homes, and working families. Medicaid helps provide security to these Americans, keeping them healthy at every stage of life.
Congress should vote against efforts to reduce Medicaid funding and instead focus on policies that strengthen access to 24/7 care, rather than take it away.
Understand the health care industry’s most urgent challenges—and greatest opportunities.
The health care industry is facing an increasingly tough business climate dominated by increasing costs and prices, tightening margins and capital, staffing upheaval, and state-level policymaking. These urgent, disruptive market forces mean that leaders must navigate an unusually high number of short-term crises.
But these near-term challenges also offer significant opportunities. The strategic choices health care leaders make now will have an outsized impact—positive or negative—on their organization’s long-term goals, as well as the equitability, sustainability, and affordability of the industry as a whole.
This briefing examines the biggest market forces to watch, the key strategic decisions that health care organizations must make to influence how the industry operates, and the emerging disruptions that will challenge the traditional structures of the entire industry.
Preview the insights below and download the full executive briefing (using the link above) now to learn the top 16 insights about the state of the health care industry today.
Preview the insights
Part 1 | Today’s market environment includes an overwhelming deluge of crises—and they all command strategic attention
Insight #1
The converging financial pressures of elevated input costs, a volatile macroeconomic climate, and the delayed impact of inflation on health care prices are exposing the entire industry to even greater scrutiny over affordability. Keep reading on pg. 6
Insight #2
The clinical workforce shortage is not temporary. It’s been building to a structural breaking point for years. Keep reading on pg. 8
Insight #3
Demand for health care services is growing more varied and complex—and pressuring the limited capacity of the health care industry when its bandwidth is most depleted. Keep reading on pg. 10
Insight #4
Insurance coverage shifted dramatically to publicly funded managed care. But Medicaid enrollment is poised to disperse unevenly after the public health emergency expires, while Medicare Advantage will grow (and consolidate). Keep reading on pg. 12
Part II | Competition for strategic assets continues at a rapid pace—influencing how and where patient care is delivered.
Insight #5
The current crisis conditions of hospital systems mask deeper vulnerabilities: rapidly eroding power to control procedural volumes and uncertainty around strategic acquisition and consolidation. Keep reading on pg. 15
Insight #6
Health care giants—especially national insurers, retailers, and big tech entrants—are building vertical ecosystems (and driving an asset-buying frenzy in the process). Keep reading on pg. 17
Insight #7
As employment options expand, physicians will determine which owners and partners benefit from their talent, clinical influence, and strategic capabilities—but only if these organizations can create an integrated physician enterprise. Keep reading on pg. 19
Insight #8
Broader, sustainable shifts to home-based care will require most care delivery organizations to focus on scaling select services. Keep reading on pg. 21
Insight #9
A flood of investment has expanded telehealth technology and changed what interactions with patients are possible. This has opened up new capabilities for coordinating care management or competing for consumer attention. Keep reading on pg. 23
Insight #10
Health care organizations are harnessing data and incentives to curate consumers choices—at both the service-specific and ecosystem-wide levels. Keep reading on pg. 25
Part III | Emerging structural disruptions require leaders to reckon with impacts to future business sustainability.
Insight #11
For value-based care to succeed outside of public programs, commercial plans and providers must coalesce around a sustainable risk-based payment approach that meets employers’ experience and cost needs. Keep reading on pg. 28
Insight #12
Industry pioneers are taking steps to integrate health equity into quality metrics. This could transform the health care business model, or it could relegate equity initiatives to just another target on a dashboard. Keep reading on pg. 30
Insight #13
Unprecedented behavioral health needs are hitting an already fragmented, marginalized care infrastructure. Leaders across all sectors will need to make difficult compromises to treat and pay for behavioral health like we do other complex, chronic conditions. Keep reading on pg. 32
Insight #14
As the population ages, the fragile patchwork of government payers, unpaid caregivers, and strained nursing homes is ill-equipped to provide sustainable, equitable senior care. This is putting pressure on Medicare Advantage plans to ultimately deliver results. Keep reading on pg. 34
Insight #15
The enormous pipeline of specialized high-cost therapies in development will see limited clinical use unless the entire industry prepares for paradigm shifts in evidence evaluation, utilization management, and financing. Keep reading on pg. 36
Insight #16
Self-funded employers, who are now liable for paying “reasonable” amounts, may contest the standard business practices of brokers and plans to avoid complex legal battles with poor optics. Keep reading on pg. 38
Dr. Philip R. Lee, who as a number one federal well being official and fighter for social justice below President Lyndon B. Johnson wielded authorities Medicare money as a cudgel to desegregate the nation’s hospitals within the Sixties, died on Oct. 27 in a hospital in Manhattan. He was 96.
The trigger was coronary heart arrhythmia, his spouse, Dr. Roz Lasker, mentioned.
From his workplace at the Department of Health, Education and Welfare, because the assistant secretary for well being and scientific affairs from 1965 to 1969, Dr. Lee engineered the introduction of Medicare, which was established for older Americans in 1965, one 12 months after Johnson had bulldozed his landmark civil-rights invoice via Congress.
“To Phil, Medicare wasn’t just a ‘big law’ expanding coverage; it was a vehicle to address racial and economic injustice,” his nephew Peter Lee, the manager director of Covered California, which runs the state’s well being care market below the Affordable Care Act, was quoted as saying in a tribute by the University of California, San Francisco. Dr. Lee was the college’s chancellor from 1969 to 1972, after leaving the Johnson administration.
Dr. Lee’s use of Medicare funding to desegregate hospitals “changed the economic lives of millions of seniors,” Mr. Lee added.
Provisions within the Medicare laws subjected 7,000 hospitals nationwide to guidelines barring discrimination towards sufferers on the premise of race, creed or nationwide origin. The regulation required equal remedy throughout the board — from medical and nursing care to mattress assignments and cafeteria and restroom privileges — and barred discrimination in hiring, coaching or promotion.
Before the regulation took impact in 1966, fewer than half the hospitals within the nation met the desegregation commonplace and fewer than 25 p.c did within the South.
“I remember during one of my visits,” Dr. Lee instructed the journal of the American Society on Aging in 2015, “a cardiologist at Georgia Baptist Hospital told me, ‘Well, you know, Dr. Lee, if I put a nigger in with one of my white patients, it would kill the patient. My patient would die of a heart attack.’”
By February 1967, a 12 months or much less after many of the regulation’s provisions had taken impact, 95 p.c of hospitals have been compliant, Dr. Lee mentioned.
“He was largely responsible for that effort,” mentioned Professor David Barton Smith of Drexel University and writer of “The Power to Heal: Civil Rights, Medicare and the Struggle to Transform America’s Health System” (2016).
Dr. Lee hailed from a household of physicians — his father and 4 siblings have been medical doctors — and whereas working within the Palo Alto Medical Clinic (now the Palo Alto Medical Foundation), which his father based, he noticed firsthand the consequences on the poor and the aged of insufficient well being care and the shortage of insurance coverage protection.
As early as 1961, he was a guide on growing older to the Santa Clara Department of Welfare in California, and as a member of the American Medical Association and a Republican at the time, he defied each the A.M.A. and his celebration in testifying earlier than Congress on behalf of a precursor to Medicare that might have helped pay for hospital and nursing dwelling care via Social Security for sufferers over 65.
Dr. Lee was branded a socialist and a Communist (irrespective of that he had served as a physician within the Korean War).
In 1987, after main the University of California, San Francisco, and heading well being coverage and analysis packages there as a professor of social drugs, he additional riled fellow physicians when, as chairman of Congressional fee, he really helpful a standardized nationwide restrict on how a lot medical doctors enrolled within the Medicare program, with an enormous pool of sufferers obtainable to them, might cost above a set schedule.
He was referred to as again to Washington in 1993, once more to be an assistant secretary, this time of the renamed Department of Health and Human Services below the Clinton administration. Serving till 1997, he suggested the White House on its in the end failed effort on well being care reform.
In 2015 he endorsed the Obama administration’s Affordable Care Act and steered that the nation might go even additional in guaranteeing common well being care.
“In 1967, President Johnson said we would continue to work until equality of treatment is the rule,” Dr. Lee wrote in Generations: Journal of the American Society on Aging. “By making Medicare an option for all Americans, the kind of care I receive could be available to everyone.”
Philip Randolph Lee was born in San Francisco on April 17, 1924, to Dr. Russell Van Arsdale Lee, who had lobbied for nationwide medical insurance as a member of a fee appointed by President Harry S. Truman, and Dorothy (Womack) Lee, an newbie musician.
His curiosity in drugs, he instructed Stanford Medicine Magazine in 2004, “began with house calls with my dad from the age of 6 or 7.”
He earned his bachelor’s and medical levels at Stanford University in 1945 and 1948. As a member of the Naval Reserve, he was on lively responsibility as a physician at the top of World War II and once more from 1949 to 1951, through the Inchon invasion in Korea. He obtained a grasp of science diploma from the University of Minnesota in 1955 and had fellowships at the Rusk Institute of Rehabilitation Medicine in New York and the Mayo Clinic.
“Phil moved from clinical medicine to health policy and then devoted his life to addressing issues at the nexus of civil rights, social justice and health,” Dr. Lasker, his spouse, mentioned in an e-mail.
His distinguished function in shaping Medicare and different federal well being insurance policies was preceded by a stint, 1963-65, as director of well being for the Agency for International Development. As chancellor of the University of California, San Francisco, he was credited with rising racial variety amongst its workers, college and pupil physique.
He was additionally lauded for his aggressive function in confronting the AIDS epidemic because the president of the newly-formed Health Commission of the City and County of San Francisco from 1985 to 1989.
The writer of a half-dozen books, Dr. Lee was an early critic of the pharmaceutical trade in “Pills, Profits and Politics” (1974, with Milton Silverman).