Earlier this week, the Centers for Medicare and Medicaid Services (CMS) issued a proposal to remedy its four years of payment cuts to the more than 1,600 hospitals participating in the 340B Drug Pricing Program through one-time, lump-sum payments that will total roughly $9B.
In 2018, CMS reduced drug reimbursement to 340B covered-entity hospitals by nearly 30 percent, in an attempt to align reimbursement with hospitals’ actual drug acquisition costs. The Supreme Court overturned those cuts in 2022, ruling that the Department of Health and Human Services (HHS) had violated rulemaking procedure. As CMS rulemaking on Medicare payment must be budget-neutral, the agency will offset the remedy payments with a 0.5 percent cut to all hospitals for non-drug items and services covered under the Hospital Outpatient Prospective Payment System (OPPS) over the next 16 years. Stakeholders have until September 5th to comment on the proposed rule. Once the final rule is published later this year, CMS plans to repay 340B participant hospitals within 60 days of their application for remedy.
The Gist: After worries about how last year’s Supreme Court ruling would be implemented, 340B participant hospitals will be relieved to receive their payment corrections up front instead of over time, especially given current margin challenges.
But while this issue is now set to be resolved, other critical decisions about the 340B program’s fate are pending before courts. Earlier this year, Bayer and EMD Serono became the 20th and 21st drugmakers to restrict discounts to contract pharmacies, following an appellate court decision in January that sided with the pharmaceutical manufacturers.
Meanwhile, appellate courts in other jurisdictions are set to hear at least two more cases on the issue, amid conflicting rulings about whether HHS can enforce contract pharmacy discounts.
Five recent Supreme Court rulings have reset the context for U.S. jurisprudence for years to come and open a can of worms for healthcare operators.
Last year’s SCOTUS decision ruling in Dobbs v. Jackson Women’s Health (June 24, 2022) set the tone: in its 6-3 decision, the high court determined that that access to abortion is a state issue, not federal thus nullifying the 50-year-old legal precedent in Roe v. Wade and reversing 2 lower court rulings.
On June 1, 2023, in the United States v. Supervalu, petitioners sued SuperValu and Safeway under the False Claims Act (FCA) alleging they defrauded the Medicare and Medicaid by knowingly filing false claims. Essentially, the plaintiffs sought financial remedy because the retailers’ prices were not explicitly and specifically “usual and customary” prices. In its unanimous ruling, SCOTUS agreed that “the phrase ‘usual and customary’ is open to interpretation, but reasoned that “such facial ambiguity alone is not sufficient to preclude a finding that respondents knew their claims were false.”
On June 29, 2023, in Students for Fair Admissions, Inc. v. President and Fellows of Harvard College, the court ruled 6-3 that affirmative action policies at Harvard and the University of NC that consider an applicant’s race in college admissions are unconstitutional.
On June 30, 2023, in 303 Creative LLC v. Elenis (June 30, 2023) By a vote of 6-3, SCOTUS ruled that the First Amendment right of free speech prohibits Colorado from forcing a website designer to create expressive designs speaking messages with which the designer disagrees.
On June 30, 2023, in Department of Education v. Brown: By a unanimous vote, SCOTUS ruled that the 2 plaintiffs lacked standing to “Article III standing to assert a procedural challenge to the student-loan debt-forgiveness plan adopted by the Secretary of Education pursuant to Higher Education Relief Opportunities for Students Act of 2003 (HEROES Act).” In effect, the court vacated and remanded the judgment of the United States Court of Appeals for the 5th Circuit because it felt Myra Brown and Alexander Taylor (plaintiffs) did not prove that any injury suffered from not having their loans forgiven. Therefore, the court had no jurisdiction to address their procedural claim.
Each of these is specific to a circumstance but collectively they expose industries like healthcare to greater compliance risk, potential court challenges and operational complexity. Here’s an example:
The 58-year-old Kennedy-era legal precedent of affirmative action to redress racial inequity was the focus in Students for Fair Admissions, Inc. v. President and Fellows of Harvard College. SCOTUS essentially sided with plaintiffs who argued affirmative action violates the 14th Amendment’s Equal Protection guarantee. In healthcare, research shows access to the healthcare system is disproportionately inaccessible to persons of color, especially if they’re poor. They improve when individuals are treated by clinicians of the same race but only about 5% of doctors in America are Black, compared to 12% of the general population and only 6% of doctors in the U.S. are Hispanic while the group accounts for nearly almost 20% of the general population.
Notwithstanding the uncanny similarities between higher education and healthcare (both have raised prices above GDP and overall inflation rates for 2 decades, both jealously protect their reputations against outside transparency and unflattering report cards, both feature competition between public and private institutions and both face questions about the value of their efforts), the issue of diversity is central in both. Affirmative action is a means to that end, but at least for now and in higher education, it’s not constitutional.
Might workforce diversity and clinician training efforts be stymied by the prospect of court challenges? Might “affirmative action” in healthcare be replaced by “holistic review” to enable consideration of an applicant’s life or quality of character as some conservative jurists have suggested?
My take:
Affirmative action per the example above is only one of many constructs widely accepted in healthcare today where court challenges may alter the future. Individual rights and free speech including online medical advice, the role of state governments, fraud and abuse and other domains are equally exposed.
It’s clear this court is not threatened by legal precedent nor cautious about public opinion on touchy issues. Thus, immediate imperatives for healthcare organizations are these:
Revisit legal precedents on which the ways we operate are based: Roles and responsibilities in US healthcare are sacrosanct and protected by legal precedent: Physicians diagnose and treat; others don’t. Insurers pay claims but don’t practice medicine. Not for profit hospitals serve community needs in exchange for tax-exemption. Public health programs that serve the poor are funded by local and state governments. Employer sponsored benefits underwrite the system’s profitability and fund its hospital Part A obligations and so on. Might a conservative court revisit these in the context of the constitution’s “general welfare” purpose and redirect its focus, roles and structure?
Revisit terms and phrases where consensus is presumed but specific definition is lacking: Just as SCOTUS recognized ambiguity in applying terms like “usual and customary” in its Supervalu-Safeway ruling, it is likely to challenge other widely used phrases used in healthcare that often lack specific referents i.e., quality, safety, efficacy, effectiveness, community benefit, charity care, evidence-based care, cost-effectiveness, not-for-profit, competition, value” and many others. Might SCOTUS force the industry to more specifically define its most widely used phrases in order to justify its claims?
For everyone in healthcare, these rulings open a can of worms. Compliance risk assessments, scenario plan updates required!
Thursday marks the 13th anniversary of the signing of the Affordable Care Act– perhaps the most consequential healthcare legislation since LBJ’s passage of the Medicare Act in 1965. Except in healthcare circles, it will probably go unnoticed.
World events in the Ukraine and China President Xi Jinping’s visit to Russia will grab more media attention. At home, the ripple effects of Silicon Valley Bank’s bankruptcy and the stability of the banking system will get coverage and former President Trump’s arrest tomorrow will produce juicy soundbites from partisans and commentators. Thus, the birthday of Affordable Care Act, will get scant attention.
That’s regrettable: it offers an important context for navigating the future of the U.S. health system. Having served as an independent facilitator between the White House and private sector interests in 2009-2010, I recall vividly the events leading to its passage and the Supreme Court challenge that affirmed it:
The costs and affordability of healthcare and growing concern about the swelling ranks of uninsured were the issues driving its origin. Both political parties and every major trade group agreed on the issues; solving them not so easy.
Effective messaging from special interests about the ACA increased awareness of the law and calcified attitudes for or against. Misinformation/disinformation about the “Patient Protection and Affordable Care Act” morphed to a national referendum on insurance coverage and the cost-effectiveness of the ACA’s solution (Medicaid expansion, subsidies and insurance marketplaces). ‘Death panels. government run healthcare and Obamacare’ labels became targets for critics: spending by special interests opposed to the law dwarfed support by 7 to 1. Differences intensified: Emotions ran high. I experienced it firsthand. While maintaining independence and concerns about the law, I received death threats nonetheless. Like religion, the ACA was off-limits to meaningful discussion (especially among the majority who hadn’t read it).
And after Scott Brown’s election to the vacant Massachusetts seat held by Ted Kennedy in January, 2010, the administration shifted its support to a more-moderate Senate Finance Committee version of the law that did not include a public option or malpractice reforms in the House version. Late-night lobbying by White House operatives resulted in a House vote in favor of the Senate version with promises ‘it’s only the start’. Through amendments, executive orders, administrative actions and appropriations, it would evolve with the support of the Obama team. It passed along party lines with the CBO offering an optimistic view it would slow health cost escalation by reducing administrative waste, implementation of comparative effectiveness research to align evidence with care, increased insurance coverage, changing incentives for hospitals and physicians and more.
The Affordable Care Act dominated media coverage from August 2009 to March 2010. In the 2010 mid-term election, it was the issue that catapulted Republicans to net gains of 7 in the Senate, 63 in the House and 6 in Governor’s offices. And since, Republicans in Congress have introduced “Repeal and Replace” legislation more than 60 times, failing each time.
Today, public opinion about the ACA has shifted modestly: from 46% FOR and 40% against in 2010 to 55% FOR and 42% against now (KFF). The national uninsured rate has dropped from 15.5% to 8.6% and Medicaid has been expanded in 39 states and DC. Lower costs, increased affordability and quality improvements owing to the ACA have had limited success.
Key elements of the ACA have not lived up to expectations i.e. the Patient Centered Outcome Research Institute, the National Quality Strategy, Title V National Healthcare Workforce Task Force, CMMI’s alternative payment models and achievement of Level 3 interoperability goals vis a vis ONCHIT, CHIME et al. So, as the 2024 political season starts, the ACA will get modest attention by aspirants for federal office because it addressed big problems with blunt instruments. Most recognize it needs to be modernized based on trends and issues relevant to healthcare in 2030 and beyond.
Trends like…
Self-diagnostics and treatment by consumers (enabled by ChatGPT et al).
Data-driven clinical decision-making.
Integration of non-allopathic methodologies.
The science of wellbeing.
Complete price, cost and error transparency.
Employer and individual insurance coverage optimization.
And others.
Issues like….
The role and social responsibility of private equity in ownership and operation of services in healthcare delivery and financing.
The regulatory framework for local hospitals vs. Regional/nation health systems, and between investor-owned and not-for-profit sponsorship.
The role and resources for guided self-care management and virtual-care.
Innovations in care delivery services to vulnerable populations using technologies and enhanced workforce models.
Modernization of regulatory environments and rules of competition for fully integrated health systems, prescription drug manufacturers, health insurers, over-the counter therapies, food as medicine, physician ownership of hospitals, data ownership, tech infomediaries that facilitate clinical decision-making, self-care, professional liability and licensing and many others.
Integration of public health and local health systems.
The allocation of capital to the highest and best uses in the health system.
The sustainability of Medicare and role of Medicare Advantage.
The regulatory framework for disruptors”.
And many others.
These trends are not-easily monitored nor are the issues clear and actionable. Most are inadequately addressed or completely missed in the ACA.
Complicating matters, the political environment today is more complicated than in 2010 when the ACA became law. The economic environment is more challenging: the pandemic, inflation and economic downturn have taken their toll. Intramural tensions in key sectors have spiked as each fights for control and autonomy i.e. primary care vs. specialty medicine, investor-owned vs. not-for-profit hospitals, retail medicine & virtual vs. office-based services, carve-outs, direct contracting et al . Consolidation has widened capabilities and resources distancing big organizations from others. Today’s media attention to healthcare is more sophisticated. Employers are more frustrated. And the public’s confidence in the health system is at an all-time low.
“ACA 2.0” is necessary to the system’s future but unlikely unless spearheaded by community and business leaders left out of the 1.0 design process. The trends and issues are new and complicated, requiring urgent forward thinking.
US District Judge Reed O’Connor ruled on Thursday that the Affordable Care Act’s (ACA’s) requirement for most insurers to cover certain preventative care services without cost-sharing is unlawful. Judge O’Connor—who invalidated the entire ACA in 2018, before the Supreme Court reversed that ruling—had already sided with the plaintiffs in Braidwood vs. Becerra last September, on the grounds that mandatory coverage of HIV prevention treatment, also known as PrEP therapy, violated their religious beliefs. His latest ruling applies to the ACA-mandated preventive services that are compelled by the US Preventative Services Task Force (USPSTF), on the grounds of the task force’s makeup and the fact that some of its recommendations predate the ACA. Services covered for no cost today include screening tests for a variety of cancers, sexually transmitted infections, and diabetes. The ruling does not impact other ACA preventative care services, like contraceptive services and children’s immunizations, as they are based on the recommendations of other government advisory groups. The immediate impact of this week’s ruling is unclear, as the Biden administration has already filed an appeal and may seek to stay the ruling, while most insurance contracts are set on an annual basis.
The Gist: Given the reasoning laid out in Judge O’Connor’s Braidwood v. Becerra ruling last fall, this decision was expected. As with previous attempts to repeal the ACA that have come through his district, the ultimate fate of the ACA’s cost-free preventative care services will likely be decided by the US Supreme Court. It’s possible that the Court may find the narrow targeting of this case more reasonable, making no-cost preventive care coverage optional for employers.
If that happens, millions of Americans could again have to pay for some of the most common and highest-value healthcare services. That additional financial burden, along with tightening of health plan benefit designs, could create barriers to access and exacerbate health disparities.
The sports betting market has multiplied tenfold in three years and may have reached $7 billion in 2022. More than half of the nation can now legally gamble on sports. Fifty million Americans are expected to bet on the upcoming Super Bowl.
Five years ago, betting on live games was illegal in most of the United States. A Supreme Court ruling in 2018 removed the ban and transformed the industry. Now, 33 states and the District of Columbia allow wagers on games.
Addiction experts fear a coming national epidemic to rival the opioid crisis.
“Gambling is a very different addiction from drugs or alcohol,” said Lia Nower, a professor and director of the Center for Gambling Studies at Rutgers University. “If I’m drunk or high, at some point my family is going to figure it out. With gambling, I can be sitting with my kids, watching cartoons, and gambling away my house, my car, everything I own, on my mobile phone. How would you know?”
The Supreme Court ruling struck down a federal law that had banned most commercial sport wagering outside Las Vegas. The subsequent spread of legal gambling was stunningly swift.
Lobbyists pampered state lawmakers with parties and promises, predicting millions in new tax dollars. Much of the promised revenue hasn’t reached the states, according to a New York Times investigation.
But gambling dollars have reached the betting operators. The industry reaped $4.3 billion in revenue on $57 billion in wagers in 2021. In the first 11 months of 2022, Americans bet $83 billion on sports and delivered $6.6 billion to betting firms. That figure is 15 times what the sports gambling industry reaped in 2018.
“We have a movement toward expanding what was once considered a sin, what was once considered a vice, and embedding it at every level of American culture, down to kindergarten,” said Timothy Fong, a clinical professor of psychiatry at the Jane and Terry Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles.
“Sports gambling market. Ten years ago, those words didn’t exist,” Fong said. “What you have is this massive, exponential expansion of gambling into homes, faster than we can study or monitor it.”
A record 50 million Americans, one adult in five, will bet on Super Bowl LVII, according to an American Gaming Association survey. They will wager $16 billion, twice as much as last year.
Celebrity athletes shill for betting firms on television. Betting firms promote gambling on college campuses. Professional teams court “official mobile sports betting partners.”
“Pete Rose was banned from baseball and blocked from the Hall of Fame because he gambled,” said Nower, of Rutgers. “Now, we’ve got professional ballplayers who are partnering with gambling companies. Now, kids are seeing these things inextricably linked.”
Teams and league owners love sports betting because they “have found that engagement is off the charts among people who are placing bets on games,” said Daniel Barbarisi, author of “Dueling with Kings: High Stakes, Killer Sharks, and the Get-Rich Promise of Daily Fantasy Sports.”
People who bet on games “are not just tuning out if it’s a blowout,” Barbarisi said, because they bet on more than the final score. Fans can place wagers on the margin of victory, the combined point total from both teams and other metrics — such as whether Aaron Judge will hit a home run or Max Scherzer will ring up double-digit strikeouts.
Sports bettors are predominantly male, surveys show. They are mostly under 45. Some are wealthy, but a Rutgers study found that half of sports gamblers earn less than $50,000 a year. Some hail from a distinct subpopulation of Americans who get a thrill from risking money on the Next Big Thing.
“You can kind of draw a through line from the people who were involved in the poker boom in the early 2000s to the daily fantasy thing in the 2010s and then to the crypto thing,” Barbarisi said.
“I don’t know if you can say it’s a small group of guys anymore. It’s a big group of guys.”
Gambling is unquestionably addictive, and arguably immoral: Not for nothing did Las Vegas earn the Sin City sobriquet. Now that betting on sports is broadly legal, however, Americans are warming to the idea.
A poll by The Washington Post and University of Maryland found that 66 percent of Americans approved of legal sports betting in 2022, up from 55 percent in 2017, a year before the Supreme Court decision.
Nower suspects most Americans remain naive about gambling’s ills, much as society once cheerily embraced smoking and drinking. “We are where cigarettes were in the 1940s and alcohol was in the 1950s,” she said.
Most Americans ignored the opioid crisis, a staggering increase in overdose deaths in the 1990s and 2000s, until the government and news media processed the data and tendered a response.
With sports betting, “you have the exact same players you had with opioids,” Fong said. “You have government. You have industry. You have civilians, a lot of whom will benefit from this. And then you have a population who will develop an addiction, let’s say 1, 1.5 percent of the population.”
With legal sports gambling, “It’s a hidden addiction,” Fong said. “You can’t see it, you can’t smell it, you can’t taste it.”
Fong points to one of his patients, a man in his 20s who earns $160,000 a year and owes $40,000 in gambling debts.
“On face value, he can pay his rent, he’s not gonna die,” Fong said. “But he’s miserable. He’s just not happy.”
Over time, researchers say, sports-betting addiction will take a toll in rising rates of bankruptcy, domestic violence, depression, anxiety and suicide.
The federal government takes a keen interest in regulating alcohol, tobacco and drugs. In sports gambling, by contrast, “there is no federal presence at all,” Nower said. “And that is the biggest problem.”
Oversight of the booming sports-betting industry has been mostly left to states.
States that allow legal sports gambling “are not disinterested parties,” the Times wrote in its 2022 investigation. “They collect taxes on gambling, and the more people bet, the more governments get. One result is that states have, in many ways, given gambling companies free rein.”
New Jersey, the state at the heart of the 2018 Supreme Court ruling, offers a rare exception, Nower said.
Gambling regulators in New Jersey studied “the relationship between gambling and problem gambling” before they allowed legal gambling on sports, Nower said. She knows of no other state that took that step.
New Jersey uses gambling data to identify “people who may be exhibiting problem symptoms,” Nower said: Shuffling several payment methods, overdrawing their cards, doubling down on bets, gambling more frequently.
Most other states “are just legalizing this stuff without any idea of the effects,” she said.
The sports betting landscape will remain untamed, researchers say, until governments recognize gambling as a matter of public health.
“I do think there are watershed moments in all public health crises,” Nower said. “Unfortunately, it usually takes some kind of crisis or tragedy to turn the tide.”
The plaintiffs in Braidwood v. Becerra filed a motion on Monday asking a US District Court judge in Texas—the same judge who ruled the entire ACA unconstitutional in 2018—to block enforcement of the ACA’s no-cost requirement for preventive care services. This judge already sided with the plaintiffs in September, ruling the government cannot require a company to fully cover preventive HIV drugs, also known as PrEP therapy, for its employees, on the grounds that doing so violates owners’ religious freedom.
In that ruling, the judge also asserted that the government’s system for deciding what preventive care services should be covered under the ACA is unconstitutional. This latest motion now asks him to invalidate all parts of the ACA requiring preventive health services on the grounds that the Preventive Services Task Force was never appointed by Congress, and thus lacks the authority to say which services insurers must cover. The final ruling is expected early next year, after which the case will certainly be appealed, regardless of outcome.
The Gist: Given the judge’s initial ruling in Braidwood last month, this motion from the plaintiffs was expected. While the US Supreme Court reversed a 2018 ruling by this judge that struck down the entire ACA, it could potentially find the narrow targeting of this case more reasonable, making preventive care coverage optional for employers.
If that happens, millions of Americans would once again have to pay for some of the most common and highest-value healthcare services, including screening tests for a variety of cancers, sexually transmitted infections, and diabetes. That additional financial burden, along with likely tightening of health plan benefit designs, would create barriers to access and exacerbate health disparities.
The court ruling comes after the Supreme Court struck down a nearly 30 percent cut to 340B hospital payments from 2018.
October 04, 2022 – A federal judge has ordered HHS to immediately end the almost 30 percent cut in Medicare drug reimbursement to 340B hospitals.
The decision published last week by judge Rudolph Contreras with the US District Court for the District of Columbia rejected HHS’ plan to restore full payment to hospitals participating in the 340B Drug Pricing Program in 2023.
“HHS should not be allowed to continue its unlawful 340B reimbursements for the remainder of the year just because it promises to fix the problem later,” wrote Contreras.
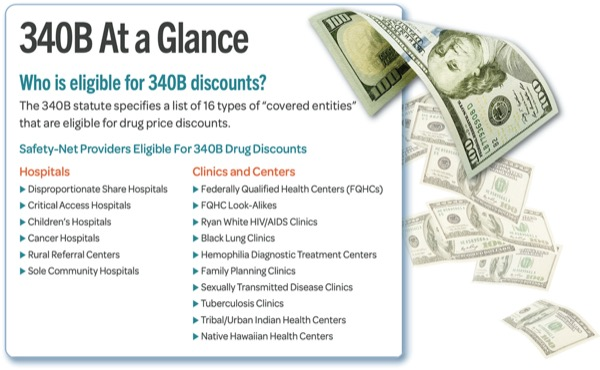
Hospitals participating in the 340B Drug Pricing Program receive outpatient prescription drugs at a discounted price of up to 50 percent since they treat a disproportionate amount of low-income and vulnerable patients. The 340B Program is designed to enable the safety-net providers to stretch their financial resources. Medicare must also reimburse hospitals for administering covered outpatient drugs.
HHS reduced the Medicare drug reimbursement rates for 340B hospitals though in 2018, cutting payments by 28.5 percent in an effort to generate about $1.6 billion in savings. Federal officials reasoned that reimbursing 340B hospitals at the same rate as other hospitals creates an incentive for the hospitals to overprescribe the drugs or prescribe more expensive drugs since they receive covered outpatient drugs at a discounted price.
HHS also argued that 340B hospital reimbursement cuts would lower co-payments for Medicare beneficiaries since the amounts are tied to hospital reimbursement rates.
Hospitals and hospital groups, including the American Hospital Association (AHA) Association of American Medical Colleges (AAMC), and American’s Essential Hospitals, sued the federal government over the reduced reimbursement rates.
The case made it all the way to the Supreme Court where, in a major win for hospitals, judges unanimously ruled that HHS should not have reduced payments to certain hospitals in 2018 and 2019 without surveying hospitals to determine average acquisition costs for drugs. HHS had relied on the average price of the drugs to set lower rates.
However, the Supreme Court did not make judgments on 340B hospital reimbursement cuts for 2020 and later years. Following the Supreme Court’s ruling, HHS announced it would reimburse hospitals for administering 340B-covered drugs the same as non-340B drugs starting Jan. 1, 2023.
Hospital groups again challenged HHS policy, asking the courts to immediately halt the unlawful cuts in 2022.
“The AHA appreciates Judge Contreras’ ruling that the Department of Health and Human Services must immediately stop unlawful reimbursement cuts for 2022 for hospitals participating in the 340B drug pricing program. Halting these cuts will help 340B hospitals provide comprehensive health services to their patients and communities,” said Melinda Hatton, AHA’s general counsel and secretary, regarding the most recent court ruling.
“We continue to urge the Administration to promptly reimburse all the hospitals that were affected by these unlawful cuts in previous years and to ensure the remainder of the hospital field is not penalized for their prior unlawful policy, especially as hospitals and health systems continue to deal with rising costs for supplies, equipment, drugs and labor,” Hatton continued in the public statement.
340B Health’s president and CEO Maureen Testoni also called the court ruling “an important victory for 340B hospitals that have been fighting these unlawful cuts for nearly six years.” 340B health advocates safety-net hospitals participating in the drug pricing program.
“The Centers for Medicare & Medicaid Services (CMS) has the clear responsibility to restore the appropriate payments for 340B drugs immediately, and now a federal court has ordered it to do so without delay,” Testoni said.
HHS has not announced a repayment plan for 340B hospitals. Notably, the court ruling also did not cover the AHA’s motion to include reimbursement cuts from 2020 through 2022 in the case, nor AHA’s motion to repay hospitals for the cuts since 2018 without penalizing other hospitals.
The same Texas federal judge who ruled the entire ACA unconstitutional in 2018—a decision overturned by the Supreme Court last year—ruled this week that the ACA cannot require a company to fully cover preventive HIV drugs for its employees, on the grounds that doing so violates owners’ religious freedom. He also asserted that the government’s system for deciding what preventive care services should be covered under the ACA is unconstitutional, a broader declaration that potentially jeopardizes a wide swath of no-cost preventive services enshrined in the ACA for millions of Americans, including screening tests for a variety of cancers, sexually transmitted infections, and diabetes. The ruling did not include an injunction and is likely to be appealed.
The Gist: Fully-covered preventive care services are a cornerstone of the ACA, and have increased access to basic healthcare services for many Americans. While there is still some uncertainty about the scope of this ruling, if it were to stand, millions of Americans would once again have to pay for some of the most common and highest-value healthcare services. That additional financial barrier, along with potential tightening of health plan benefit designs, would create barriers to access that only exacerbate our nation’s already stark healthcare disparities.
The American Hospital Association wants HHS to act quickly to ensure that affected hospitals receive withheld 340B program funds.
The organization’s June 28 letter to HHS comes after the Supreme Court recently overturned a $1.6 billion 340B payment cut.
The case centered around whether CMS has the authority to make cuts to the program under its Medicare Outpatient Prospective Payment System. Under the payment rule, HHS cut the reimbursement rate for covered drugs by 28.5 percent in 2018, but it later lowered the cut to 22.5 percent. The Supreme Court reversed a federal appeals court’s 2020 ruling that HHS had the authority to make the $1.6 billion annual reimbursement cut.
“Given the vital role that 340B hospitals play in serving vulnerable communities, they should be repaid the funds that have been withheld from them without delay,” the American Hospital Association said in the letter. “They also should be paid for all of the years (2018-2022) in which the Centers for Medicare & Medicaid Services (CMS) illegally cut reimbursement rates.”
The hospital group said it is concerned that despite the Supreme Court’s decision, the resolution of these issues “could be bogged down in needless litigation, and that hospitals will not be appropriately compensated at a time when they are weathering significant financial challenges on many fronts.”
The 6-3 decision in Dobbs v. Jackson Women’s Health Organization, challenging a Mississippi law banning most abortions after 15 weeks, overturns the nearly 50-year precedent providing a constitutional right to abortion. The opinion was little changed from a draft that was leaked last month, returning most decision making on abortion to states. At least 13 states have so called ‘trigger laws’ in place that will almost immediately make abortion illegal, and another 13 states are likely to pass similar laws.
The Gist: In over half of states, existing or new laws will likely prevent pregnant people from accessing critical and evidence-based reproductive healthcare services, including medically safe abortion, miscarriage care, pregnancy termination for severe fetal anomalies, and endangerment of the childbearing parent’s life.
Patients in Texas, which passed one of the strictest abortion laws last year, have already been facing challenges obtaining prescriptions for medications for miscarriage and abortion care. Many state laws which criminalize providing the procedure put physicians and other medical providers in legal jeopardy.
And as legal experts point out, most malpractice insurance doesn’t protect physicians from damages incurred from criminal charges.
Moreover, most laws have been written by legislators with little or no medical expertise, leading to lack of clarity about which potentially life-threatening situations, in what circumstances, merit pregnancy termination—forcing physicians to delay lifesaving obstetric care. (Read this NEJM piece to understand what this looks like for doctors and patients in Texas today.) Regardless, today’s decision will lead to increased mortality for pregnant people and those unable to seek safe abortion care.