Cartoon – Modern Leadership Survival


https://www.beckershospitalreview.com/finance/hospitals-are-investing-in-housing-here-s-why.html

Several factors, including changes in reimbursement, have motivated some hospitals to invest in community housing projects, according to NPR.
In the 1990s, 50 percent of the children in Southern Orchards — near Columbus, Ohio-based Nationwide Children’s Hospital — lived in poverty. Through a partnership called the Healthy Neighborhoods Healthy Families initiative, Columbus, community groups like United Way, and Nationwide Children’s began to invest in the neighborhood’s homes. In 2008, the organizations started renovating vacant homes for resale, building affordable housing and funding renovations for homeowners.
With a $6.6 million infusion from Nationwide Children’s, the $22 million project led to the construction of 58 affordable housing units, 71 renovated homes and 15 new homes. The organizations also gave out 149 home improvement grants from 2008 to 2018, according to the report, which cites Pediatrics.
Kelly Kelleher, MD, director of the Center for Innovation in Pediatric Practice at Nationwide Children’s, writes in Pediatrics that Nationwide Children’s is treating “the neighborhood as a patient.” The hospital is attempting to mend harmful socio-economic and physical environments in the hope it will lower the prevalence of health issues caused by those conditions. The investment could pay for itself if the number of hospital visits from Southern Orchards neighborhood falls, said Dr. Kelleher.
Hospitals across the country are taking similar approaches, though not as direct as owning and operating housing in a certain neighborhood, according to Megan Sandel, MD, who helps direct Boston Medical Center’s housing initiative. Dr. Sandel said Boston Medical Center’s projects are owned and operated by other community organizations. Similar projects are off the ground in Seattle, Boston, Atlanta and New York, among other places.
A potential motivator for these projects is a shift from fee-for-service medicine to reimbursement based on improving quality of care, according to the report. Some states are even starting to give healthcare organizations funding to manage populations.
https://www.beckershospitalreview.com/finance/6-latest-hospital-bankruptcies-082018.html

From reimbursement landscape challenges to dwindling inpatient volumes, many factors lead hospitals to file for bankruptcy.
Here are six hospitals that have filed for bankruptcy protection since Jan. 1:
1. Rockdale, Texas-based Little River Healthcare, its parent company and several of its affiliated entities entered Chapter 11 bankruptcy July 24. One of the hospitals included in the bankruptcy filing, Crockett, Texas-based Timberlands Hospital, closed in 2017.
2. Florence (Ariz.) Hospital at Anthem entered Chapter 11 bankruptcy in late May after it failed to contest an involuntary bankruptcy petition from creditors within the required 21-day timeline.
3. Gilbert (Ariz.) Hospital, which is affiliated with Florence Hospital at Anthem, entered Chapter 11 bankruptcy May 24.
4. The Miami Medical Center, a 67-bed hospital that suspended services in October 2017, filed for Chapter 11 bankruptcy protection March 9. The hospital was sold in auction in late June.
5. Iron County Medical Center, a critical access hospital in Pilot Knob, Mo., filed for Chapter 9 bankruptcy Feb. 21. The hospital is owned by the Iron County Hospital District.
6. Surprise Valley Health Care District, which operates 26-bed Surprise Valley Hospital in Cedarville, Calif., filed for Chapter 9 bankruptcy Jan. 4.
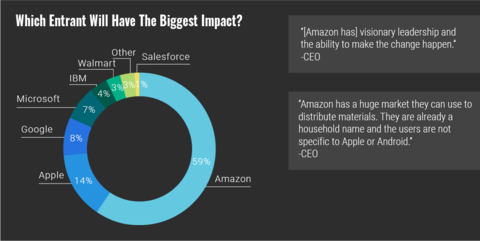
Out of all the technology giants with ambitions in healthcare, hospital executives have overwhelmingly put their faith in Amazon, according to a new survey.
A full 59% of executives say Amazon will have the biggest impact, according to the survey by Reaction Data. Respondents cited resources available to the retail and technology behemoth, the company’s current influence and name recognition.
Comparatively, 14% said Apple, with its foray into EHRs, would be the most influential, followed by Google at 8% and Microsoft at 7%
Among healthcare CEOs—which accounted for 26 of the survey’s 97 respondents—75% said Amazon would make the biggest impact.
About 80% of survey respondents were from the C-suite, including chief nursing officers, chief financial officers and chief information officers.
While Amazon alone may be generating significant excitement in boardrooms, a previous survey by HealthEdge shows consumers are largely skeptical about Amazon’s partnership with JPMorgan and Berkshire Hathaway.
Amazon’s push into healthcare “has been a shot across the bow for the entire industry,” Rita Numerof, Ph.D., president of Numerof & Associates told FierceHealthcare. The company’s consistent and deliberate investments indicate they are serious about making substantial changes within the industry.
“Amazon is known for its relentless focus on the consumer and its ability to use data systematically to identify and meet unmet needs in an accessible manner,” she said. “Unfortunately, access, consumer engagement, and segmentation haven’t been the hallmark of healthcare delivery.”
Executives were also bullish on telemedicine, with 29% saying the technology would have the biggest impact on healthcare, followed by artificial intelligence at 20%. That’s less surprising given that nearly 75% of respondents were already using telehealth in some way.However, 51% of respondents said telemedicine is revenue neutral, and key focus areas were split equally around rural patients, follow-up care and managing specific populations.

One of the country’s largest suppliers of oxygen and respiratory equipment has agreed to pay $5.25 million to settle allegations that it violated anti-kickback laws by reducing copayments for certain Medicare Advantage members.
Lincare has also entered into a corporate integrity agreement with the Office of Inspector General, the Department of Justice announced last week.
The settlement resolves allegations filed by former billing supervisor Brian Thomas, who worked for nearly a decade at the Florida-based company. In his 2015 complaint, which was later joined by federal prosecutors, Thomas claimed Lincare waived copays for Humana’s Medicare Advantage members beginning in December 2011 after the insurer contracted with Apria Healthcare to be an exclusive in-network provider of medical equipment.
In his complaint, Thomas said Lincare matched network benefits by reducing copays from Humana beneficiaries from 30% to 13% to align with copays from Apria. Humana was left paying for a higher charge using government funds.
Lincare was purchased by The Linde Group, a German industrial gas company, for $3.8 billion in 2012. The government alleged Lincare continued the scheme through 2017.
It’s the second major settlement for Lincare, which operates about 1,000 locations across the country. In May, the company paid $875,000 to settle a class action lawsuit from employers who had their information stolen during a data breach.

Anthem has entered a new partnership with retail giant Walmart to offer members access to over-the-counter (OTC) medications.
Beginning in January, Anthem’s Medicare Advantage members will be able to use OTC plan allowances to purchase medications and other supplies such as support braces and pain relievers, the two companies announced on Monday.
Previously, MA beneficiaries with OTC allowances could purchase medications through a catalog or by calling a designated number. Some members were provided a card they could use at a limited set of retail stores.
The new partnership significantly expands access to OTC drugs and supplies by allowing members to make purchases at any of Walmart’s 4,700 locations.
“The program with Walmart will allow consumers to pick the shopping method that best fits their lifestyle and the initiative is expected to significantly reduce the out-of-pocket cost burden for those enrolled in Anthem’s affiliated MA health plan,” Anthem spokesperson Hieu Nguyen said in an email.
Walmart says 90% of Americans live within 10 miles of a Walmart. The partnership will also give members access to free two-day shipping on orders $35 or more.
“We believe that programs like this can make a tremendous difference for healthcare consumers who often live on a fixed income or are managing chronic medical conditions,” Felicia Norwood, executive vice president and president of Anthem’s Government Business Division, said in a statement. Sean Slovenski, senior vice president of health and wellness at Walmart, said the company is “thrilled to be working with Anthem to provide its Medicare Advantage members with convenient access to our broad assortment of high-quality over-the-counter products.”
Interestingly, the partnership comes months after Walmart was reportedly considering an acquisition of Humana. Slovenski, the former vice president of innovation at Humana, joined Walmart last month.