The House voted Tuesday to repeal the excise tax on medical devices, with nearly five-dozen Democrats joining all but one Republican in backing the bill.
The measure was approved on a 283-132 vote that comes before lawmakers leave Washington for their summer recess at the end of the week.
The 2.3 percent tax on some devices sold by medical manufacturers was created under the Affordable Care Act. It is not set to take effect until 2020, following a move by lawmakers to include its postponement as part of the deal that ended a government shutdown in January. But lawmakers of both parties have long sought to repeal the tax, arguing that its enactment could lead to higher prices for consumers as well as the loss of tens of thousands of manufacturing jobs.
Fifty-seven Democrats joined 226 Republicans in approving the measure Tuesday night. The path forward in the Senate remains uncertain.
Start-up Bind uses proprietary algorithms, powered by machine learning, to lower health-care costs.
Bind discovered that it could break out certain procedures and reduce health benefit costs more effectively than with a high-deductible plan.
It is backed by Ascension Ventures, Lemhi Ventures and UnitedHealthcare.
Technology has made on-demand services a reality for everything from food deliveries to gym classes and car-sharing. What if you could have on-demand health coverage for big-ticket procedures like knee surgery?
On-demand health insurance seems like an oxymoron, but digital health insurance firm Bind is betting that by structuring health plans so that people can add coverage and pay for it when they need it, companies and employees can save money in the long run.
“It’s not intuitive for people, but I think when we started this we thought, ‘how do people really use the health-care system?’ And we used it in an on-demand way,” explained Tony Miller, co-founder and CEO of Bind.
The two-year old start-up is not a full-fledged insurer, it administers benefits for self-insured employers using UnitedHealth Group’sprovider networks and data analytics. Using its own proprietary algorithms, powered by machine learning, Bind discovered that it could break out certain procedures and reduce health benefit costs more effectively than with a high-deductible plan. It is backed by Ascension Ventures, Lemhi Ventures and UnitedHealthcare.
Plans are designed with basic co-pays and no deductibles for core medical coverage. In addition to free preventive care required under the Affordable Care Act, Bind’s plans cut out deductibles for primary care and specialist visits, maternity coverage, hospital care, medications and even cancer treatment. Co-pays are priced on a sliding scale — from $15 for a visit to retail clinic to $100 at an urgent care facility.
The big-ticket out-of-pocket costs kick in for elective procedures, such as knee replacement or back surgery. The extra co-pay for those procedures is based on the total cost, with consumers being given the full price of the procedure up front and no surprise bills on the back end. The co-pay can be structured so the worker can pay it off through payroll deductions, like a premium.
By outlining the total costs, Bind said it helps employees generate 10 to 15 percent in savings for themselves and for their employer compared to traditional out-of-pocket deductible plans.
“A market might be $6,000 to $24,000 for knee arthroscopy,” explained Miller. “What Bind does is says (for) the $6,000 performer — you only have to pay $1,000 to have access to them. If you want to go to the $24,000 knee arthroscopy with no difference in quality, no difference in performance, you have to pay $6,000 as a consumer.”
“What happens is the consumers actually go and buy the more cost-effective provider and they save money. But more importantly, the entire pool saves money … we save $18,000 for the group,” he said.
That was the way high-deductible plans were supposed to work, with consumers making the most cost-effective choice. Miller should know. He co-founded Definity Health in the late 1990s, which helped pioneer so-called consumer directed health plans; UnitedHealth bought that firm in 2004.
Does he worry that employers could use Bind’s on-demand plans to skimp on core benefits, and shift more costs to their workers? He does.
“What I would worry about is, taking this very novel plan design and if someone wanted to create a skinny plan out of it,” which he admitted would defeat the goal of Bind plan designs.
“Let’s make sure we fund the things we all need in health insurance and make sure that’s a part of everyone’s core benefit,” he said.
Bind has so far signed up small regional employers for its plan, but hopes to launch with a large Fortune 500 company for 2019 coverage.
As high health costs squeeze employers, managed care is making a comeback.
Nineties throwbacks have swept through music, television and fashion. Some startups want to bring a bit of that vintage feel to your workplace health insurance plan.
Health maintenance organizations drove down costs but were painted as villains in that decade for limiting patient choice, rationing care and leaving consumers to grapple with high bills for out-of-network services. But some features of the plans are regaining currency. Companies reviving the model say that new technology and better customer service will help avoid the mistakes of the past.
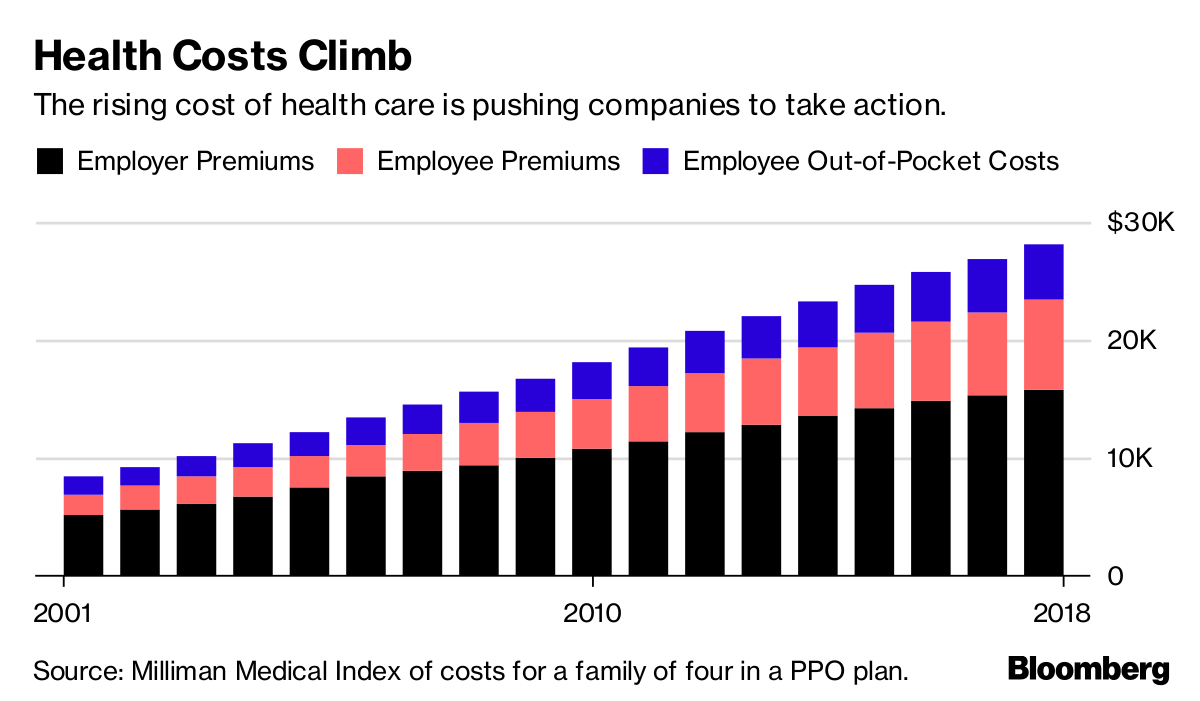
Rising health-care costs and dissatisfaction with high-deductible plans that ask workers to shoulder more of the burden are pushing employers to consider new ways of controlling spending—and to rethink the trade-offs they’re willing to make to save money.
Medical costs have increased roughly 6 percent a year for the past half-decade, according to PwC’s Health Research Institute, outpacing U.S. economic growth and eroding workers’ wage gains. Some employers, such as Amazon.com Inc., Berkshire Hathaway Inc. and JPMorgan Chase & Co.—wary of asking workers to pay even more—are trying to rebuild their health programs.
Barry Rose, superintendent of the Cumberland School District in northern Wisconsin, went shopping recently for a new health plan for the district’s 290 employees and family members after its annual coverage costs threatened to top $2 million.
“How do we provide quality, affordable and usable health care for employees,” said Rose. “I can’t keep taking money out of their paychecks to spend on health insurance.”
The company he picked, called Bind, is part of a new generation of health plans putting a tech-savvy spin on cost controls pioneered by HMOs.
Bind, started in 2016, ditches deductibles in favor of fixed copays that consumers can look up on a mobile app or online before heading to the doctor. Another upstart, Centivo, founded in 2017, uses rewards and penalties to nudge workers to get most of their care and referrals for specialists from primary-care doctors.
Health Costs Climb
The rising cost of health care is pushing companies to take action.
For many years, employers offered health plans that paid the bills when workers went to see just about any doctor, imposing few limits on care. The companies themselves usually paid much or all of the premiums.
Confronted with rising costs in the 1990s, many employers switched to HMOs or other forms of what became known as managed care. The switch worked, helping hold health costs down for much of the decade.
Soon, however, consumer and physician opposition grew amid horror stories of mothers pushed out of the hospital soon after childbirth, or patients denied cancer treatments. States and the federal government passed laws to protect consumers, and, in 1997, then-President Bill Clinton appointed a panel to create a health consumers’ Bill of Rights.
“The causes of the backlash are much deeper than the specific irritations or grievances we hear about,” Alain Enthoven, the Stanford health economist who helped pioneer the idea of managed care, said in a 1999 lecture. “They are first, that the large insured employed American middle class rejects the very idea of limits on health care because they don’t see themselves as paying for the cost.”
Workers would soon bear the cost, though. By the end of the decade, employers had moved away from these limited health plans. In their wake, costs skyrocketed, giving rise to a new cost-containment tool: high deductibles.
Centivo co-founder Ashok Subramanian spent the past decade trying to figure out how to offer better health insurance at work. His first startup, Liazon, helped workers pick from a big menu of coverage options. He sold it for some $215 million to Towers Watson in 2013, but he said it didn’t fix the bigger problem: Workers had lots of options, but none of them were very good.
“Yes, we were increasing choice, yes we were enabling personalization, but the choices themselves were not that good,” Subramanian said in an interview. “The choices themselves were predicated on a system in which the fundamental incentives in health care are broken.”
Tony Miller, Bind’s founder, helped give rise to health plans with high out-of-pocket costs. He sold a company called Definity Health that combined health plans with savings accounts to UnitedHealth Group Inc. for $300 million in 2004. He now says high-deductible plans failed to deliver on their promises.
“There’s a fever pitch of frustration at employers,” he said. “They’re tired of using the same levers that they’ve been using for the past 20 years.”
UnitedHealth, the biggest U.S. health insurer, helped create Bind with Miller’s venture capital firm and is an investor in the company, which has raised a total of $82 million. Bind is also using UnitedHealth’s network of doctors and hospitals as well as some of its technology.
Centivo has raised $34 million from investors including Bain Capital Ventures.
Centivo and Bind both promise to reduce costs for patients and employers while making it easier to find doctors and check coverage. They say they’ll reduce costs by making sure patients get the care they need, keeping them healthy and avoiding emergencies or unnecessary treatment.
Covered?
The proportion of Americans under 65 in health plans with high deductibles continues to increase.
In most cases, workers who follow the rules of Centivo’s plans won’t face a deductible. When signing up, employees pick a primary-care doctor, who’s responsible for managing their care and making decisions on whether they need to see a specialist. Care provided or directed by that primary physician is free, as is some treatment for chronic diseases such as diabetes, depending on how employers choose to set up the coverage.
The goal is to ensure workers get the care they need, while avoiding low-value treatments. Those who go to an emergency department in cases that aren’t true emergencies, for example, could face high costs.
“The big question is: Is the market ready for it?” said Mike Turpin, who advises employers on their health benefits as an executive vice president at USI Insurance Services. “The American consumer just has it built into their head that access equals quality.”
Bind bundles its coverage so consumers don’t get billed for lots of charges for services that are part of the same treatment. In Rose’s district, the copay for an emergency room visit is $250, while the cost of a hospital stay is capped at $1,000. Office visits are $35; preventive care is free.
Bind also offers what it calls on-demand insurance. Coverage for planned procedures such as knee surgery, tonsil removal or bariatric surgery must be purchased before the operation. That gives Bind a chance to push customers toward a menu of lower-cost alternatives or cheaper providers.
A patient who looks up knee arthroscopy, for instance, would also be offered physical therapy. The patient’s cost for the surgery ranges from $800 at an outpatient center to more than $6,000, in an example used by Miller. Surgeries in hospitals are typically more costly. Bind also charges more for providers who tend to be less efficient or have worse outcomes.
The ability to view costs upfront is part of what appealed to Rose, the Wisconsin superintendent. “Each of my employees knows exactly what they’re paying for, and they have choice in it,” he said.
Rose said the switch to Bind will save his district several hundred thousand dollars, depending on how much health care his workers need over the next year.
Lawton R. Burns, director of the Wharton Center for Health Management and Economics at the University of Pennsylvania, recently authored a paper with his colleague Mark Pauly arguing that it’s probably impossible to simultaneously improve quality, lower costs and achieve better health outcomes. The ideas now being pushed forward, he writes, are similar to ideas tested in the 1990s.
“It’s deja vu all over again,” he said. “It’s not clear to me, this is just me talking, that people have learned the lessons of the 1990s.”
The tech giant is looking to the former exec for guidance on addressing healthcare improvement in a way that could reduce burden on providers.
Toby Cosgrove, MD, the Cleveland Clinic’s former top executive, will share a stage Tuesday afternoon with several colleagues from his new employer: Google.
Cosgrove, who served as the clinic’s CEO from 2004 through 2017, signed on as an executive advisor to the Google Cloud Healthcare and Life Sciences team, the company announced in a blog post last week. An update to his LinkedIn profile indicates he’s been in the role since January.
As part of his new role, Cosgrove will join National Institutes of Health Chief Information Officer Andrea Norris for a conversation Tuesday about how advances in cloud computing are changing healthcare.
Those advances can help stakeholders go beyond achieving the triple-aim of healthcare improvement—better patient experience, improved population health, and reduced cost—to add a fourth aim, according to Gregory J. Moore, MD, PhD, vice president of healthcare for Google Cloud, who will moderate the conversation.
Although advances in technology have added to the recordkeeping burden on healthcare workers, people like Cosgrove can help companies like Google improve the work experience of physicians and their staff, Moore wrote in the blog post.
“Technology may have been the cause of some of these challenges, but we believe that it can also be the cure,” Moore wrote.
Cosgrove, who retired from Cleveland Clinic in January, also joined the board of Denver-based healthcare IT company RxRevu, as HealthLeaders Media reported last month.
Santa Clara County interested in buying O’Connor and St. Louise
Santa Clara County is hoping to buy a pair of struggling hospitals that have long served as a safety net for the poor, less than three years after they were sold to a New York hedge fund in a state-approved deal to ensure they remained open.
County Executive Jeff Smith said the county sees a renewed opportunity to acquire O’Connor Hospital in San Jose and St. Louise Regional Hospital in Gilroy as public hospitals to extend its reach and help relieve overcrowding at the county-run Santa Clara Valley Medical Center in San Jose.
“We’re watching carefully,” Smith said. “We’ve told them that we’re interested and asked them to let us know what their process is going to be.”
The county’s interest comes after Verity Health System, the Redwood City-based secular nonprofit that now runs the hospitals, announced the “potential sale of some or all” of the hospitals among options “to alleviate financial and operational pressures.”
It was less than three years ago that the Catholic Daughters of Charity, which provided medical care for California’s poor since the Gold Rush, announced the largest nonprofit hospital transaction in state history with the $260 million sale of six hospitals to a hedge fund.
The deal, blessed by a state attorney general under conditions that included facility improvements and no cuts to charity care, jobs or pay, was welcomed with guarded optimism: As hospitals struggle nationwide, a half dozen in the Bay Area and Los Angeles would stay open.
But already, the deal has soured. Verity saw operating losses of $55.8 million in the nine months that ended March 31.
The hospitals in San Jose, Gilroy, Daly City, Half Moon Bay and Los Angeles provide 1,650 inpatient beds, emergency rooms, a trauma center and a host of medical specialties, and employ 7,000.
But insurers are pushing to cut hospital stays to keep a lid on costs and premiums, shrinking hospital business. At the same time, demand for housing and commercial space has soared with California’s surging economy, raising the possibility that some of the hospitals could be turned into homes or offices.
Who would buy the hospitals, and what other alternatives are under consideration, is unclear. No hospital chains have announced interest.
“I don’t know of a system in California that would pick them up,” said Wanda J. Jones, a veteran health system planner and writer in San Francisco who has followed the deal.
San Mateo County officials could not say what might happen to Seton Medical Center in Daly City and Seton Coastside in Moss Beach, near Half Moon Bay.
“The potential closure of the hospitals and the impact on the residents they serve is very important to the county,” said Michelle Durand, spokeswoman for the San Mateo County county manager’s office. “However, we currently have made no decisions and also cannot speculate as to the potential interest of private hospital operators.”
But Santa Clara County officials have been vocal about their interest.
Daughters of Charity Health System had declined to sell the two hospitals to Santa Clara County because it wanted to sell all the hospitals as a package. After for-profit Prime Healthcare Services walked away from a potential $843 million deal to buy the six hospitals in 2015, calling then-Attorney General Kamala Harris’ conditions too burdensome, Daughters sold them to hedge fund BlueMountain Capital Management under similar terms.
A year ago, a Culver City company owned by billionaire doctor and entrepreneur Patrick Soon-Shiong, who also owns the Los Angeles Times and San Diego Union-Tribune, bought the hedge fund’s Integrity Healthcare division that owns Verity.
Smith said that in the current landscape for hospitals, O’Connor and St. Louise would always be money-losers for a private owner, but could pencil out as public hospitals. That’s because public hospitals get reimbursed by Medi-Cal, the state’s coverage for the poor, at higher rates than private hospitals, which rely on a mix of insured patients to cover charity care costs. O’Connor and St. Louise, he said, are in areas where they won’t attract enough insured patients.
For the county, acquiring O’Connor and St. Louise would make sense, Smith said. The county’s Santa Clara Valley Medical Center in San Jose is “filled to the brim with patients, and we have great need for services,” said René G. Santiago, deputy county executive and director of the Santa Clara Valley Health and Hospital System.
Some of the money to buy the hospitals could come from funds set aside for VMC renovation, Smith said.
But the six hospitals share debt and employee retirement obligations, which is what made Daughters of Charity unwilling to sell them piecemeal, Smith said.
There’s also the possibility that potential buyers may see greater use for some of the hospital properties for housing or offices. Smith said that while that wouldn’t satisfy the attorney general’s approval conditions, a seller could argue those terms were unworkable and seek a new deal.
Jones said the attorney general’s conditions made it impossible for the hospitals to survive in today’s environment, calling terms like no job cuts “insane.”
“Kamala Harris was so overboard in her requirement for what she wanted to happen,” Jones said. “You don’t put a condition like that on a buyer.”
The office of the attorney general, now under Democrat Xavier Becerra, had no comment.
Sean Wherley, a spokesman for SEIU-United Healthcare Workers West, which represents the hospitals workers, said when the possible sale was announced earlier this month that they were “disappointed.”
He said the union expects “Verity and any new buyer to be held accountable to keep hospitals open, maintain vital services, fund pension obligations, protect jobs and honor our collective bargaining agreements.”
Walmart’s $4 generic prescription drug program ends up being cheaper for some Medicare patients than their own health insurance, according to a new study released Monday.
It’s more evidence that patients cannot always rely on their health insurance to get them the lowest prices for their prescription drugs, said Dr. Joseph Ross of the Yale School of Medicine, who led the study.
“Patients were paying more out of pocket when they were using their insurance than when they went to Walmart,” Ross told NBC News.
The study, published in the Annals of Internal Medicine, documents that Walmart provides a better deal than the government’s health insurance plan for people over 65. And that is bad news for Medicare, because if people don’t take their drugs, whether for cost or for other reasons, they tend to get sicker and then end up costing even more to treat.
“Everyone’s talking about pharmacy costs these days,” Ross said. “We did this study in part because of all the discussion about pharmacy gag rules.”
Pharmacy gag rules prevent pharmacists from telling patients that they could save money on drugs, for instance by not using their health insurance.
Pharmacy benefit managers are the middlemen between drug companies and pharmacies, and some of those companies have agreements forbidding talk of discounts. But some states have also banned pharmacists from giving this information to customers.
One way patients can get around this is to ask, but few people think to do so.
Ross and colleagues decided to see what would happen if Medicare patients just took advantage of Walmart’s program offering $4 generic prescription drugs.
They looked at Walmart’s generic list for drugs commonly used to treat heart conditions, including high blood pressure and high cholesterol.
“Next, we used Medicare prescription drug plan data from June 2017 to determine beneficiary out-of-pocket costs for the lowest-priced dose of each drug in each plan,” they wrote. They got data on more than 2,000 Medicare prescription drug plans, including Medicare Advantage plans.
Overall, 21 percent of the plans asked patients to pay more out of pocket for the drugs than they would pay if they just got them for $4 at Walmart, the team reported.
Medicare Advantage plans were the most expensive for patients, Ross said. And the higher-tier programs were the worst, he found.
“Twenty percent of the time, at least, we should go to Walmart,” Ross said.
It doesn’t help that Medicare is very complicated. Patients can choose from dozens of different plans, depending on where they live, and it can take a great deal of research to find out which plan is most likely to cover a particular person’s health conditions for the least amount of money.
“Each Medicare drug plan has its own list of covered drugs (called a formulary),” the Center for Medicare and Medicaid Services says on its website.
“Many Medicare drug plans place drugs into different ‘tiers’ on their formularies. Drugs in each tier have a different cost. A drug in a lower tier will generally cost you less than a drug in a higher tier.”
Ross said it is time-consuming to compare one Medicare plan to another. But understanding one of the many plans tells people very little about what the others might offer.
“If you have read through the details and material for one plan, you have read through the details and materials for one plan. It’s very hard to compare,” he said.
In addition, any given plan may change the drugs that it covers and their prices throughout the year.
Ross said he studied Walmart because its $4 price for a 30-day supply of a generic drug seemed like the least expensive option, but other retailers also have inexpensive drug plans. Some grocery-based pharmacies even offer free drugs, such as antibiotics.
These offers get customers into the store, and the hope is that they’ll buy something else while they are there.
Ross said no patient should decide on a Medicare plan based solely on whether Walmart offers a better deal on prescriptions.
Switching plans might not be the best idea, because different plans provide different levels of coverage for doctor visits, medical procedures and other health needs.
“What we are showing is there may be some ways to save some money on some drugs by going to Walmart,” Ross said.
According to the Kaiser Family Foundation, about 90 percent of prescriptions filled in the U.S. are for generic drugs. Most people get health insurance through an employer, and the typical co-pay for a generic drug for a patient covered by employer-provided health insurance is $11, Kaiser found. For a brand-name drug, the average co-pay is $33.
Walmart is moving aggressively to get a big share of the U.S. health care market. Besides having large pharmacies, stores offer free health screenings and the company has said it intends to expand its locations of retail walk-in health clinics.
Walmart is also negotiating a closer partnership with health insurer Humana, including the possibility of buying it outright, according to CNBC.
The discount retailer’s $4 generic prescriptions beat Medicare’s co-pays 21 percent of the time, a study found.
Confidence is one of the defining characteristics of successful executives, but few CEOs felt prepared for their responsibilities, according to a survey in the Harvard Business Review.
Leadership advisory firm Egon Zehnder surveyed 402 CEOs from 11 countries between January and November 2017 and asked them questions regarding the challenges of stepping into a leadership position.
Four things to know:
1. There is no role that matches the demands of a CEO, and 68 percent of respondents said that, in hindsight, they weren’t fully prepared to take on the job.
2. Every CEO wants to drive culture change, but 50 percent of respondents said the task was more difficult than they expected.
3. Most CEOs know that they are only as effective as the people they surround themselves with, but 47 percent said that developing their senior leadership team was surprisingly challenging.
4. Forty-eight percent said that finding the time for self-reflection was harder than they anticipated.
Pfizer may have decided to roll back drug price hikes after being criticized by President Trump, but Bloomberg reports that several other large drugmakers are canceling or reducing planned price increases, perhaps in part because of a new California drug pricing transparency law that requires them to provide at least 60 days’ notice of price increases greater than 16 percent during a two-year period.
“In the past three weeks, Novartis AG, Gilead Sciences Inc., Roche Holding AG and Novo Nordisk A/S sent notices to California health plans rescinding or reducing previously announced price hikes on at least 10 drugs,” Bloomberg’s Ben Elgin, Cynthia Koons and Robert Langreth write.
The law is being challenged in court by the industry, but manufacturers have been complying while the case plays out.
Still, one industry analyst tells Bloomberg that the California law won’t actually slow the rate of price hikes. “If what you are trying to do is limit price inflation, this is not the way to go about it,” said Richard Evans, an analyst at investment research firm SSR. “This is not going to change mainstream list price behavior at all.”
Evans says that the drugmakers involved are probably just “throwing up a smokescreen” to hide the details of their price increases from competitors and patients.
Why it matters: These early results from California’s law might look encouraging, but it’s still a far cry from structural reforms that will keep prices in check.