

The Lines of Life
If Trump and RFK Jr. want to crack down on deceptive health care ads, they should start with the avalanche of misleading Medicare Advantage commercials blanketing seniors every fall.
The Trump administration announced last week it plans to crack down on prescription drug advertising. In reporting on the news, the New York Times quoted former Food and Drug Administrator David Kessler as saying that what the administration is proposing “would in essence remove direct-to-consumer advertising from television.”
In a press release, Health and Human Services Secretary Robert F. Kennedy Jr. said the intent is to “shut down that pipeline of deception and require drug companies to disclose all critical safety facts in their advertising.”
You’ll get no argument from me that companies of any kind, especially those that make money in health care, should not be allowed to deceive the public by withholding critical facts.
What I do argue – and hope this administration and Democrats in Congress will agree on – is that this crackdown should also include so-called Medicare Advantage ads.
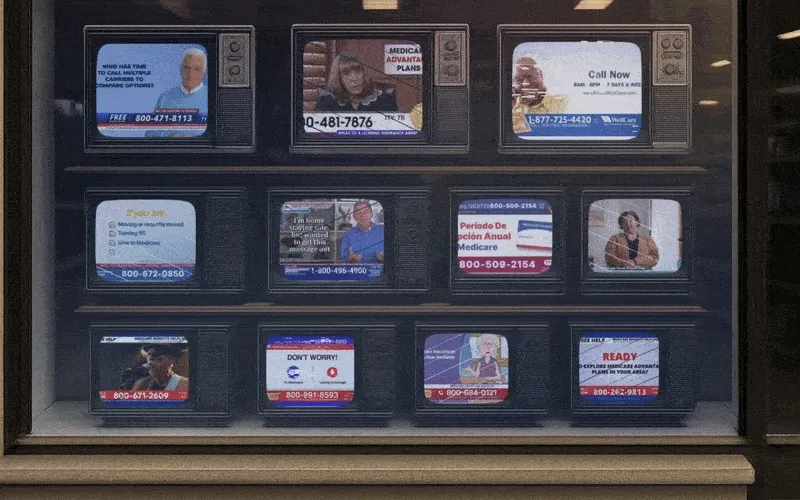
As we get close to “open enrollment” season, the period of time every fall when seniors and people with qualifying disabilities can choose between Traditional Medicare and one of many private health insurance plans, we already are beginning to see deceptive ads by Big Insurance to once again lure Medicare beneficiaries into their often deadly money machine.
You’ve seen the ads: happy, smiling seniors playing tennis or pickleball and gabbing about “free” groceries and dental benefits they presumably get because of the generosity of their MA plans. Nowhere – ever – have you seen or heard anything in any of those ads about the potentially lethal side effect of signing up for those plans. But the terrifying truth is that an untold number of MA enrollees have gone to early graves because their insurers delayed or outright denied a test, treatment or medication their doctors said they needed. Or because they couldn’t even find a high-quality doctor, hospital or skilled nursing facility close to their home – or even far away for that matter. Many centers of excellence – hospitals and clinics that are renowned for things like cancer and cardiac care – are not in many MA plans’ “networks.”
Seniors need to be told how limited MA networks can be – and that Traditional Medicare, by contrast, doesn’t even have networks. Traditional Medicare doesn’t restrict you to certain providers. That’s because almost all doctors, labs, clinics and hospitals participate in Traditional Medicare.
And seniors need to be told explicitly in ads what prior-authorization is and how it can affect them. And they need to be told about how much money they’ll have to pay out of their own pockets if they knowingly or unknowingly get care from an out-of-network provider. They also need to be told that their MA plans can and do drop doctors and hospitals from their networks during the course of a given year and that more and more physician practices and hospitals – including world-class facilities like Johns Hopkins and M.D. Anderson and the Cleveland Clinic – have dropped out of many MA networks. And they need to be told that their MA plan could very well dump them next year by “exiting” the community they live in, as Humana, Aetna, UnitedHealth and other plans did this year and plan to do next year.
Why, Mr. Trump and Mr. Kennedy, are MA insurers not held to the same standards as pharmaceutical companies? And how fast can you put standards in place to assure us that MA ads don’t omit “critical facts?” You know as well as anyone that between October 15 and December 7 (the open enrollment period) you won’t be able to turn on your TV or scroll through your social media feeds without seeing multiple MA ads that blatantly lie by omission.
Researchers at the nonpartisan KFF found TV ads hawking MA plans ran 650,000 times during the 2022 open enrollment period. You can expect that number will be surpassed this year because Medicare Advantage has become such a cash cow for Big Insurance. As just one example, UnitedHealthcare, a division of the biggest health care conglomerate in the world, got more than 75% of its revenue last year from Medicare and other taxpayer-supported programs. Now you know why those deceptive ads are so ubiquitous, and why private insurers lie with impunity.
Speaking of UnitedHealthcare, it co-brands its MA plans with AARP, which gives that corporation a kind of good seal of approval. AARP has received billions of dollars from UnitedHealthcare over the years as part of the relationship. To its credit, AARP called attention to that KFF study on its website just before the 2023 open enrollment season started. That’s notable, but AARP needs to do much more. So I am hereby calling on AARP to join us in demanding that both the Trump administration and Congress take immediate action to make sure MA ads cannot leave out essential information. Truthful MA ads are just as important as drug company ads. Maybe even more so when you consider all the potential harms MA plans inflict on seniors and people with disabilities every single year.
https://jamanetwork.com/journals/jama-health-forum/fullarticle/2837518
Privately administered Medicare Advantage (MA) has long been the subject of policy debate. To some, the once-nascent source of Medicare coverage is an important mechanism for injecting competition and innovation into the government-sponsored insurance program. To others, it represents an expensive and unnecessary alternative to directly administered traditional Medicare (TM).
After years of rapid growth, MA accounted for most program enrollments (33.6 million) and federal spending ($494 billion) in 2024.1 This has intensified some existing debates but also spurned increasing bipartisan agreements and interest in reforms. Politicians and policy experts who have historically supported MA, including some Republicans, have articulated greater openness to reforming the now-entrenched program.2 In effect, the debate has shifted from whether the MA program should be reformed to how it should be reformed and, critically, what the government should do with any savings. This Viewpoint discusses notable areas of consensus (and lack thereof) and the prospect of reforms from the Trump administration.
Areas of Growing Consensus
Several observations about MA are generally agreed upon. First, MA plans can use utilization management tools, like prior authorization, to constrain costs in ways that TM generally cannot. This reduces MA plans’ costs of covering Part A (hospital) and B (physician) benefits compared with a scenario where they imposed few constraints on utilization, like in TM. Policymakers also increasingly recognize the administrative burdens imposed on clinicians and restraints on patient access due to these tools, which have generated growing interest in reforms.
Second, and perhaps paradoxically, the federal government would spend less if all MA enrollees instead chose TM. This reflects several factors. MA plans are paid benchmark rates that are set above the fee-for-service spending in many counties. Plan payments can increase further due to the quality-bonus program. MA plans also have higher coding intensity, meaning the same beneficiary has more diagnoses recorded if they are enrolled in MA rather than TM. This increases risk scores and payments from the government (whether this reflects more accurate coding vs fraudulent behavior remains a source of debate). In addition, MA plans experience advantageous selection, meaning they attract enrollees who are relatively cheaper to cover conditional on their observable characteristics.3 All told, the Medicare Payment Advisory Commission estimates that the federal government spends 20% more (or an estimated $84 billion in 2025) than if all enrollees chose TM.1 While the exact magnitude of difference is subject to debate, the basic conclusion is not.
Third, MA plans offer more generous benefits to enrollees, including lower out-of-pocket costs and coverage of additional benefits such as vision and dental services. This occurs because plans keep a portion of the difference between their bid and the benchmark rate. These rebates average $2255 annually per enrollee, which represents 17% of all spending on MA.1
Where Disagreements Remain
While there is growing acknowledgment of the fiscal costs of the MA program, there is disagreement or uncertainty about several questions that inform an appropriate policy response. First, there is debate about how valuable some supplemental benefits are to enrollees. While it is relatively straightforward to value reductions in premiums or cost sharing in MA plans, there is limited information about how often enrollees use many of the supplemental benefits. Some research suggests that use of certain extra benefits may not be much higher in MA plans.4
Partly because of this, it is uncertain how much payment reductions to MA plans will reduce benefits and, in turn, how much that reduces enrollee welfare. Some research suggests the last dollar spent on MA plans results in much less than a dollar’s worth of additional benefits, particularly in markets with limited competition between plans.5 This suggests that reducing payments would initially lower plan profits but result in minimal welfare loss for enrollees. Even if true, it is not obvious when this tradeoff becomes more pronounced. Other research indicates the aggregate value of reduced cost sharing represents a large share of excess payments, suggesting reducing spending may quickly trigger benefit reductions.6 These effects may further depend on how policymakers chose to alter payments.
Finally, there remains significant disagreement about how to use any savings generated by program reforms. Democratic lawmakers often argue that savings should be used to increase TM benefits (eg, by adding dental benefits or imposing an out-of-pocket cap). Republicans are much more likely to pair spending reduction with policies that boost MA (eg, allowing MA plans to keep more of the savings if they bid below benchmarks). This predominantly reflects different preferences over the optimal structure of Medicare rather than empirical uncertainty.
Reform Possibilities From the Trump Administration
Many observers expect that the current administration will be relatively generous toward MA, as is typical of a Republican administration. This is particularly true given that the Centers for Medicare & Medicaid Services (CMS) administrator, Mehmet Oz, MD, has historically expressed support for MA plans. While major spending reductions may remain unlikely, early actions suggest the administration supports targeted reforms and is likely to test changes to the program’s design.
In his Senate confirmation, Oz was explicitly critical of strategic upcoding by insurers. Early policy decisions have been consistent with this view. The 2026 final payment notice for MA continues implementation of several policies that reduce MA payments. Notably, the Trump administration finalized implementation of an updated risk adjustment model that is designed to partly address coding intensity. For example, it eliminates approximately 2000 diagnosis codes that were judged to be most prone to upcoding. In conjunction with related changes, this is expected to decrease plan payment by 3.01%.7 CMS also announced the expansion of audits aimed at verifying the accuracy of diagnoses recorded by MA plans.8 This suggests the administration is willing to address strategic behavior by insurers, which they characterize as addressing waste, fraud, and abuse.8
However, the final payment notice also included higher payment increases for MA plans than was initially proposed by the Biden administration (5.06% vs 2.23%). After accounting for coding trends, realized payments are expected to increase by 7.16%. While consistent with an effort to boost MA enrollment, CMS noted that this change predominantly reflected the effects of higher-than-expected growth in per capita costs in TM, which mechanically increased payment updates. While CMS has some flexibility in payment updates, observers should use caution when using these upward revisions to infer the administration’s level of support for MA.
If the current administration is open to more novel and consequential reforms, they are likely to emerge from the Centers for Medicare & Medicaid Innovation (CMMI). While CMMI demonstration projects have historically focused on TM, the office can test changes to key features of MA that would significantly alter spending and incentives. Notably, Abe Sutton, JD, the director of the CMMI, recently highlighted the possibility of testing changes to risk scores, benchmarks, and quality measures, suggesting they are interested in taking advantage of this authority.9
With its place in the Medicare program now firmly established, MA has begun to attract more consistent interest in reform, even among Republican policymakers. This may reflect political considerations, as an unwillingness to act may provide an opportunity (and a source of budgetary savings) for future lawmakers to pursue alternative policy goals. Early signals from the Trump administration suggest they support program reforms, especially those targeting strategic behavior by insurers. Given the slim margins in Congress, it will be interesting to see if and how the administration uses CMMI’s authority to pursue substantive program changes.

Matthew Fiedler testified at a hearing held by the Subcommittees on Health and Oversight of the House Committee on Ways and Means to discuss the present and future of Medicare Advantage (MA).
His testimony made five main points on MA payment reform:

They were late filing a claim. Now I’m in collections.
Hey there —
I get a lot of questions from An Arm and a Leg listeners. Sometimes I write back with advice. So: Why not share? Welcome to an experiment: Our occasional advice column!
Maybe let’s call it: Can they freaking DO that?!?
Disclaimer: I don’t know everything, I’m not a lawyer, and I haven’t done new reporting for this. It’s the kind of advice I’d give a friend.
Or, in this case, a listener named Chris.
I had an emergency appendectomy. The hospital rang me up for about $47,000 — but, insurance denied the claim because they say the hospital didn’t submit it to them until eight months after the fact — beyond their 60-day “timely filing” limit in the contract [between the hospital and the insurance company].
After that, the hospital started billing me.
I have spent hours and hours on the phone over the last two months with various people in their billing department. I followed their recommendation to send a letter, and an email, requesting that they write off these charges since it was their billing error — and nothing has been fixed.
Now they’ve sent me to collections.
What do I do now? Do I sue? How can I sue? Help!
Chris
Chris, thanks so much for writing in — and YIKES.
I think you’re zeroing in on the right question, which is: How can you demand redress?
Put another way: Where’s your leverage? How can you get them to see they’re better off dealing with you in good faith, versus… getting themselves in actual trouble?
I don’t think you need to run out and hire a lawyer. But there’s a bunch of homework to do.
Because it’s their job to protect you from getting unfairly harassed like this.
Sounds like the hospital promised the insurance company — in a contract — to submit bills within 60 days.
That contract probably does not say, “and if we’re late on that, we’ll just go after Chris.”
No. I’m thinking it says, “If we don’t get you that bill on time, that’s just too bad for us.”
So: the insurance company has a right — and an obligation to you — to tell the hospital where to stick that bill.
So ask your insurance company: What’s *supposed* to happen if a hospital doesn’t submit a bill on time? What’s their process for getting things fixed? Can they tell the hospital to just knock it off, already?
And while you’ve got them, you may as well ask: If the hospital had submitted the bill on time, what would you have been on the hook for?
…because when this gets fixed, you’ll probably owe that amount.
If your insurance won’t cough up the info and won’t go to bat for you, get help. If you get your insurance through work, call HR. Otherwise, ring up your state insurance regulator.
Meanwhile, you’ve got the hospital siccing a collection agent on you. That’s not right.
Notify the collection agency that you’re disputing this debt, as described in this recent First Aid Kit — which includes a dispute-letter template. (While you’re at it, send a copy to the hospital billing office.)
Document your efforts to get the hospital to see the light on this. If you’ve written to them, attach copies of previous correspondence. If it’s been all phone calls, document them: You called them on this day, at that time, etc.
If you haven’t been logging calls — keeping a set of notes with times, dates, who you spoke to, and where things stood at the end of the call — start now.
Your state’s consumer-protection office might take a dim view of what the hospital is doing here.
I mean, I’m not a lawyer, but I’m pretty sure there are laws against chasing you for money you don’t actually owe.
Look up that consumer-protection office here. If you can talk with someone there, great. If your state’s consumer-protection laws are easy to find online (and understand), also great.
(If not, consider calling your local public library. Seriously, librarians are amazing at helping dig up useful information.)
Once you’ve got some sense of your legal rights — from the hospital’s contract with the insurance company, from your state’s consumer-protection laws…
Start writing letters. To the hospital, to the collection agency — saying: Let’s get this settled before I have to complain to regulators about this. (When you write to the hospital, maybe cc the General Counsel’s office.)
Let them know how you expect things to go, and indicate — subtly but clearly —that you know what kind of trouble they could be in and why.
And make it all as confident and calm as possible. I’m thinking of something the legal expert Jacqueline Fox told me once:
The person who gets the letter has to make the decision: “Do I ignore this, or do I bring it to my manager?”
And if I was that person and [the letter-writer] was very calm — just saying, “this is happening, and it’s starting to look like this [legal issue] and I want this to be handled according to your processes,” that’s the part I’d find alarming.
If I was that person, I would either make sure it’s handled according to my processes, or give my manager a heads up: that there’s a grownup who seems somewhat irritated.
Somehow, we never actually used that tape, even though I think about it all the time — until now. Thanks for the chance to bring it back.
Health care inflation hit a three-year high last month, in the latest sign that workers could soon be juggling big premium increases with higher prices for groceries, clothing and other items subject to President Trump’s tariffs.
WHY IT MATTERS:
Medical prices have been steadily rising, but corporations projecting increases of 9% or more next year are no longer willing to insulate their employees from the pain.
DRIVING THE NEWS:
Medical care costs rose 4.2%, compared with an overall inflation rate of 2.9%, the Bureau of Labor Statistics said Thursday.
THE BIG PICTURE:
Consulting firms are forecasting that the trend will carry over into next year, even without sector-specific tariffs on drugs.
BETWEEN THE LINES:
The rising costs are being felt beyond workplace insurance; Affordable Care Act marketplace plans are seeking median 18% premium hikes for next year, according to KFF. That’s the largest rate change insurers have requested since 2018, they said.
THE BOTTOM LINE:
Inflation is hitting health care harder than the broader economy, setting up a painful year ahead for both patients and employers.
The Trump administration has confirmed it will once again expand access to so-called short-term health insurance — which all too often fall into the category of “junk” insurance. They’re usually skimpy policies that do not meet the coverage requirements of the Affordable Care Act and that were largely reined in (again) by the Biden administration because of how devastating they can be for families with pre-existing conditions – or anyone who gets badly injured or sick.
Calling many of these plans junk insurance isn’t hyperbole. They’re called that because they are not designed to protect policyholders from financially crippling medical expenses. They’re built to look affordable upfront but in many cases leave people dangerously exposed when they need care most. Leslie Dach of Protect Our Care summed it up plainly:
“Short-term junk plans are allowed to deny coverage, drop people when they get sick, and exclude life-saving coverage such as prescription drugs and hospital care, leaving families with sky-high bills and nowhere else to turn”
Short-term, limited-duration insurance (STLDI) plans were originally designed as a stop-gap for people who needed catastrophic-protection between jobs. But starting in 2018, the ACA rules were loosened to allow these plans to last for a year and be renewed for up to three years, which inspired health insurers to jump in and begin heavily marketing them online as if they were real alternatives to traditional, comprehensive insurance.
Before the ACA, junk plans were not just short term, they were everywhere. The ACA outlawed much of what these STLDI plans do including refusing to cover basic medical services, excluding people with preexisting conditions, and spending only a fraction of policyholders’ premium dollars on care. There is a reason that the provisions preventing those abuses were some of the most popular in the ACA: They led to better care and lower costs for millions. These STLDI plans don’t cover needed care and only spend an average of 65% of the money patients pay in premiums on medical care, with some plans spending as little as 34% on care and keeping the other 66%. Expanding plans that do not adhere to patient protections in the ACA is not the way to fix our health care system.
As American Lung Association explains, most of these plans keep premiums low by cutting out what most of us think of as essential care: prescription drugs, hospital stays, mental health treatment, maternity care and more. They often cap how much they’ll pay in benefits, leaving families on the hook for huge bills if someone gets sick or injured. Unlike plans that comply with patient protections under the Affordable Care Act, they can deny coverage to people with asthma, diabetes, cancer or any other pre-existing condition.
Simply put, junk plans are the snake oil of the health insurance business, and advocates, including myself, have been sounding the alarm for years. On June 24, 2009, I testified before the Senate Committee on Commerce, Science, and Transportation and, for the first time, blew the whistle on how my old industry confuses their customers and dumps the sick. But I wasn’t alone on the dias. Nancy Metcalf, then senior program editor at Consumer Reports, sat to my left. Metcalf had much to say about junk insurance plans. In her written testimony, she wrote:
“As consumers, we are trained to look for a bargain. Buying a car or a flat-screen TV, we’re proud if we can get it for less than our friend paid. People think insurance works the same way. They never consider that if they are 55 years old, and have diabetes and heart disease, that no insurer could possibly stay in business selling them a comprehensive policy for $150 a month. That’s why so many of the junk policies we’ve looked at are marketed as “affordable.”
In my book, Deadly Spin: An Insurance Company Insider Speaks Out on How Corporate PR Is Killing Health Care and Deceiving Americans, I wrote an entire section titled “Selling the Illusion of Coverage” which focuses on junk plans and highlights how Cigna, Aetna and UnitedHealth made boatloads of money off buying companies that specialized in so-called junk insurance.
“Yet another scheme to shift costs to consumers and away from insurers and employers is to enroll them in limited-benefit plans. The big insurers have spent millions of dollars acquiring companies that specialize in these plans, often providing such skimpy coverage that some insurance brokers refuse to sell them.”
“There are so many restrictions built into limited-benefit contracts that there is always reduced risk to insurers, who appear only too happy to sell these policies to people who don’t realize they could be ill served.”
“Limited-benefit plans, coupled with high deductibles, represent the ultimate in cost shifting and are among the fastest growing health insurance products. They’re the future that insurers had in mind as they fought bitterly against reform that could jeopardize their profits.”
The Biden administration tried to put an end to this dangerous bait-and-switch. In March 2024, the Centers for Medicare & Medicaid Services (CMS) issued rules to once again limit short-term plans to a maximum of four months and require clearer disclosures so people would know what they were buying. As CMS Administrator Chiquita Brooks-LaSure put it:
“By making short-term plans truly short term, people will be more informed about the risks associated with these types of coverage and their options for comprehensive coverage.”
The Trump administration’s move to undo that rule means these plans can proliferate again and, as Protect Our Care noted in a statement, more than 100 million Americans with pre-existing conditions could be put at risk as insurers are once more allowed to deny coverage or drop people when they get sick.
This isn’t about politics. No matter who is in office, promoting junk plans is a bad idea. Families can get ruined when they think they’re covered — only to find out in the middle of a crisis that what they thought was a real insurance plan won’t pay for what they need. Short-term, limited benefit plans are the riskiest bet you can place in the U.S. health insurance casino. The house will always win.

Evernorth’s new latest investment in Shields Health Solutions ties its parent company, Cigna, even closer to hospitals and the fast-growing specialty drug market.
Regular readers will know that we’ve harped on UnitedHealth Group’s vertical integration into care delivery, pharmacy benefits and nearly every other corner of the health care landscape. But UnitedHealth isn’t the only company guilty of vertical integration: Cigna is playing the same game.
This week, Cigna’s health services arm, Evernorth, announced a $3.5 billion investment into Shields Health Solutions, a fast-growing specialty pharmacy company.
Shields partners with more than 80 health systems and over 1,000 hospitals and clinics across nearly all 50 states. That reach gives Cigna another way to weave itself into the daily operations of hospitals – and the lives of millions of patients.
When I was an executive at Cigna, the company was primarily what’s known as a third-party administrator. We sold some health and group life policies as an insurer, but our bread-and-butter was administering health benefits for large employers. Our “value proposition” back then was keeping costs under control — at least as we defined them. Evernorth didn’t exist. At the time, to me, the idea that Cigna would one day be pouring billions into specialty pharmacies and drug distributors would have seemed far-fetched.
In 2018, though, Cigna bought the huge pharmacy benefit manager Express Scripts. And soon after that, it created Evernorth to oversee its non-insurance health services operations, not only its PBM but also specialty pharmacies, and now investments like Shields. Cigna is no longer just deciding what care to cover, but it’s increasingly involved in how drugs are dispensed and priced. In fact, the company now gets the great majority of its revenues from the pharmacy business. Of the $195 billion in revenues Cigna took in last year, $154 billion came from Evernorth.
According to Reuters, Evernorth’s investment in Shields was structured as preferred stock and, according to the company, won’t affect its 2025 profit forecast. But make no mistake: This is part of the same playbook we’ve seen before from companies Americans have been led to believe are primarily insurers.
UnitedHealth buys physician practices, rehab centers, and home health companies. CVS Health owns Aetna, the PBM Caremark, and a sprawling pharmacy business. Cigna, for its part, is also planting stakes across the drug supply chain. In addition to Express Scripts, it also owns Accredo, one of the nation’s largest specialty pharmacies, and now Shields.
Cigna CEO David Cordani, who I once worked with during my time at Cigna, framed the deal as a way to “deliver exceptional care across healthcare settings – from home to physician’s office or clinic, to hospital”. In a statement on Evernoth’s website, Cordani said:
“Demand for specialty medications continues to grow at an accelerated pace, and Evernorth is uniquely positioned to serve the rapidly expanding number of individuals living with complex and chronic conditions and the doctors who care for them.”
Specialty medications, as Cordani mentioned, are among the fastest-growing and most expensive parts of the pharmaceutical market and include medications for cancer, multiple sclerosis, rheumatoid arthritis and other complex and chronic conditions. Research indicates that spending on specialty drugs will make up more than half of all U.S. drug spending in the coming years.
That’s why Evernorth already owns Accredo. Now, by getting into bed with Shields, Evernorth is tying itself even closer to the hospitals and health systems that rely on specialty pharmacies to serve patients.
When insurers buy into the businesses that are supposed to compete for contracts (like pharmacies and physician practices) it gives the insurer almost all the cards because they are able to both set the rules of the game and profit from it. Competition suffers, and costs for patients and employers can rise.
Fortunately, Washington is starting to wise up to these tactics. The Patients Over Profits Act, soon to be introduced by Sen. Jeff Merkley (D-Oregon) and Rep. Val Hoyle (D-Oregon), would prevent insurers from owning most doctors offices and medical providers. In addition, The Patients Before Monopolies Act, introduced by Sens. Elizabeth Warren (D-Massachusetts) and Josh Hawley (R-Missouri), prevents pharmacy benefit managers and/or health insurers from owning pharmacies. Given a divided Congress, these bills wont be easy to pass, but seeing strange bedfellows like Warren and Hawley taking the lead brings me great hope.
I saw firsthand during my years inside Cigna how Wall Street’s pressure for constant growth drives these decisions. Insurers and their shareholders aren’t satisfied with premiums alone. They want to control the entire pipeline — from the doctor’s prescription pad to patients’ wallets.
So the next time you hear about vertical integration in health care, don’t just think about UnitedHealth Group. Remember that Cigna is moving just as aggressively. With this latest $3.5 billion bet, it’s clear that the insurer I once worked for has transformed into something much larger — and far concerning — than the insurance company most folks believe it to be.


