https://www.forbes.com/sites/robertpearl/2017/11/14/disruptive-solutions-healthcare/#31b4ef452364

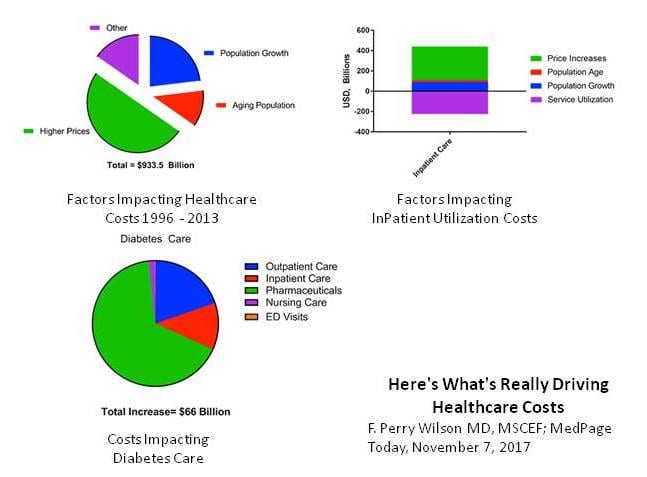
American healthcare needs a hero. Among other wealthy countries, it ranks dead last in clinical outcomes yet costs more than $3 trillion a year. By comparison, Europe spends $1.8 trillion annually on healthcare for a population nearly twice the size.
This three-part series, which previously explored the limited impact of primary care innovators and the struggles of U.S. hospitals, now concludes with the search for a hero – a disruptive cure for what ails the U.S. healthcare system.
Highlighted here are three possible directions the industry could turn and three trailblazing companies hoping to guide the way.
CareMore: In The Direction Of High-Touch Patient Care
Today’s healthcare is extremely people dependent. From receptionists, billing clerks and housekeepers to nurses, technicians and physicians, people account for more than 40% of all healthcare expenditures.
Therefore, one might assume lowering the cost of medical care means slashing headcount. Not at CareMore. The company spends twice as much on staffing as the typical healthcare organization – part of an approach that has proven remarkably successful.
Founded in 1993 as a medical group, CareMore was acquired by Anthem in 2011 and rapidly expanded its services across eight states. The company’s president and CEO Sachin H. Jain believes the best way to lower healthcare spending is to invest in the health of patients.
To do that, Jain hires large numbers of nurse practitioners, social workers, physician assistants and pharmacists. Located in care centers, these multidisciplinary teams help seal the cracks of America’s fragmented care delivery system.
In a recent Forbes editorial, Jain explained his hire-more philosophy: “Given the false choice between ensuring that I have the right processes and technology in place or the right people … I would choose the latter every day of the week.”
Indeed, people are central to CareMore’s strategy. But to understand why the company may prove disruptive, let’s dive deeper into its model, one that prioritizes disease management, limited specialty referral and reduced hospitalization:
- CareMore focuses on caring for the relatively sick, particularly low-income seniors enrolled in Medicare Advantage. This government-run program differs from traditional Medicare in that doctors receive a lump-sum prepayment for the expected cost of care, rather than receiving “fee-for-service” payments for each visit, test or procedure. Further, Medicare Advantage offers financial incentives to providers that keep patients healthier and avoid expensive hospital care. This is how CareMore is able to invest in a larger staff.
- The company invites the community doctors with whom it contracts to refer patients to CareMore care centers at no added expense. This controlled care-management process is a win-win for overburdened primary care physicians and for CareMore, whose nurse practitioners get to direct specialty referrals within their narrow network of providers.
- Today, 20% of elderly patients consume 80% of Medicare resources. That’s why CareMore hires “extensivists” to oversee complex patient cases both inside the hospital and on an outpatient basis. And because extensivists are trusted by their patients, they’re able to manage specialty referral, hospitalization and admissions to skilled nursing facilities in the most efficient ways.
- CareMore’s multi-disciplinary teams offer individualized programs for patients living with complex (and expensive) medical problems such as chronic lung disease, diabetes, heart failure and kidney dysfunction. And because chronic diseases are often associated with high levels of stress and depression, CareMore provides extensive mental and behavioral health services.
- The distinct power of CareMore derives from its synergistic approach, an end-to-end care model that not only maximizes quality outcomes and avoids complications from chronic disease, but also effectively controls specialty referrals and inpatient utilization.
This last point may be the most important. In some ways, CareMore’s model resembles other cutting-edge primary care programs that serve patients with chronic illnesses. But by using nurse practitioners and extensivists to personally manage referrals within CareMore’s cost-effective specialty network, the company goes a step beyond.
As a result, CareMore achieves 20% fewer hospital admissions, 23% fewer hospital days per patient and a 4% shorter inpatient stay compared to traditional Medicare beneficiaries.
The biggest question for CareMore is whether it will hit a ceiling. Its people-dependent approach could prove too difficult to replicate on a nationwide scale. As it tries to expand to new markets, CareMore may also encounter resistance from patients and the broader medical community given the narrowness of its specialty network.
Forward: In The Direction Of High-Tech Patient Care
Adrian Aoun, who created Forward in 2016, takes a decidedly different approach to solving healthcare’s biggest problems. With a background in artificial intelligence (AI), Aoun previously created Sidewalk Labs, an urban innovation project for Google and, before that, a news-aggregation startup that Google purchased for more than $30 million.
So, rather than hiring more people, Aoun uses sophisticated technology to reduce healthcare’s massive headcount and costs. He thinks computerized systems can diagnose and treat humans more accurately and affordably. And because human employees are more expensive and less-reliable than computers, you won’t find many of them performing traditional office roles at Forward’s San Francisco location, nor at the one set to open in Los Angeles. Instead, here’s what you will see:
- An iPad, not a receptionist, checks you in. From there, you step up to a sophisticated, space-aged body scanner and place your left hand inside the reader. In less than a minute, the machine records your pulse, oxygenation, height, weight and body temperature. The data is immediately input into your medical record and compared to past measurements.
- Inside the exam room, a technician uses “near infrared” technology to draw your blood before running tests at Forward’s fully automated in-house laboratory system. Your blood count, chemistries and genetic analyses for key markers are made available in less than half an hour and graphed against prior results.
- When a physician enters the room, there’s no large computer to sit behind and, therefore, no barrier between you, the doctor and the problem at hand. Your medical information appears on a large wall monitor that’s powered by a combination of AI and predictive analytics, with easy-to-follow graphics and voice-recognition commands. And since Forward’s members pay a $149 monthly fee with no copays or deductibles, data entry is designed to support care delivery, not billing and coding.
- Then there’s the AI system itself. Unlike commonly used algorithmic care that requires manual revisions, Forward’s technology learns as it goes. By analyzing a multitude of patient problems and treatments, the system ascertains which solutions are most effective. And with patients staying connected through a variety of wearable devices and computer applications, nurse practitioners and physicians know when a patient is likely to have trouble, even when that person is sitting at home.
- Finally, every health measurement taken at Forward is uploaded to the patient’s smart phone, making it easy for individuals to obtain data on their laboratory and clinical results.
As a primary care model, Forward’s approach is interesting but unlikely to disrupt the $3 trillion healthcare industry. The company’s uniqueness is in its technology, which is designed to scale up. Through high-tech devices and AI programming, Forward’s model could expand into high-end specialties. Already, the company is introducing automated eye refraction and digitally enabled melanoma screening at little or no extra cost.
Ask most doctors, and they’ll tell you Forward is not the future of medicine. Then again, technology aversion is the very thing that undid industry titans like Kodak, Borders and Yellow Cab.
Ultimately, Forward’s disruptive ability depends on how far and how quickly the company can broaden its scope beyond primary care. For example, will Aoun seek to hire a select group of specialists to consult with patients via video? Imagine the benefit of having top cardiologists and oncologists checking in on that giant wall monitor or via a patient’s smartphone. More importantly, can Forward convince insurance companies to carve out dollars from premiums to pay for the patient care delivered and for the hospital or specialty care avoided? If not, Forward’s going rate of $149 per month may restrict its footprint to the nation’s most affluent areas.
Health City: In The Direction Of Off-Shore Patient Care
Take a one-hour plane ride from Miami to the Grand Cayman Islands and feast your eyes on the palm-tree-lined entryway of healthcare’s third potential disruption. Health City is a sophisticated, modern hospital, offering affordable cardiology, pediatric, orthopedic and oncology services with clinical results that rival the best in the United States. Adjacent to the hospital, you’ll see the future site of a five-star hotel. Dr. Devi Shetty hopes to fill it with hundreds of Americans each night, thus making his healthcare tourism plans a reality.
Shetty, an India-born and American-trained surgeon, sees the future of healthcare differently than the leaders of CareMore and Forward. He believes 50% of the costs swallowed up by traditional care providers can be eliminated through discipline and operational excellence.
Shetty’s approach, like the other two, is complex. It includes:
- Highly efficient operating rooms. Health City completes more than twice as many surgeries per day as the average U.S. hospital. And rather than using the ORs five days a week, they’re scheduled for six. Instead of an eight-hour block, they run for 12. To accomplish this, Health City matches supply to demand to an exacting degree, quite unlike American facilities with their inadequate volume, inconsistent staffing and wasted capacity.
- Hyper-specialization. Higher patient volume per physician drives higher clinical quality at lower costs. That is, the more surgeons focus on a limited number of procedures, the better their performance and results. And by limiting number of procedures per physician, the more likely Health City is to achieve operational efficiency and innovate surgical techniques.
- Technology. IT needs to support clinicians, not vice-versa. At Health City, nurses and physicians carry their mobile devices everywhere, entering data on touch-screen interfaces to improve patient care, not to keep track of billing codes. The system is locally designed to analyze and provide immediate hospital data. As a result, physicians and administrators can see reports today on how to improve patient care tomorrow.
- Little to no delays. Walk into the administrative area of Health City and the first thing you’ll notice is a large computer screen reporting how long it takes physicians to respond to an elevation in a patient’s heart rate or higher than usual post-operative bleeding. In U.S. hospitals, delays in addressing patient problems often run an hour or longer on nights and weekends. Inside Health City, the average delay is eight minutes, with an aim of reducing it to six.
- A powerful mission. Health City is committed to “delivering world-class healthcare that is accessible and affordable for all.” It’s a core value built into the hospital’s culture, believed by all and evident in its outcomes.
Health City’s biggest challenge is getting patients to travel to the Cayman Islands for care. The objective data affirms the hospital’s clinical excellence and lower costs, but Americans distrust the medical care provided in other parts of the world. With most of its patient population hailing from the Caribbean and South America, Health City’s best hope is to contract with large, self-funded U.S. companies that want to cut their medical costs in half, particularly those organizations willing to offer employees incentives to combine their medical care with a tropical island vacation.
Will Healthcare Disruption Happen? How?
American healthcare is inefficient, ineffective and expensive. In other words, it’s ripe for disruption, which could happen a number of ways. It may be through highly personal care that effectively manages utilization and helps sick patients get healthier. Perhaps high-tech systems will replace expensive humans and create far better outcomes for patients. Or maybe an operationally efficient, off-shore solution will disrupt America’s bloated delivery system, just as it did the manufacturing and IT sectors.
CareMore, Forward and Health City represent three possible approaches to healthcare disruption, but it’s far too early to declare a hero among them. Combined, these companies care for a fraction of 1% of American patients. Should that number grow, it will likely come at the expense of the doctors and hospitals who benefit from today’s broken system. Unless healthcare providers in the U.S. are willing to embrace new solutions and care delivery models soon, they risk being disrupted. The cautionary lesson taught by other industries is that once disruption begins, it’s already too late for the old model to save itself.