The drug price hikes that are helping drive the health affordability crisis will continue for the rest of President Trump’s term, key industry stakeholders are now predicting —despite his deals with drugmakers and Medicare negotiating lower prices.
The big picture:
Insurers, drug supply middlemen and hospitals who represent 13% of all pharmaceutical purchases predict single-digit price increases for branded drugs over the next three years, according to a new survey by TD Cowen.
The increase will be largely driven by pricey new medications, such as drugs for cancer, diabetes and obesity, as well as cell and gene therapies, the purchasers said.
Drugmakers are already set to raise prices this year on at least 350 medications, including common vaccines and cancer treatments.
State of play:
Democrat and Republican policymakers have prioritized lowering drug prices in recent years in response to mounting public concern over health costs.
Congress during the Biden administration passed the Inflation Reduction Act, allowing Medicare to negotiate lower prices for select drugs.
Trump has made direct deals with drugmakers for decreased U.S. prices on certain products.
Yes, but:
TD Cowen’s latest annual drug purchaser survey shows these policy interventions aren’t driving prices down, at least in the near term.
Insurers, pharmacy benefit managers and other payers said they expect their cost of acquiring a drug to increase by 8%, on average, over the next three years. They gave the same figure when surveyed in 2024, 2023 and 2022.
Prices for generic drugs are predicted to increase by 2% over the same period.
“As long as biopharma delivers innovation, we see no change in the upward trend in drug prices,” TD Cowen wrote in its analysis.
By the numbers:
44% of purchasers surveyed expect Medicare drug negotiations to have a modest impact on cost, and another 30% said they don’t think they will have any impact.
But 74% said they think drug usage will increase over the next five years due to the policy changes and the IRA’s out-of-pocket cost protections for seniors.
Reality check:
Patients aren’t necessarily going to see an out-of-pocket increase as drug acquisition prices rise, due to rebates and other discounts.
But payers often pass increased costs along to patients, including by raising monthly premiums.
Net drug prices increased one-tenth of a percent in 2024 after accounting for rebates and discounts, per an IQVIA report published in April.
What they’re saying:
Patients “bear an unfair burden as out-of-pocket costs have risen faster than the net prices paid by PBMs and insurers,” PhRMA spokesperson Chanse Jones said. “At the same time, innovation … continues to skyrocket.”
Advocacy group Patients for Affordable Drugs said in response to the survey results that the IRA’s reforms are working for seniors.
“[T]hat’s exactly why expanding and protecting the law matters,” Alyson Bancroft, director of policy, legislation and alliances, told Axios in an email.
Health and Human Services communications director Andrew Nixon told Axios the agency doesn’t weigh in on third-party analyses, but said HHS continues to advance policies to lower drug costs so patients can afford treatments.
What we’re watching:
Purchasers expect coverage of obesity drugs to grow over the next three years.
Almost 30% of respondents said they currently have very limited coverage of GLP-1s for obesity, but nearly 20% said they expect to offer complete coverage for a finite amount of time within three years.
Medications for diabetes, obesity and rheumatological conditions were cited as likely to have the greatest decrease in price over the next three years. That’s due to coming patent expirations and increased competition among advanced products, TD Cowen noted.
In mid-December, members of Congress members left Capitol Hill for the final time in 2025, thus ensuring that the year would end with a failure arguably more significant than anything they accomplished during the prior 12 months: the end, despite a widespread public clamor for action, of subsidies put in place during the pandemic that made premiums of ACA marketplace plans affordable for millions of Americans.
Although important health care stories often fail to get much media attention, the failed efforts – mostly, but not exclusively, by Democrats – to save the Affordable Care Act/Obamacare subsidies were different. As patients from Maine to California opened their yearly renewal letters, many were shocked to see their monthly premiums for 2026 would be doubling or even tripling – right when the rising cost of living was already the No. 1 voter concern.
But there’s another aspect to America’s looming health care crisis that almost no one is talking about.
This is the other side of the coin – the out-of-pocket expenses that everyday consumers pay for doctor visits or prescription drugs – because of higher deductibles, or because of the growing number of patients who will risk not having any insurance at all next year because they can no longer afford it.
Even before the new year began, many Americans were dreading a double whammy of skyrocketing premiums and a sharp spike of what they expect to pay on top of that, out of their own pockets.
For example, Doug Butchart of Elgin, Ill., told ABC News that while his wife Shadene – who is living with the neurological disorder amyotrophic lateral sclerosis (ALS) – paid about $3,000 in out-of-pocket costs last year, that’s expected to rise as high as $10,000 in 2026, on top of monthly premiums that are tripling with government inaction on the ACA subsidies. It’s all more than the senior couple currently earns from Social Security.
Of course, millions of other Americans who switched to insurance plans that trade lower monthly premiums for sharply higher deductibles are taking an economic gamble that won’t play out until they see how healthy they are in 2026. In particular, those joining the surge of patients switching their ACA health coverage from the common Silver plan to the lower-premium Bronze coverage could pay thousands more as a result.
An analysis by KFF, the health care think tank, found that the average deductible in 2026 for patients who sign up for a Silver plan, assuming no reductions for cost sharing, will rise to $5,304, but for those who opt into a Bronze plan, the average deductible will spike to $7,576 – meaning a more than $2,000 higher outlay for sicker patients who max out on their covered expenses.
Katie Keith, director of Georgetown University’s Center for Health Policy and the Law and a former Biden administration aide, said the skyrocketing cost of insurance means “people are so premium sensitive that they might still go with Bronze and kind of leave money on the table – then they’re facing at least a $9,000 deductible, or whatever out-of-pocket max is, and just huge burdens.”
Keith and other health policy experts see a perfect storm of negative factors for higher out-of-pocket expenses in 2026 – from the impact of generally rising health costs to the added burden of government inaction or indifference in Washington. Among the factors behind a looming crisis:
Last summer, the Trump administration finalized new rules for the ACA that changed a key calculation and thus increased the maximum in out-of-pocket expenses that can be set by insurers – a ruling that also affects the millions of Americans who receive health insurance through a private employer.
The new math proposed by the Trump administration’s Centers for Medicare and Medicaid Services (CMS) adds yet another 4% hike on top of an already expected steep increase. The higher limit means individuals in some plans will pay $10,600 before their insurance kicks in, with a bump to $21,200 for families – an overall increase of 83% for individuals and 67% for families since the out-of-pocket maximum established by the ACA went into effect in 2014.
The Center on Budget and Policy Priorities reported that, because of these changes, a family of two or more people on the same plan could face an additional $900 in medical bills if a family member is seriously ill or injured in 2026.
Increasingly, employers are putting more of the economic burden on their workers for health care costs, especially through higher deductibles. For one thing, the KFF Employer Health Benefits Study has found that – for employees whose coverage carries a deductible, on individual plans – that average out-of-pocket cost has outpaced inflation and more than tripled in less than two decades, from $567 in 2006 to $1,887 in 2025.
What’s more, increasing pressure for workers to share the cost burdens of their health insurance has also caused more employer plans to offer a higher deductible option, and more people are signing up for that risk. Federal data shows that while only 38% of private-company employees had the option for a high-deductible plan in 2015, that number has now risen to more than half.
Perhaps the biggest factor is the end, for now, of the tax credits that had been holding down the cost of monthly premiums for ACA marketplace coverage since the COVID-19 epidemic. In states gathering data about early enrollment trends this past fall as higher premium notices went out, the shift away from traditionally popular Silver plans into Bronze coverage, with its higher out of pocket costs, has been dramatic.
For example, in California, where the Covered California program is considered a trailblazer in public health plans, officials told NBC News they’ve seen a “substantial” movement of enrollees choosing the Bronze plans with the highest out-of-pocket deductibles. Typically, officials reported, about one in five new enrollees go with the Bronze option, but for 2026 that number has soared to more than one-third. It’s a similar story in Idaho, where officials told NBC that Bronze enrollments are running 5% higher than normal, with most moving from Silver plans.
“There’s a lot yet to be seen, but there are definitely some early warning signs in terms of the decisions consumers are having to make in reaction to the changing federal policy,” Jessica Altman, executive director of Covered California, told the network.
Even more worrisome, however, is the number of Americans who are cancelling their ACA marketplace coverage altogether, because – all evidence suggests – they can no longer afford the premiums for any level of plan. In Pennsylvania, after families began receiving notices that – in many cases – their premiums had doubled, officials reported that about 40,000 people dropped their coverage, which is double the total from the 2024 enrollment period. What’s more, new enrollments in the Keystone State are also running about 20% lower than this time last year.
This is on top of a growing number of people – especially in the younger age brackets – who are switching to other low-cost alternatives that also are essentially a big gamble. These include so-called short-term plans, which are not compliant with ACA coverage requirements and that often come with annual or lifetime caps on coverage, don’t cover certain critical expenses like prescription drugs or paternity care and can penalize patients with preexisting conditions. There are also so-called catastrophic plans, which usually carry the maximum allowable deductible and which – in recognition of the worsening health insurance climate in the U.S. – have been expanded as an option to consumers over age 30. You may have even heard ads for faith-based sharing plans, whose members pool their expenses. People who sign up for those plans often find out they are not covered for a serious illness.
No wonder growing numbers of us are more anxious about the cost of health care than any time since the ACA was enacted in 2010 – perhaps ever. In November, a West Health-Gallup survey found that 47% of U.S. adults are worried they can’t afford health care next year – the highest number since the survey began in 2021. Those surveyed cited the rising cost of out-of-pocket requirements for prescription drugs in particular. And the number of Americans who say the cost of health care is causing “a lot of stress” in their daily lives has nearly doubled since the survey began, to 15%.
Georgetown’s Keith noted that – with patients and their families getting hit with higher costs on all sides – both the federal government and individual states have shown there are legislative actions that can reduce out-of-pocket costs for these anxious consumers. These include the federal No Surprises Act, which was signed into law by President Donald Trump in 2020 to address surprise medical bills, and a $2,000 annual cap on prescription drug costs for Medicare beneficiaries that went into effect in 2025 (it will rise to $2,100 this year), as well as various state efforts to curb tack-on facility fees or impose limits on insulin charges.
“There are many different flavors – ways that patients are getting charged,” Keith said. Indeed, that’s the bad news, since many of the fixes that lawmakers have been working on feel like bail-out buckets of water against a tsunami of rising medical expenses that in 2026 threaten the broader American economy, not to mention the national psyche.
Rising out-of-pocket expenses might be the looming health crisis that no one is talking about, but the lack of media coverage is likely to change over the course of 2026 as horror stories trickle in from those who gambled on not getting sick over the next 12 months – and lost that wager.
There’s a good chance your health insurance premiums are going up next year, regardless of where you get coverage.
Why it matters:
The spike in what millions of Affordable Care Act plan enrollees pay will be acute, but workplace insurance is getting more expensive, too — and all at a time when affordability is prominently on Americans’ minds.
ACA premiums have dominated the political discourse in Congress for weeks, but there’s no real sign that any relief is coming from Washington.
Even extending the Biden-era enhanced ACA subsidies — which most Republicans don’t want to do — would do nothing to address what’s driving the surging cost of care or employer insurance affordability issues.
And all signs point to Democrats hammering Republicans for high costs in all forms of health insurance leading up to next year’s midterm elections.
The big picture:
Health insurance gets more expensive almost every year, keeping up with increases in the costs of procedures, tests, drugs and more. But some years see bigger jumps than others, and 2026 is looking like one of those years.
That means tough choices for families, employers and workers all faced with shouldering higher premiums or out-of-pocket spending. Some will conclude it’s prohibitively expensive and go uninsured.
Another thing that’s different about this year is that the white-hot political rancor around ACA premiums is putting health insurance back centerstage politically.
By the numbers:
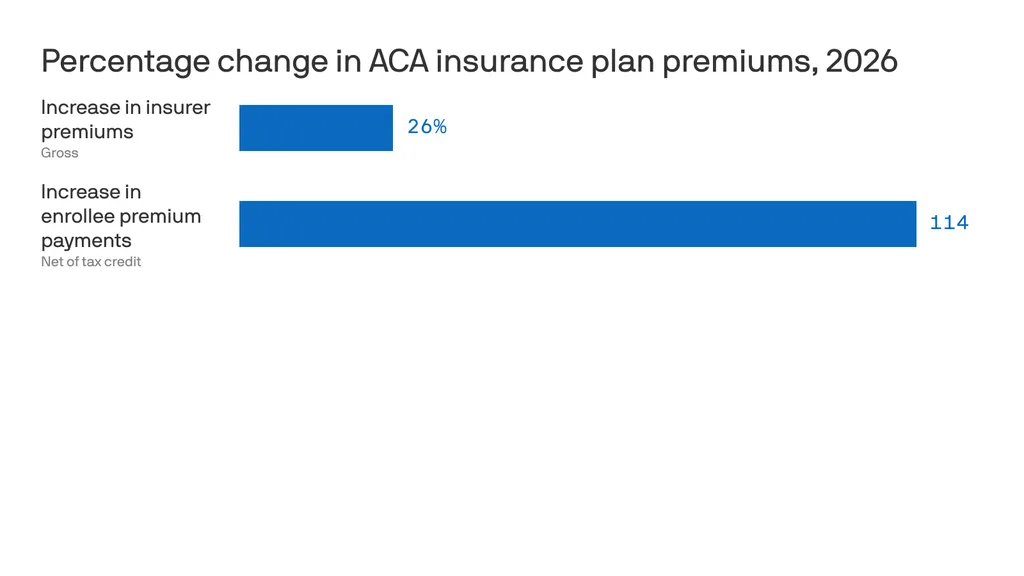
ACA insurers themselves are raising premiums by an estimated 26%, in part due to rising hospital costs, higher demand for pricey GLP-1 drugs like Ozempic, and the threat of tariffs.
But add in the loss of federal subsidies, and the increase is 114% — or more than double what they currently pay, according to KFF. 22 million out of 24 million marketplace enrollees now receive subsidies.
Premiums in the small group employer market will go up by a median of 11%, also per KFF, due to some of the same reasons insurers cite in ACA markets.
For employer health insurance, there’s no comprehensive data yet for 2026, but estimates from earlier this year put the increases in the high single digits.
There’s a good chance your health insurance premiums are going up next year, regardless of where you get coverage.
Why it matters:
The spike in what millions of Affordable Care Act plan enrollees pay will be acute, but workplace insurance is getting more expensive, too — and all at a time when affordability is prominently on Americans’ minds.
ACA premiums have dominated the political discourse in Congress for weeks, but there’s no real sign that any relief is coming from Washington.
Even extending the Biden-era enhanced ACA subsidies — which most Republicans don’t want to do — would do nothing to address what’s driving the surging cost of care or employer insurance affordability issues.
And all signs point to Democrats hammering Republicans for high costs in all forms of health insurance leading up to next year’s midterm elections.
The big picture:
Health insurance gets more expensive almost every year, keeping up with increases in the costs of procedures, tests, drugs and more. But some years see bigger jumps than others, and 2026 is looking like one of those years.
That means tough choices for families, employers and workers all faced with shouldering higher premiums or out-of-pocket spending. Some will conclude it’s prohibitively expensive and go uninsured.
Another thing that’s different about this year is that the white-hot political rancor around ACA premiums is putting health insurance back centerstage politically.
By the numbers:
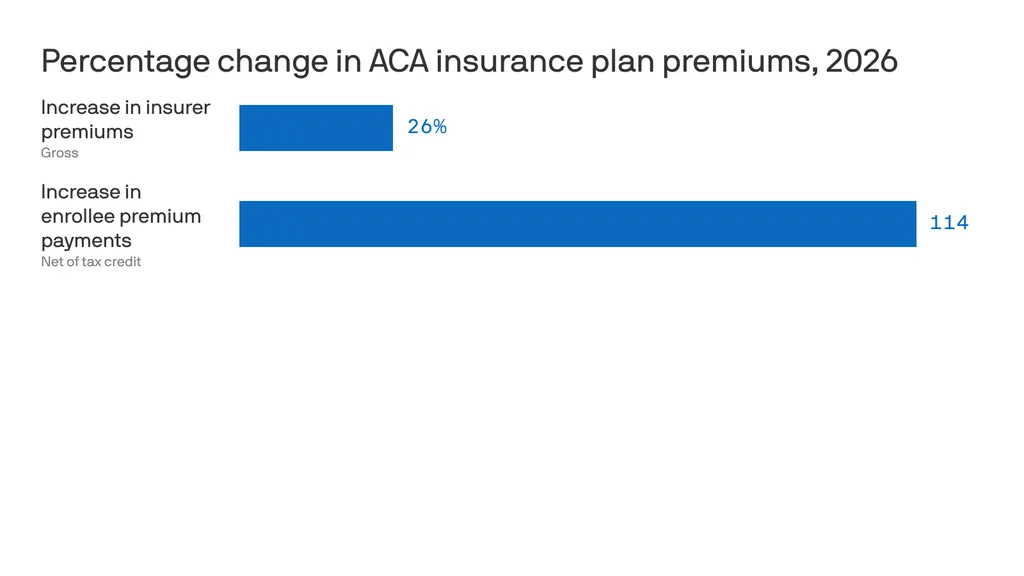
ACA insurers themselves are raising premiums by an estimated 26%, in part due to rising hospital costs, higher demand for pricey GLP-1 drugs like Ozempic, and the threat of tariffs.
But add in the loss of federal subsidies, and the increase is 114% — or more than double what they currently pay, according to KFF. 22 million out of 24 million marketplace enrollees now receive subsidies.
Premiums in the small group employer market will go up by a median of 11%, also per KFF, due to some of the same reasons insurers cite in ACA markets.
For employer health insurance, there’s no comprehensive data yet for 2026, but estimates from earlier this year put the increases in the high single digits.
For example, according to Mercer, health benefit costs are expected to increase 6.5% per employee in 2026, and many employers are planning to limit premium increases by raising out-of-pocket costs for employees.
One factor driving these increases is advances in medicines, like new cancer treatments, that are more expensive, according to Mercer.
But people are also using health care more, per Mercer. That’s possibly because they missed or delayed care during the pandemic — but also because the use of AI in doctors’ offices gives them more capacity and allows them to work faster.
Between the lines:
Just this month, Gallup polling found that approval of the ACA has hit an all-time high of 57%, including more than 6 in 10 independents but only 15% of Republicans.
Another recent Gallup poll found that 29% of Americans say that cost is the “most urgent health problem” facing the country, up from 23% a year ago.
The bottom line:
Get ready to hear a lot more about health care costs over the next year — while potentially also experiencing your own premium increase.
Next year, seniors and families will have more stringent and more unaffordable health coverage thanks to new AI-driven prior authorizations in Medicare and loss of subsidies in the ACA.
The New Year is just two weeks away, and when Americans wake after clinking champagne and kissing at midnight, the health care landscape in the United States will be in worse shape than it was in 2025. There is a growing list of why that’s true, but here are a couple of developments that will make it harder for many of us to get the care we need:
The December 31 expiration of the Affordable Care Act enhanced subsidies, which will lead to millions of Americans losing coverage and make premiums barely affordable for millions of others; and
CMS’s January 1 implementation of a new pilot project that will put private, for-profit contractors using AI-powered prior authorization in traditional Medicare.
Unless policymakers change course, many Americans will be ringing in 2026 with higher costs, less access and a nasty health care hangover.
WISeR strikes at 12
As we’ve reported, the implementation of the Wasteful and Inappropriate Service Reduction (WISeR) model’s will mark the first time in traditional Medicare’s 60-year history that for-profit companies will decide whether seniors receive certain medical services their doctors recommend. Six companies — many with deep ties to Big Insurance and insurer-backed venture capital — will suddenly have the power to say yes or no to 17 procedures that never required prior authorization before. And for these companies, the more the denials, the bigger the profits.
As Dr. Seth Glickman documented after sitting through CMS’s own WISeR webinar, the rollout has been vague on details and confusing to providers and patients. CMS even admitted during the webinar that the vendors chosen to administer the model were selected in part based on their “success” of using prior authorization in the private Medicare Advantage program, which is notorious for denials, delays and life altering decisions.
Some lawmakers in Washington have taken notice. A coalition of Democrats introduced the Seniors Deserve SMARTER Care Act, warning that WISeR creates “a dangerous incentive to put profits ahead of patients’ health.” Imposing prior authorization in traditional Medicare “will kill seniors,” said Rep. Mark Pocan, one of the bill’s sponsors.
Kiss subsidies goodbye
While WISeR threatens seniors’ access to care, millions of working families are facing a different New Year’s surprise: the expiration of enhanced ACA marketplace subsidies, which Congress has (so far) failed to extend or replace. As Rachel Madley, PhD wrote in October, families will have to gamble when they pick a health insurance plan. She added:
The enhanced premium subsidies being debated in Congress right now are a lifeline for so many of us and must continue in the short term, but they don’t fix the underlying problem: Private insurers extract value rather than control costs or provide access to necessary and affordable care. Decades of experience show that when profits rule health insurance, families face financial ruin no matter which plan they pick during open enrollment.
But as we’ve noted before, this isn’t an existential crisis for Big Insurance. ACA marketplace plans are not where insurers make their real money. Their profits flow increasingly from taxpayer-funded programs like Medicare Advantage and Medicaid managed care — the same universe WISeR is quietly expanding.
One proposal to “solve” the subsidy issue, endorsed by President Donald Trump and HELP Chairman Bill Cassidy, would not extend the tax credits but put $1000 to $1500 into government-sponsored health savings accounts (HSAs). HSAs can be helpful if you you have crappy insurance – or are rich and need an additional place to put your money to avoid taxes – but not a meaningful solution to the millions of Americans facing a 75% hike in premiums or finding themselves priced out of coverage altogether in 2026. The supporters of this approach claim it would somehow take money away from health insurers, but it would just reroute federal dollars to those same companies. For instance, UnitedHealth Group, which owns the nation’s biggest HSA custodian, could grab even more of our tax dollars than they already do. Meanwhile, families would still be exposed to unaffordable premiums and massive out-of-pocket costs. Champagne dreams.
Thanks to these changes in health care: The hangover on January 1, 2026, won’t only be from the previous night’s festivities – and it won’t be cured with some water and Advil. Cheers.
Yesterday aboard Air Force One, President Trump was asked by a reporter if he supported Senators Bill Cassidy (R-LA) and Mike Crapo’s (R-IN) new health care proposal, which would authorize $1,500 deposits in Health Saving Accounts (HSAs) for lower-income individuals to replace the expiring Affordable Care Act (ACA) subsidies. The president’s response to the question was telling. And it shows just how much Big Insurance has fallen from grace in recent months.
For decades, merely expressing disenchantment with private health insurers could get you labeled as a socialist. Now we are seeing daily criticism of health insurance companies from people across the political spectrum, leading one to not know if a quote like “Americans are getting crushed by health insurance with monthly payments” is coming from a progressive, like AOC, or a conservative like MTG. (Hint: that quote was from MTG). Trump’s response was in the same vein and could lead one to believe there is a chance of the left and right finding common ground in holding insurance companies accountable for their greed.
Where Trump is right. Where Trump is wrong.
Below we will dissect the president’s response and explain where he’s right and wrong.
“I like the concept [of the Cassidy-Crapo legislation]. I don’t want to give the insurance companies any money. They’ve been ripping off the public for years.“
This is true. Big Insurance has been ripping us off for years. And almost all of insurers’ growth in recent years has come from us as taxpayers. Most big insurers now make far more money on the lucrative Medicare Advantage business and managing state Medicaid programs than from their commercial health insurance plans. And they’ve even figured out how to bilk the VA.UnitedHealthcare, the biggest insurer, now gets more than 75% of its revenues from taxpayer-funded programs. And yes, insurers are getting hundreds of billions of dollars every year from the ACA subsidies that are at the center of debate in Washington.
Here are a couple of examples. Private health insurers took in over $500 billion in tax dollars to administer Medicaid in 2023. And this year alone, they will be overpaid – yes overpaid – $85 billion as a consequence of how they’ve rigged the Medicare Advantage program.
Insurers also take in massive amounts of money in the form of premiums that people pay thinking that money goes to care. Much of that money ends up going toward things (and people) that do nothing to get us well or keep us well. Since 2014, the seven largest insurers have made over $500 billion in profits, and they used $146 billion to buy back their own stock. So yes, Trump is correct, health insurance companies have been ripping people off for years.
“Obamacare is a scam to make the insurance companies rich.”
No, Mr. President, the ACA is not a scam and most Americans now know that it has done a lot of good for a lot of people. Among other things, it made it possible for millions of people who previously had been blackballed by insurers because of a preexisting condition to finally get coverage. It brought us many long-overdue consumer protections, outlawed junk insurance, enabled young people to stay on their parents policies until they turned 26, alleviated job-lock through the creation of the ACA (Obamacare) marketplaces, and it made millions more low-income families eligible for Medicaid.
But, the president is right to say that Big Insurance has gotten rich since the passage of the ACA. Between 2014 (the year the entirety of the ACA was implemented) and 2024, just seven for-profit health insurers amassed $543.4 billion in profits and took in a staggering $10.192 trillion in revenues.
“And they have made, I mean, you look, $1,400 to $1,700 increase, 100 percent increase over the last number of years. There’s really few things that have gone up like insurance companies.”
The president is kind of right. As KFF reports, the cost of a family policy has increased 60% since 2014 – a rate of increase much higher than general inflation and also higher than medical inflation. And as we’ve published previously, not only has the total cost of an employer-sponsored plan skyrocketed, so has the share of premiums workers must pay. This year, employers deducted an average of $6,850 from their workers’ paychecks for family coverage, up from $4,823 in 2014. And keep in mind, all that money our employers are having to send to insurance companies is not money that’s available to give raises to workers or hire more people.
“They’re getting numbers and money like nobody’s ever seen before. Billions and billions of dollars is paid directly to insurance companies. We’re not going to do that anymore.”
The president is right. Several Big Insurance companies have ballooned in size over the past decade to become some of the world’s biggest corporate conglomerates. UnitedHealth Group, CVS/Aetna and Cigna are now numbers 3, 5 and 13 on the Fortune 500 list. The only American companies that take in more revenue than UnitedHealth are Walmart and Amazon.
“I believe Obamacare was set up to take care of insurance companies, not to take care of the American public.”
The president has his history wrong here. While there are plenty of Monday-morning-quarterbacking you can do for the ACA – the law was not passed to “take care of insurance companies.” While the ACA didn’t fix everything – not by a long shot – it did stop some of the insurance industry’s worst abuses, like refusing to sell policies to people with preexisting conditions – even acne – and “rescinding” policies to avoid paying for life-saving care. Some insurers were found to be paying employees bonuses to find policies to rescind, including the policies of women almost immediately after being diagnosed with breast cancer.
It prohibited health insurers from charging people more because of a preexisting condition and from dumping the sick so they could reward their shareholders more generously. Keep in mind that insurers consider every claim they pay as a loss, hence the term “medical loss ratio” (MLR), which the ACA addressed by requiring insurers to spend at least 80%-85% of our premiums on our health care.
And it’s not like Big Insurance wanted the ACA to pass. Back in 2010, America’s Health Insurance Plans (AHIP), the PR and lobbying group for health insurers, quietly funneled $100 million to the U.S. Chamber of Commerce to orchestrate a PR, advertising and lobbying blitz to keep the ACA from being passed.
While big health insurance companies have only grown since the passage of the ACA, it has been Big Insurance’s corporate maneuvers and work on Capitol Hill (not the law itself) that has allowed these companies to flout some of the ACA’s regulations and bend the law to do their will.
“I love the idea of money going directly to the people, not to the insurance companies. Going directly to the people. It could be in the health savings account. It could be a number of different ways.”
While that is a compelling sound bite, it’s disingenuous. The money proposed by Cassidy and Crapo to go to HSAs would then be used by enrollees to buy insurance, thus still giving money to the insurance companies. Even worse, the proposed amount of money to go to people’s HSAs to help them pay for health insurance and care is $1,000-$1,500. This is money that would be used to purchase a bronze or copper plan with a high deductible (with many of those plans having deductibles north of $5,000). That means under this plan people would still need to come up with thousands to meet their deductible on top of paying their premiums every month. $1,000 wouldn’t come close to even covering the premiums for a decent policy, much less the out-of-pocket costs.
Replacing ACA subsidies with HSAs would still keep Americans tied to the same private health insurers that Trump calls “big, bad” and “money-sucking.”Most families would still be exposed to crippling medical bills, and even more tax dollars would flow to insurance conglomerates that own HSA custodian businesses (like UnitedHealth’s Optum Bank).
“And the people go out and buy their own insurance, which can be really much better health insurance, health care.”
That’s wishful thinking far removed from reality. The health insurance plans available to people who get money for their HSAs under the Cassidy-Crapo proposal – rather than getting subsidies – are the same as those currently available. Worse, without the subsidies, people will not be able to afford the gold or silver plans that have lower out-of-pocket costs. In reality the plans that people buy under the proposed Cassidy-Crapo plan would have less value than the plans they previously bought with subsidies.
Trump’s comments are coming ahead of tomorrow’s scheduled vote in the Senate on dueling Democratic and Republican proposals to deal with the enhanced subsidies for ACA plans that will expire in three weeks. Without those subsidies, premiums will spike for many of the 24 million American enrolled in “Obamacare” plans. Democrats want to extend the subsidies for three years. Republicans, led by Senate Majority Leader John Thune, will push a plan replacing those subsidies with direct payments into individuals’ Health Savings Accounts (HSAs), as the president is suggesting. Neither plan is expected to get the 60 votes required for passage. What happens next is anybody’s guess.
Over 17 million nonelderly Californians (55%) received health benefits through an employer in 2023. The California Health Benefits Survey (CHBS) tracks trends in these workers’ coverage, including premiums, employee premium contributions, cost sharing, offer rates, and employer benefit strategies. In 2025, the survey also included questions about provider networks, coverage for GLP-1 agonists, premium cost drivers, and employee concerns about utilization management. The CHBS is jointly sponsored by the California Health Care Foundation and KFF.
KEY FINDINGS INCLUDE:
Premiums for covered workers in California are higher than premiums nationally. The average annual single coverage premium in California is $10,033, higher than the national average of $9,325. The average annual family premium in California is $28,397, higher than the national average of $26,993.
Overall, the average family premium has increased annually by 7% in California and 6% nationally. The average single premium has increased 8% annually in California and 6% nationally. Since 2022, the average premium for family coverage has risen 24% in California, higher than national measures of inflation (12.2%) and wage growth (14.4%).
Workers are typically required to contribute directly to the cost of coverage, usually through a payroll deduction. On average, covered workers in California directly contribute 14% of the premium for single coverage and 27% for family coverage in 2025. These shares vary considerably, and some workers face much higher premium contributions, especially for family coverage.
A lower share of covered workers in California face a general annual deductible for single coverage than covered workers nationally (75% vs. 88%), and the average deductible is lower ($1,620 vs. $1,886). The share of California covered workers with a deductible has increased since 2022 (68% to 75%).
Employers in California are significantly less likely than employers across the nation to say there were sufficient mental health providers in their plans’ networks to provide timely access to services.
Many employers report concerns about out-of-pocket costs: 47% of firms offering health benefits indicate that their employees have a “high” or “moderate” level of concern about the affordability of cost sharing in their plans. About one in 10 covered workers in California faces a general annual deductible of $3,000 or more for single coverage.
Large California employers view drug prices as a major driver of rising premiums. Thirty-six percent of large firms report that prescription drug prices contributed “a great deal” to premium increases.
Over one-quarter of large firms (28%) offering health benefits in California say they cover GLP-1 agonists when prescribed primarily for weight loss. Nearly one-third of these firms report higher-than-expected utilization of this benefit.
Read the full report on the KFF website or download it below.
Structural, regulatory and competitive changes will alter the landscape.
10 areas will likely be the foci.
Last week…
the stock market took a dive largely due to tech company volatility resurrecting fears of an A.I. bubble.
reports from the Departments of Labor and Commerce confirmed mixed signals about the economy: job growth was relatively strong but inflation (3%) remained stubbornly above its 2% target and consumer confidence slid.
Target warned Black Friday sales later this week will likely signal softness in consumer spending, and
Congress returned to DC after its 43-day shutdown that ended with no agreement on extension of insurance tax credits that expire at year end.
This week, Thanksgiving will likely slow down things on the U.S. domestic front but not for healthcare. Unlike just about every other industry in the economy, we operate 24/7/365. And like some industries, demand for our services is hard to predict– acts of God, accidents, court decisions, regulatory policy changes, social media “experts” et al. make predictions educated guesses at best. New technologies, clinical innovations, A.I. and private capital keep planners off-balance. Short-terms plans are more defensible; longer-term plans more challenging.
Thus, the industry is understandably focused on 2026. Here are assumptions:
Affordability for groceries, transportation, housing and healthcare (premiums and out-of-pocket) will drive media attention, public opinion and voting November 3, 2026.
Congress will not extend tax credits that expire at year-end prompting a spike in the uninsured and under-insured populations. In tandem, large private insurers will raise premiums and increase leverage with providers to reduce competitive threats.
Media coverage of healthcare will feature sensationalism, soundbites and hyper-simplification: costs (affordability), prices, disparities, executive compensation, outcomes, community benefits, workforce dissatisfaction, profitability and business practices will be foci.
Warfare between hospitals, insurers, and drug manufacturers will intensify. Each will assert their systemic reform proposals serve the greater good best by protecting themselves against unwelcome threats.
States will be the epicenters of health system transformation. Federal changes will be paralyzed by partisan-brinksmanship and posturing for 2026 and 2028 elections.
Trust and confidence in the health system will decrease (further) to record levels of discontent.
And, reflecting on the current state of affairs in U.S. healthcare, here are 10 healthcare headlines you MIGHT see next year:
Employed physicians win class action challenge to hospital employment agreements citing clinical independence, excessive administrative costs concerns
IRS cuts not for profit health systems tax exemptions. Private investments, community benefits, executive compensation cited
UnitedHealth Group completes acquisition of HCA: sets stage for new era of competition in U.S. healthcare
EPIC completes interoperability agreement with CMS: public-private oversight board named
Congress passes most favored nation pricing for biologics, specialty drugs as states enact price controls
Large employers drop employee coverage due to costs, systemic flaws in system
Health and wellbeing services consolidated under HHS to integrate social services and health
Primary care physicians, nurse practitioners, community pharmacists launch national society to advance primary and preventive health services
CMS capitates, expands primary care services in restructured MSSP program
National coalition launched to design transformed system of health that’s accessible, affordable, comprehensive, efficient and effective
And, I’m confident, many others.
2026 is a mid-term election year. In 2016 (Trump 45 Year One), Republicans controlled 31 governorships and 68 legislative chambers. This January, the GOP will control 26 governorships and 57 legislative chambers– a 15% reduction on both. Politics is divided, affordability matters most to voters and healthcare is a high-profile target for campaigns so humility, thoughtful messaging backed by demonstrable actions will be an imperative for every healthcare organization.
2026 is a HUGE year for U.S. healthcare. The outcome is unknown.
I know plenty of people who are politically right-of-center – and they want to rein in Big Insurance just as much as people to the left.
Some of my closest family and friends have nearly polar opposite political beliefs than mine. And these are not family members I’m only with on holidays (like during Thanksgiving dinner later this week) or friends I only see on Facebook. These are people I love and communicate with weekly — sometimes daily. They’re my people.
And I’d say that my people largely fall into two distinct right-of-center sub groups:
The first group:
USDA grass-fed Trump supporters who like Jeanine Pirro and Blue Lives Matter bumper stickers.
And the second group:
Nonpolitical and anti-establishment 20-30 somethings who make their own beef-tallow.
(And both groups are patient enough to keep a Bernie-t-shirt-owning-lib, who listens to The Daily (like myself) in their lives.)
We don’t all agree on vaccines. We don’t all agree on the Gulf of America. And none of them agree with my mullet. But what we all do agree on is that through backroom deals and moneyed influence, big corporations pull Washington’s levers and squeeze American families at every chance they get – all to make their Wall Street investors and executives richer. And, as readers of HEALTH CARE un-covered undoubtedly know, Big Insurance may be the perfect example of those deals and influence.
That’s where my people and I meet in our venn diagram. While we have many sticking points, Big Insurance is not one of them.
And this is not just qualitative on my end. Poll after poll proves that my people are not the exception to the rule. An October KFF poll showed that a majority of Republicans who align with the MAGA movement (57%) said Congress should have extended the enhanced premium tax credits for Affordable Care Act (ACA) plans, and a new study by Undue Medical Debt found that 62% of Republicans blame health insurance companies the most for the medical debt crisis in the country.
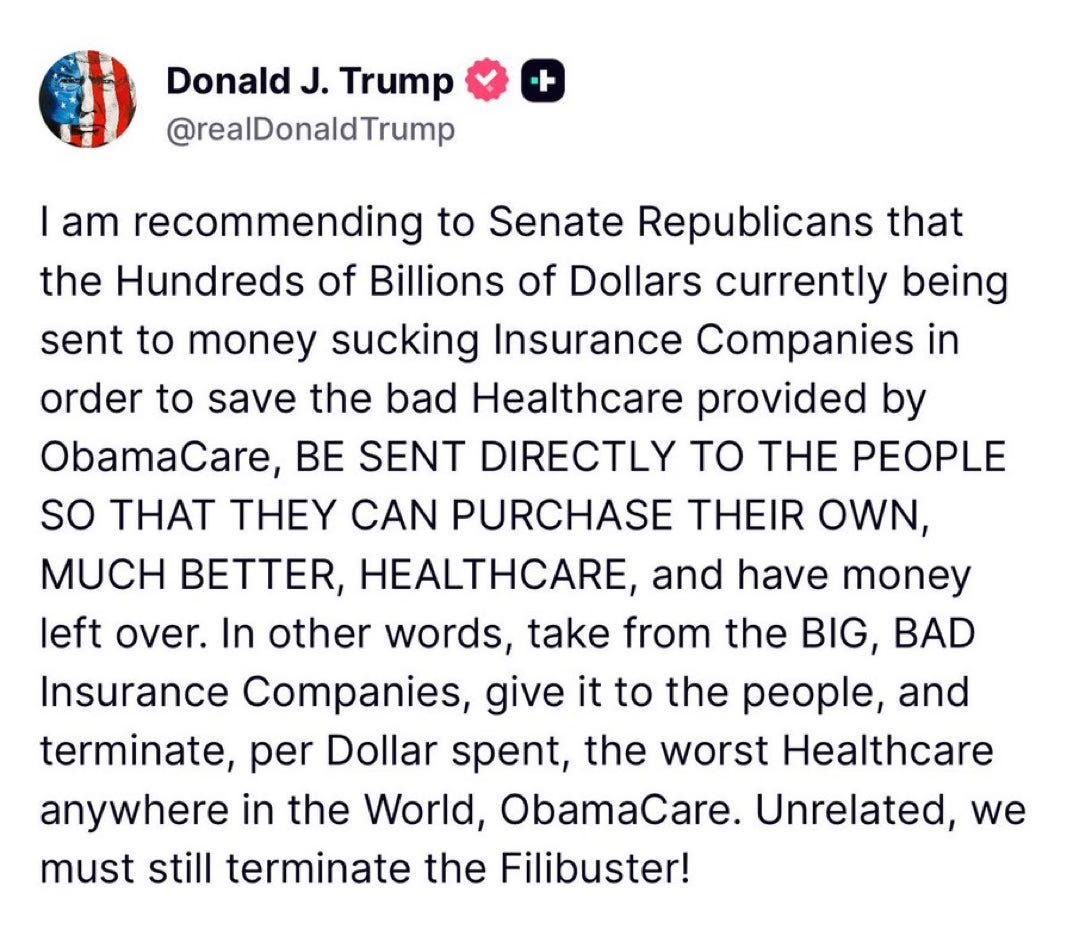
The deeds of the health insurance industry have grown so rotten and their stench so unavoidable that even the President has caught a whiff. On Truth Social last month, President Trump posted about “BIG,” “BAD” and “Money sucking” health insurance companies. His message reverberated in the media and on Wall Street and helped bring this issue even more to the forefront.
President Trump’s post on Truth Social attacking the health insurance industry.
But here’s the thing: Trump’s post isn’t the tip of the spear but rather the caboose following a long train of Republicans (and their voters) who as of late have begun to focus on Big Insurance. In the last six months, we’ve seen Representative Marjorie Taylor Green call on Republicans to take on Big Insurance, former Representative Mark Green (R-TN) introduce legislation to crack down on Big Insurance’s prior authorization tactics, and Pam Bondi’s Department of Justice open a criminal investigation into UnitedHealth Group’s Medicare Advantage business – all moves that have been historically uncharacteristic of their political bents but nonetheless are, in one way or another, raising the heat on Big Insurance.
If the latest news out of Washington tells us anything, it’s that conservatives are largely on the same side as many of the most liberal voices when it comes to health insurance reforms.
While my people may not speak the same health care language or advocate the exact same solutions that many health care reform advocates or left-of-center folks would raise, the differences are largely just in the terminology used. For instance, my people are not going to mention Medicare for All or a public option as an answer to our country’s health care woes. Those phrases have been carefully tarred and feathered by the insurance industry as “socialism” to hold back both centrist and Republican voters and policymakers from putting guardrails in place that would cut into the industry’s immense profits. But again, it’s the terminologies that have been discredited – not the sentiment behind them.
On more than one occasion, when talking with my people about health insurers, they have straight-up volunteered that they think “insurance companies should be outlawed.” That belief, last time I checked, was to the left of even Senators Elizabeth Warren and Bernie Sander’s proposals to finally establish universal coverage for every American by expanding Medicare to cover all of us.
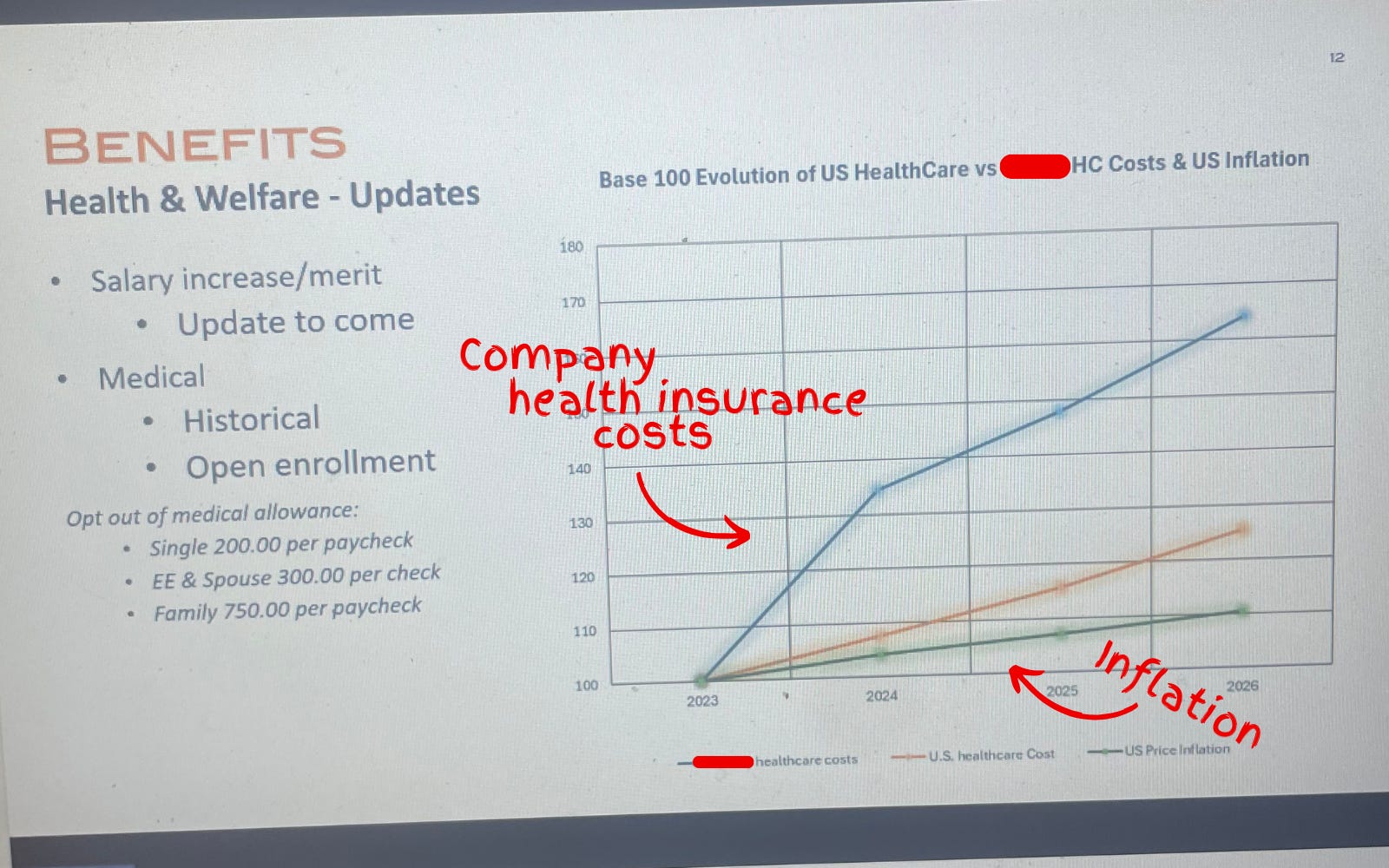
Another one of my people, who handles financials for the North American-sector of a sizable global company in the home-technology space, FaceTimed me last week to show me his computer screen while he was crunching the companies’ health care costs.
Photograph of a slide used during the company town hall showing the company’s health care costs vastly outpacing the rate of inflation.
In anticipation for a company-wide town hall, he had to make a slide showing that the health insurance costs for his company’s U.S.-side had increased (on average) 20% over the past several years – including a projected 25% jump in 2026. He couldn’t believe it. “Show this to Wendell,” he said.
And that’s the thing:
Nobody can believe how out-of-control Big Insurance has become.
Where my people and I meet
It’s fair to say that I think more about health care policy than the average bear. And it’s true that my people have had me in their ear talking about these issues for nearly a decade. But as I noted above, polling shows that while certain solutions may not be as popular, the desire for action is clear and exists sans my yapping.
Over years of conversations, there have been some major themes that have stuck. I will list them below:
Big Insurance is the villain in health care: With its army of slick lobbyists and spokesmen on TV, Big Insurance is the epitome of the D.C.-swamp monster that so many Americans disdain. Between 2014 and 2024, just seven for-profit health insurers amassed $543.4 billion in profits (of which they spent $618 million on lobbying during that time) all while 100 million Americans owe $220 billion in medical debt and Americans’ life expectancy is ranked 48th in the world.
Big Insurance and it’s cushy government handouts: Nearly all of Big Insurance’s growth has come from contracts it engineers with the federal and state governments in the form of managing Medicaid, Medicare Advantage and some Veteran health services. These contracts are not the invisible hand of the free market but rather cushy government handouts that have allowed just seven for-profit health insurance conglomerates to capture $10.192 trillion in revenues between 2014 and 2024.
Big Insurance has grown too big: Big Insurance companies are buying up the entire health care landscape – from physician practices to pharmacies. That is why independent physicians are an endangered species and why an independent pharmacy closes nearly every day in this country.
Big Insurance hurts the little guy: American small businesses often see double-digit yearly increases in health insurance costs that stifle Main Street America’s growth and stop Americans from being entrepreneurs altogether. And, not to mention, if businesses weren’t being raked over the coals for more premium dollars year after year, more money could be paid to workers.
I included this list because I think we are at a watershed moment in the health care debate and reforming Big Insurance is no longer a wedge issue. It’s a bridge issue.
I don’t know what comes next
Because the long standoff between Republicans and Democrats to open the government finally came to an end this month – without the ACA subsidy extensions – Big Insurance reform (and health care reform broadly) has become an unaddressed priority in American politics.
In the current moment, if Republican electeds were smart, they’d read the writing on the wall and focus on rooting out an actual source of widespread waste, fraud and abuse found in health insurance companies’ private Medicare Advantage, Medicaid and military businesses. That’s an issue that polls incredibly well with conservatives. Just tackling Medicare Advantage, for example, could save taxpayers somewhere between $80 and $140 billion annually.For reference, the DOGE website claims it has only clawed back $214 billion in total since January.
Republicans could also work with their political opposites (and fulfill a campaign promise) to pass a worthwhile health insurance reform package that builds on (or possibly replace) the consumer protections of ACA and fills the loopholes of well-intended rules that have been exploited and manipulated by Big Insurance.
And it wouldn’t be a one-party trick. For what it’s worth, I think most Democrats in Washington would be on board with anything that lessens the corporate grip Big Insurance has on our country’s public programs and improves the ACA. In the last year, we’ve already seen Democrats link with the country’s current controlling party to introduce bills that would bring meaningful change to Big Insurance:
Senators Elizabeth Warren (D-MA) and Josh Hawley (R-MO) introduced legislation that would stop health insurance companies from owning pharmacy benefit managers (PBMs);
Senators Jeff Merkley (D-OR) and Bill Cassidy, M.D. (R-LA) introduced the No UPCODE Act to curb taxpayer-sponsored overpayments to health insurers; and
These unlikely partnerships in Washington are happening because what my people (and all people) want is a health insurance system that guarantees comprehensive coverage for all of us, without forcing folks to choose between biopsies or groceries. Everybody I know – left, right and in between – wants a health care system that doesn’t bury families under mountains of medical bills or force them to attend unnecessary funerals. And all rational people want an insurance system that doesn’t buy off its buddies in Washington to serve their Wall Street daddies.
I want to scream from the mountaintops that health insurance reform is not just a moral or economic issue. It’s a winning issue.
Americans have had it. Most of Washington seems motivated. And now is the time for health care, patient and consumer advocates to change their tune and stop (just) preaching to the choir. Advocates for reform need to get their message to the corners of the country that they may have written off — or found too difficult to bridge — because the ground for health care reform is fertilefor change. And I think all people are ready.
Thanksgiving is in a few days. And in times of heightened political polarization, the dinner table – filled with folks sharing a myriad of different opinions – can become a battleground between courses of mashed potatoes and pumpkin pie. But if I can gleam anything from what I see as a bi-partisan kumbaya against Big Insurance, it’s that even with all the reported divisiveness, we have one less thing to argue about.
And because of that – I don’t know what comes next – but what I do know is that the 2026 midterms and the 2028 presidential election will be about health insurance reform. And whichever political party takes that seriously is going to seize the day.
Harvard psychologists Daniel Simons and Christopher Chabris ran a now-famous experiment in the late 1990s. They showed students a short video of six people passing basketballs and told them to count the number of passes made by the three players in white.
Halfway through the film, a person in a gorilla suit walks into the frame, beats its chest and exits. Amazingly, half of viewers — both then and in multiple recreations of the study — never notice the gorilla. They’re so focused on counting passes that they miss the obvious event happening right in front of them.
The authors call this “inattentional blindness.” And you don’t need to visit a research lab to see it. It’s everywhere in American healthcare.
Policymakers, business leaders and medical societies are all busy counting their own pass equivalents: metrics like insurance subsidies, premiums and enrollment numbers.
As a country, we need to stop counting passes long enough to observe how the gorilla negatively affects people everywhere: in Washington, in boardrooms, in workplaces and in rural communities. Only then can we confront the gorilla head on.
1. The gorilla in Washington
In Congress, lawmakers spent 43 days debating how to reopen the government. The fight centered on whether to continue funding the enhanced premium tax credits that have made coverage more affordable for roughly 20 million lower-income Americans who purchase health insurance through the Affordable Care Act’s online exchanges.
Democrats argued that ending those payments in 2026 would cause premiums to spike and make care unaffordable. Republicans warned that continuing them would add nearly $400 billion to the federal deficit over the next decade. Both believed they were protecting Americans from financial harm. And both were right. If the cost of providing medical care isn’t reduced, neither the federal government nor the average family will be able to afford it.
The United States spends $14,885 per person each year on medical care while the next highest-paying nation, Switzerland, spends $9,963 per person with far better clinical outcomes, according to the Peterson Center, .
If the U.S. could cut the spending gap between American and Swiss healthcare in half, our nation would save $700 billion annually. Those savings could help maintain ACA subsidies, lower out-of-pocket costs for families and reduce federal deficits.
But the gorilla inflicts financial damage far beyond just the ACA exchanges. Between federal funding cuts and eligibility changes, analysts warn that millions of Americans enrolled in Medicaid will become uninsured starting in 2026. Meanwhile, because federal law limits Medicare payment growth to the rate of inflation, hospitals make up lost revenue by charging private insurers and their enrollees more (already about 250% of Medicare rates). Ultimately, employers and workers will pay the price.
2. The gorilla in corporate America
America’s C-suite leaders are conducting the business equivalent of counting passes. Instead of confronting the cost of medical care itself, they’re focused on comparing premiums, raising deductibles and choosing plans with narrower physician networks.
But without major changes in how care is delivered, no plan will remain affordable.
The average cost of family health coverage premiums will approach $30,000 next year, with employers paying about $24,000 and workers responsible for the rest, according to an October KFF survey of 1,862 non-federal public and private firms. A projected 9% premium increase means employers and employees together will spend roughly $2,500 more next year per worker — limiting wage growth, hiring and investments in innovation.
America doesn’t have an insurance problem. It has a medical cost crisis.
3. The gorilla in the workplace
While workers focus on wages, benefits and job security, the same cost crisis threatening businesses and government is about to hit them hard.
More than half of U.S. adults receive health insurance through an employer. But as medical costs rise, companies are turning to automation and generative AI to reduce their expenses.
Amazon offers a vivid example: the company eliminated 14,000 office and professional roles and announced plans to combine robotics with generative AI to replace as many as three-quarters of its warehouse workforce. The company plans to create new, higher-skill jobs to maintain the robots, but far fewer (and not for the same people who were displaced).
When workers lose employer-based insurance, they don’t stop getting sick. They turn to Medicaid or subsidized exchange plans. That strains government budgets, lowers hospital reimbursements and pushes insurers to raise commercial premiums even higher.
Unless the cost of medical care drops dramatically, the gorilla’s impact will reverberate throughout society.
4. The gorilla in rural hospitals
The cost crisis is devastating people everywhere, but perhaps nowhere more than in rural America. Over the past two decades, 150 rural hospitals have closed or stopped offering inpatient services. Another 700 facilities (nearly one-third of those remaining) are at risk of shutting down.
With small patient populations and high fixed costs, many rural hospitals can no longer provide inpatient care. But instead of reducing the high cost of care delivery, most communities pursue short-term relief: emergency grants, temporary bailouts and added Congressional funding.
These efforts can delay closure, but they don’t change the math. Even when hospital beds are empty, the buildings must be staffed, heated, insured and maintained, turning every day into a financial loss.
To survive, the model will have to change, and painful sacrifices will be necessary.
Addressing the gorilla everywhere
The United States can dramatically reduce healthcare spending while improving quality. But doing so will require a structural overhaul, not incremental tweaks. Three major opportunities already exist.
1. Shrink our hospital footprint
America maintains far more hospitals than it needs, with many offering duplicate services at high fixed costs. A more sustainable system would:
Eliminate overlapping specialty programs in crowded markets.
Small rural hospitals could transition into 24-hour emergency and urgent-care hubs supported by telemedicine and reliable, low-cost transportation to larger facilities.
2. Prevent diseases before they happen
According to the CDC, more effective control of chronic diseases would reduce medical costs up to $1.8 trillion by preventing as many as half of all heart attacks, strokes, cancers and kidney failures. Three pragmatic opportunities include:
Every complication avoided is a hospital admission, ICU stay or surgery that never happens and is never billed.
Pay for value, not volume
Healthcare’s fee-for-service payment system rewards doing more, not doing better. Capitation — fixed monthly payments to physician groups and hospitals — flips the incentive structure, rewarding improved health, not just disease treatment.
Under capitation, prevention becomes financially rewarded, chronic diseases are managed earlier and more effectively, and care shifts to high-quality, cost-efficient settings, including outpatient facilities and virtual platforms.
The result is a virtuous cycle: healthier patients, fewer complications and significantly lower cost.
No single group — government, employers, patients or clinicians — can solve this crisis alone. Success will require all stakeholders to overcome their inattentional blindness and confront the gorilla together. The only question is how much worse things must become before we do.