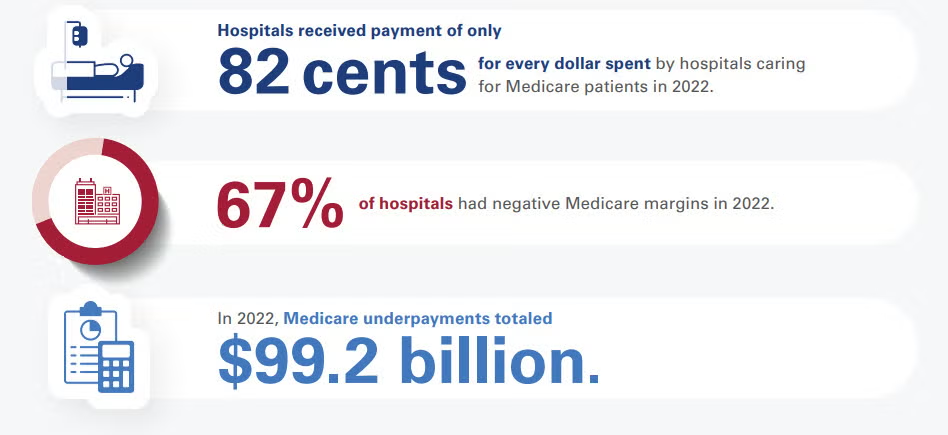
Medicare reimburses hospitals at an average of 82% to 87% of the actual cost of providing patient care. According to long-term data from the American Hospital Association (AHA) and the Congressional Budget Office (CBO), this means hospitals face a shortfall, receiving roughly 82 to 87 cents for every dollar they spend caring for Medicare beneficiaries.
Financial Impact and Hospital Margins
Because Medicare reimbursement rates are fixed by the federal government, they often fail to keep pace with the rising costs of labor, drugs, and supplies:
Negative Profit Margins: The Medicare Payment Advisory Commission (MedPAC) reported that hospitals experienced an average -12% margin on fee-for-service Medicare services, with projections remaining deeply negative at -10%. [1]
Widespread Losses: Approximately 67% of all U.S. hospitals operate at a net financial loss specifically on their Medicare patient population. [1]
Aggregate Underpayments: This payment-to-cost deficit translates to roughly $99.2 billion in annual underpayments that hospitals must absorb or offset through other revenue streams.
How Hospitals Balance the Deficit
To remain financially viable while absorbing underpayments from Medicare and Medicaid, hospitals rely on cost-shifting to the private sector:
Commercial Insurance Rates: Private, employer-sponsored health plans pay hospitals significantly more to subsidize public program shortfalls. On average, commercial insurers reimburse hospitals at 196% to 199% of Medicare rates.
Payer Mix Vulnerability: Hospitals located in regions with high concentrations of elderly or low-income residents are at higher financial risk. At 96% of U.S. hospitals, government programs (Medicare and Medicaid) account for more than half of all inpatient days.
If you are tracking hospital financials or healthcare policy, would you like to see how Medicaid reimbursement rates compare, or look closer at the differences between inpatient and outpatient Medicare payment structures?
Medicaid reimburses hospitals at an average of 88% to 90% of the actual cost of care, but this figure heavily relies on supplemental government funding. Without these extra state and federal payments, standard Medicaid base rates only cover roughly 58% to 65% of hospital costs.
Because Medicaid is jointly funded by federal and state governments, the exact payment-to-cost ratio varies wildly by state, fluctuating between 49% and 169% of Medicare benchmarks.
The Core Components of Medicaid Payments
Medicaid hospital payment structures are highly complex and divided into two primary tiers:
Base Rates (Severe Shortfalls): Standard Fee-For-Service (FFS) base rates and Managed Care Organization (MCO) plans pay well below actual expenditures. According to industry data published by the American Hospital Association (AHA), standard MCO plans cover just 65 cents on the dollar, while FFS base payments plummet to 58 cents on the dollar.
Supplemental Payments (The Lifeline): To minimize this gap, states issue extra payments to hospitals. These account for over 52% of total Medicaid hospital spending nationwide and are broken down into:
Disproportionate Share Hospital (DSH) Payments: Extra funds legally required for safety-net hospitals serving high volumes of low-income or uninsured patients.
Non-DSH Supplemental Payments: Upper Payment Limit (UPL) adjustments and state-directed payments meant to artificially boost base rates closer to commercial or Medicare levels.
Operational Impacts on Hospitals
The gap between Medicaid base reimbursement and actual cost strains hospital systems in several distinct ways:
Widespread Financial Loss: Even after accounting for all safety-net supplemental payments, roughly 62% of U.S. hospitals operate at a net loss on their Medicaid patient populations.
Aggregate Underfunding: The total nationwide Medicaid underpayment deficit adds up to approximately $24.8 billion annually that hospitals must absorb.
The Commercial Subsidy: Because public programs underpay, hospitals shift costs onto employer-sponsored health plans. As a result, private insurers are charged nearly double (up to 200%) what Medicare and Medicaid pay for the exact same medical services.
The administrations new ACA rules encourage health insurers to offer loans for medical bills instead of addressing the soaring out-of-pocket costs driving Americans into debt.
Most Americans are familiar with UnitedHealth, the largest private health insurer in America – if not because the corporate giant provides their medical coverage, then because of the massive publicity when the CEO of its key subsidiary was assassinated on a Manhattan street in December 2024.
The shooting of Brian Thompson also sparked a nationwide debate over Big Insurance practices, after many came forward with horror stories about their denied claims for urgent medical care or other bad health insurance experiences. Yet there is one thing most Americans do not know about UnitedHealth: It also has a bank.
But a number of physicians did know about Optum Financial by the spring of 2025, and they were not happy. Some doctors said their practices had been forced to borrow money from Optum to deal with a crippling cyberattack on the medical payments system, and Optum then pressured them to quickly repay the money. One New Jersey specialist in pediatric neurology and neurosurgery told The New York Times: “Optum, in my opinion, is acting like a loan shark trying to rapidly collect.”
Now, financially pressed U.S. families might learn what it’s like to owe money to Optum, under a new plan from the Trump administration.
With out-of-pocket medical costs for Americans skyrocketing, new guidelines for the Affordable Care Act marketplace suggest that insurers begin offering loans to patients with sky-high deductibles and unexpected large medical bills, a loan that presumably would be repaid with interest.
“We note that multiyear and 1-year catastrophic plans may be able to offer relief from the high deductible and maximum annual limitation on cost sharing through other mechanisms,” reads the final rule. “For example, issuers of catastrophic plans could consider financing the deductible by providing enrollees a loan.”
Experts say the ACA rules for 2027 and 2028 from the Centers for Medicare & Medicaid Services reveal the administration’s focus on expanding consumer choice and reducing federal outlays while ignoring the core issue: higher out-of-pocket costs.
“They’re putting a lot of stock into the idea that people really want these extremely, extremely high deductibles and out-of-pocket costs,” said Katie Keith, director of the Center for Health Policy and the Law at the Georgetown University Law Center. “And so they’re coming up with all these attempts at workarounds, including things like making your insurance company your bank.”
The New York Times noted that UnitedHealth, with its Optum financial unit, is the one large insurer that’s already equipped to offer loan packages to patients who can’t afford their bills. In addition to its controversial program of loans to physician practices, Optum’s bank currently offers government-approved Health Savings Accounts, or HSAs, which allow patients to set aside pre-tax earnings for future medical bills. A UnitedHealth spokesperson wouldn’t comment to the Times on the new ACA rules.
It’s understandable why the Big Insurance icon wouldn’t be eager to weigh in on a concept that will only fuel consumer anger over the increasing unaffordability of health care. U.S. Rep. Shontel Brown, an Ohio Democrat, weighed in on the Trump administration scheme on the social media platform X by noting this would “supercharge medical debt.” She added: “This could ruin people’s finances, while creating a financial incentive for insurers to deny coverage.”
Indeed, a 2025 report from the health-policy organization KFF found that UnitedHealth had – along with two Blue Cross Blue Shield affiliates – one of the nation’s three highest rates of claims denials for its ACA Marketplace policies. Its reported denial rate of 33% was nearly double the overall national rate of 19%. Now UnitedHealth – which posted more than $12 billion in profits in 2025, the highest of the nation’s insurers – could make even more money from denying claims or raising deductibles and offering loans.
The crisis of high out-of-pocket medical costs in America has been spiraling rapidly since the Trump administration and the Republican-controlled Congress rejected extending enhanced federal subsidies that had made coverage under the ACA, or Obamacare, reasonably affordable.
For millions of Americans, the end of those subsidies – with some consumers getting 2026 monthly premium bills that have more than doubled – has meant shifting to the lowest level of Bronze ACA plans, which come with high annual deductibles. This will mean thousands of dollars in bills for an unexpected major illness.
The soaring premiums have also seen many families joining the growing ranks of the uninsured. One early analysis from KFF predicted that as many as 5.5 million Americans – or about 25% of the peak enrollment – will have dropped their ACA insurance by the end of 2026, The new negative aura around health insurance – higher premiums, higher-out-of-pocket costs for those choosing inferior plans, or those without any coverage at all – is behind a recent report that about one-third of all Americans are cutting routine expenditures or even skipping meals to deal with their rising doctor bills and drug costs.
Instead of continuing the subsidies that had brought a steep rise in ACA enrollment earlier in the decade, the Republican-led government insists it is addressing the growing affordability crisis with new options that dangle lower premiums with the much greater risk of painful out-of-pocket costs in an emergency.
The government’s new ACA rules for 2027 increase the number of people who’d be eligible to buy so-called catastrophic plans that might defray costs for an extreme medical emergency but put consumers on the hook for the costs of most doctor visits or prescriptions. This is on top of new rules that will allow insurers to raise deductibles for the third-tier Bronze plans to $15,600 for individual coverage or $31,200 per family.
The Trump administration hoped to boost catastrophic plans to spike their enrollment as high as 3 million Americans, but Louise Norris, the longtime expert who writes for Healthinsurance.org, noted that a variety of factors have prevented any surge in customers for these high-deductible plans. In some states, she noted, premiums are actually lower for the Bronze plans, and this year, only about 67,000 people have signed up for the catastrophic plans.
Norris said the Trump administration’s idea for insurance-company loans is “that you can pay back that deductible over time, [but] I’m not sure that would really offset those other factors in terms of making those plans appealing.” She added that, “if you don’t qualify for subsidies, and you’re looking for the cheapest plan you can get in a lot of areas, that’s actually going to be a Bronze plan.”
So the government seems determined to make catastrophic insurance popular when American consumers don’t really want it.
Instead, the various schemes in the new ACA rules for 2027 and beyond – pitched with a notion of offering consumers more choices instead of the cost relief that Americans need – are projected to cost a whopping $1.3 billion annually, while it’s projected that two million more people will likely drop their ACA coverage because of the expense.
While the Trump administration and its GOP allies on Capitol Hill own this current crisis, Democrats need to acknowledge their own complicity in the situation.
Democrats in the past have bent to insurers’ demands to make sure all the health plans offered in the ACA marketplace have cost-sharing requirements of some amount and also to allow the out-of-pocket maximum to be unaffordably high for most Americans – especially for people with chronic conditions and those with low incomes.
This year’s midterm election is an opportunity for candidates to promise that health care affordability will be a priority. The centerpiece of such an agenda should be lowering the outrageous out–of-pocket maximums. The Lower Out of Pockets NOW coalition, which I founded, supports a bill sponsored by Massachusetts Democratic U.S. Rep. Jake Auchincloss to extend the Biden-era Medicare prescription drug yearly out-of-pocket maximum of $2,000 (rising to $2,100 this year) to people enrolled in ACA marketplace plans.
Some states already offer innovative cost-control plans. For example, Massachusetts now requires issuers of individual coverage and fully insured group coverage to limit increases in the enrollees’ out-of-pocket costs to the Consumer Price Index inflation rate for the Boston area. For 2027, the cap will be 3.6%. The covered expenses include plan deductibles, copayments and coinsurance bills.
When the idea of loans from insurers like UnitedHealth was reported in The New York Times, an attorney commented on social media that “it’s hard to top this level of dystopia.” This is a wake-up call to focus on the real pathways to affordable health care.
A federal watchdog is renewing the debate over whether private insurers are overutilizing prior authorization to delay patient careNew polling shows how the Trump administration’s approach to health policy could impact the midterm electionsDrugmakers are tweaking GLP-1 formulations, showing that industry still views the drug category as a revenue winner It’s a sweltering day in Washington, and yet Health Brief persists.
Medicare Advantage, operated by private insurance plans, has come under scrutiny. (Jenny Kane/AP)
The Lead Brief:
A new report from a federal watchdog found that three of the nation’s largest Medicare Advantage insurers routinely denied requests for post-acute care services, which could intensify scrutiny of prior authorization practices in the rapidly growing program.The Office of Inspector General for the Department of Health and Human Servicesexamined more than 2,000 prior authorization decisions made in June 2024 by Aetna, UnitedHealthcare and Humana.→ That’s the subject of the latest report from The Post’s Christopher Rowland.The OIG focused on services often needed after a hospital stay, including long-term acute care hospitals and inpatient rehabilitation facilities. Delays or denials can leave patients stuck in hospitals longer than necessary or without access to specialized recovery services.The report found denial rates for long-term acute care hospitals ranged from 70 percent to 80 percent, while denials for inpatient rehabilitation services exceeded 50 percent across all three insurers.
Why it matters:
More than half of Medicare beneficiaries — roughly 35 million people — are now enrolled in Medicare Advantage plans, giving a handful of insurers enormous influence over access to care.“As enrollment in Medicare Advantage continues to grow, so does the urgency and importance of ensuring that [insurance companies] are delivering on the value that the federal government pays them to provide,” the OIG report said.Complaints about Medicare Advantage coverage denials are nothing new, but the report underscores the potential impact they can have.The Centers for Medicare and Medicaid Services, which oversees the Medicare Advantage program,has been working with insurers over the last year to scale back their use of prior authorization.
What to watch:
The report could add fuel to several legislative proposals on Capitol Hill that would require insurers to submit more information about claim denial rates and, for Medicare Advantage plans specifically, additional encounter data related to patient care. The OIG report found for-profit Medicare Advantage organizations denied coverage more frequently than nonprofit plans, a pattern investigators said suggests financial incentives may play a role in utilization management decisions.→ But the report’s data predates pledges that private insurers have made to decrease use of the practice for all consumers. Companies have reported early progress in reducing prior authorization for many services.“This report reflects data from 2024. Since then, health plans have voluntarily eliminated roughly 6.5 million prior authorizations across markets — including more than 15 percent in Medicare Advantage,” said Mary Beth Donahue, president and CEO of the Better Medicare Alliance.Insurers also pointed to previous findings, including ones from the HHS watchdog in 2018, that raised concerns about whether many inpatient rehab facilities met Medicare’s standards or were providing unnecessary care that ultimately harmed patients.“The reports ignore serious, well-documented concerns about wide variations in the cost and quality of post-acute care and skilled nursing facilities,” said Chris Bond, a spokesperson for insurance industry group AHIP.BUT WAIT, THERE’S MORE→
A companion report issued by the OIG also renews scrutiny of insurers’ use of contractors to conduct prior authorization reviews. Investigators found a UnitedHealth Group subsidiary, formerly known as NaviHealth, denied nursing home care more frequently than insurers themselves or other vendors. The subsidiary, which rebranded to Home & Community Care in 2024, has allegedly used an algorithm to determine care needs. The OIG report doesn’t mention the reported algorithm usage. UnitedHealth Group has maintained that coverage decisions are always made by a human, thereby rejecting claims that the algorithms led to improperly denied care. However, the claims are at the center of an ongoing lawsuit filed by the families of deceased Medicare Advantage patients. The inspector general is urging CMS to take action to ensure plans are not improperly denying care. CMS officials told Christopher the agency is examining insurance denials by collecting data through a pilot program and conducting audits. The agency added that it “will continue using its full range of oversight and enforcement tools to identify potential issues, hold plans accountable and strengthen program integrity while protecting beneficiary access to care.
The Trump administration has announced that it will significantly expand access to so-called catastrophic health insurance plans, which are policies with comparatively low monthly premiums but deductibles so high they often leave families effectively uninsured until a medical crisis strikes. CMS described the move as giving Americans “flexibility” and improving access to “affordable healthcare coverage.” But what I call them are “junk plans”.
Back in October, I warned that these plans (often called short-term, limited-duration insurance plans, or STLDIs) were poised for a comeback as enhanced Affordable Care Act subsidies expired and millions of Americans faced sharp premium increases. Well, now these plans are, in fact, a reality.
The Affordable Care Act outlawed most of these junk-style plans because the law requires insurers to cover health care services people need, including prescription drugs, hospitalization, mental health care and maternity care. The ACA also forced insurers to spend most premium dollars on medical care instead of executive compensation, advertising and shareholder returns.
But the ACA never fully solved the deeper affordability crisis in American health care. Premiums have steadily become much too high. Deductibles and other out-of-pocket requirements have put care out of reach for millions as insurers have continued to shift more costs onto patients while simultaneously becoming larger, more powerful and more profitable. The shortcomings of the ACA and the decisions by the President and congressional Republicans have created the perfect opening for catastrophic plans to return.
Affordability’s all the buzz, but Trump’s sweeping payment rule emphasizes consumer choice over cost control.
When families are staring at monthly premiums they can no longer afford, a cheaper option — even one loaded with massive deductibles and coverage gaps — starts looking attractive. That is exactly what insurers are counting on.
In my old job at Cigna, I helped market plans like these. In my book Deadly Spin, I called them what they often really are: “the illusion of coverage.” These policies were designed to look like insurance while minimizing the likelihood insurers would actually have to pay significant claims. Companies like UnitedHealth Group and other insurance and health care conglomerates make enormous profits on catastrophic-style plans because the deductibles are so high and the restrictions so extensive that relatively few claims ever get paid.
Supporters of these plans frame them as “consumer choice.” But choice is a misleading word when many Americans are being financially cornered into skimpier coverage because comprehensive insurance has become unaffordable. People do not think they will get cancer before it happens. No one expects a devasting car crash or for their kid to come down with a confusing illness. The danger with junk plans is that people undoubtedly only discover how weak their coverage is after their lives have already been turned upside down.
And so, both parties in Washington deserve criticism. Republicans are now openly expanding access to catastrophic-style plans. But Democrats also bear responsibility for defending a post-ACA system that still leaves millions of Americans underinsured and financially exposed. Expanding coverage was enormously important. But coverage alone is not enough if using that coverage can still bankrupt you. We need a comprehensive update to the consumer protections in the ACA – expanding junk insurance is not that – and Republicans know better.
The real danger now is that America slowly normalizes a health care system where people are expected to carry insurance cards that offer little meaningful protection until disaster strikes. Once that becomes acceptable, legitimate insurance and junk insurance become indistinguishable.
Findings from the Commonwealth Fund 2025 Affordability Survey and Focus Groups.
U.S. adults with private insurance are anxious and frustrated about getting and paying for the care they need through their health plan. One of patients’ main concerns is uncertainty about whether their insurer will cover a health procedure or prescription drug that their doctor says they need, particularly for a serious medical condition.
Insurers can deny coverage for a variety of reasons. For example, they might deem a treatment or procedure to be medically unnecessary. Payment can also be denied for care delivered by an out-of-network provider, or for services the plan simply doesn’t cover. Administrative or billing errors can also trigger a denial.1
In this brief, we report findings from the Commonwealth Fund 2025 Affordability Survey on patients’ and families’ experiences with insurance coverage denials. We pair these findings with those from focus groups on the same topic. We examine experiences with two types of denials: those that occur before care is received, which we refer to as prior authorization denials, and those that occur after care has been provided, which we refer to as claim denials.
SSRS interviewed a nationally representative sample of 6,353 adults ages 19 to 64 from July 22 to October 27, 2025. Our analysis focused on 4,589 respondents with private insurance, either through an employer or the Affordable Care Act (ACA) marketplaces and individual insurance market. To gain a deeper understanding of people who experienced coverage denials, SSRS also conducted eight online focus groups with a total of 45 privately insured adults across the United States. To learn more about the survey and the focus groups, see “How We Conducted This Survey.”
Highlights
Experience with denials: One in five (21%) U.S. working-age adults with private insurance reported that they or a family member had experienced an insurance company denial of coverage for medical care recommended by a doctor in the past year, either before or after the care was provided.
Treatment delays: Forty-one percent of people who experienced a prior authorization denial said it led to a delay in medical care, and more than a quarter (28%) said a health problem got worse because of it. More than 60 percent said the denial caused worry and anxiety.
Out-of-pocket costs and medical debt: Among people who experienced a claim denial, nearly 70 percent said it cost them or their household more money. More than two in five (43%) adults who experienced a claim denial reported that the denial led to medical debt that they are still paying off.
Appeals: Only about half of those who experienced a denial appealed the decision, citing uncertainty over their right to do so and whether it would make a difference if they did, as well as confusion about who to contact.
We asked U.S. working-age adults with private insurance coverage if their insurance, or the insurance of a household member, denied coverage for recommended medical care. One in five (21%) working-age adults reported a coverage denial in the past year for a health care service recommended by a provider, either their own or that of a family member. Thirteen percent reported a prior authorization denial, 8 percent reported a claim denial, and 1 percent experienced both a prior authorization denial and a claim denial.
In focus groups with people who reported having a prior authorization or claim denial, participants reported that coverage denials, and the process of challenging them, often had significant consequences for their finances, health, and well-being.
Denied: John’s Story
John, who is in his early 60s, had surgery on both rotator cuffs. His provider recommended physical therapy (PT) as part of his recovery. For the first surgery, his PT was fully covered. After the second surgery one year later, his insurance company denied coverage for PT.
He plans to appeal the denial through his PT provider. “I’m going back to the physical therapist to ask them to resubmit my application, see if they can reword it and make a better case for me.”
Coverage denials can harm peoples’ health and financial well-being. Over half (63%) of working-age adults with private insurance who experienced a prior authorization denial of coverage for medical care said it caused them or their households worry or anxiety. About 40 percent said that a prior authorization denial delayed medical care, and more than a quarter (28%) said that their health problem worsened as a result. Three in 10 said they spent more money because of the prior authorization denial. That’s because when coverage is denied, some patients may elect to pay for their care out of pocket.
Denied: Sally’s Story
Sally, who is in her 40s, was due for a routine mammogram. Her gynecologist recommended that she also get an ultrasound, because she has dense breasts. Sally was told the ultrasound would be covered when she called prior to her appointment, but after she had the procedure, her insurance company refused to pay for it.
Sally says she’s still fighting the claim denial, but she’s feeling discouraged. She feels her insurance provider “will try to wiggle out of anything they can.”
Having a claim denied after receiving care leaves patients and their families on the hook for medical bills they didn’t expect. Nearly 70 percent of people who experienced a claim denial said that the denial cost them or their household more money. Thirty percent reported the denial had led to a delay in their health care, possibly because they were reluctant or financially unable to seek additional care. One in five people said their health problem worsened as a result.
For focus group participants, coverage denials were often a source of financial stress. Some patients who appealed their insurer’s denial said their health care provider had threatened to send their overdue bills to collections while they awaited their insurance company’s decision. They feared that their credit score would suffer if they continued waiting for an insurer’s decision.
I’m very busy right now. I haven’t pursued any avenue. I just paid for [the test]. I didn’t want to; I was afraid, and I haven’t learned much about credit, how it affects me, or whether it affects me. . . . I decided not to proceed with any legal means. I just paid it.
Oscar, a man in his 30s who had a claim denial for lab tests
Coverage denials also affected peoples’ subsequent medical care decisions. Some focus group participants said they were avoiding getting needed medical care because of their coverage denial. Following a coverage denial, one participant stopped seeking care for her ongoing health issue, which remains unresolved. Others are postponing future checkups or procedures because of how uncertain insurance coverage can be. Even just the anticipation of coverage denials and unexpected bills led some participants to avoid seeking care.
I feel like I’ve been unable to address the initial issue. . . . I don’t want to go back [to the doctor] with the very high chance [care] gets denied again.
Mary, a woman in her 20s who had a claim denial for lab tests
Coverage denials can have serious financial consequences. More than two in five (43%) adults who had a claim denial said the denial caused them or their household to incur medical debt that they are still paying off. More than half of the adults said that their original bill was $1,000 or more.
For many focus group participants, the accumulation of medical debt because of a coverage denial had made them hesitant to get health care again. Worry about financial consequences of additional care further exacerbated the anxiety and stress they experienced.
Denied: Jaime’s Story
Jaime was at dinner with his wife when he lost consciousness. She called an ambulance from the restaurant, and Jaime was taken to the hospital. Arriving barely conscious, he was told the hospital was out of his plan’s network.
“Because of the type of insurance I have, they just said they couldn’t accept me due to the coverage. . . . I had to wait hours for them to call back and forth between the hospital and the insurance company before they finally allowed the hospital to provide coverage for me.”
Jaime’s insurance covered some of his tests at the hospital but not all of them — for example, they covered a magnetic resonance imaging scan but not an electrocardiogram. He said he was convinced that “anything they could find not to pay, basically, they didn’t.” A few months later, Jaime’s insurance notified him that they also would not cover the $3,000 ambulance bill.
Jaime was left with significant medical debt. He makes monthly payments, so the debt doesn’t affect his credit. He worries, however, about future medical bills.
Even though patients have a right to appeal an insurer’s decision to deny coverage for a health care service, only about half appealed. When asked why they didn’t appeal a coverage denial, many people believed it would not make a difference. Many also doubted they had a right to appeal a decision or expressed confusion about who they were supposed to contact.
Patients in focus groups described a time-intensive, confusing, and highly frustrating process to appeal coverage denials. They often weren’t sure if they should contest the denial with their provider or insurance company, or even why they should have to appeal at all, since the denial was for care their doctor recommended.
[I] gave it my all in appealing the whole situation. . . . I got the run around like, ‘Oh, you need to speak to this person.’ Then they transferred me back to that person and the phone would ring and ring, and I’d give a voicemail and they wouldn’t call me back for two or three days. I’m still fighting with them.
Sally, a woman in her 40s with a claim denial for ultrasound
Several focus group participants felt that appealing a coverage denial would be futile. One thought that insurance companies take advantage of patients’ lack of knowledge about the health system. Many expressed frustration with the lack of transparency from insurers, saying patients “have no clue what’s going to be covered” when a doctor recommends health care. Over time, this pattern eroded participants’ trust in both their health care providers and insurance plans.
I hate the way it felt like I got conned. . . . I think [the insurance companies] know that the average person is not going to ask the right questions or know the right information. They take advantage of that, which I think is terrible, especially . . . those who are elderly or anything like that who don’t have the help or the resources.
About half of people challenged their coverage denials, but they were not always successful. Among those who challenged prior authorization denials, 30 percent said that their insurer approved the recommended medical care, and a quarter received approval for a different type of care. But in one-third of appealed cases, the insurer continued to deny the care. Nearly 80 percent of people who challenged their prior authorization denial and had received a decision on their appeal at the time of the survey said they waited two weeks or more for their insurance company’s decision.
Among patients and their families who challenged a claim denial, only one-third (33%) said their insurer reduced or eliminated the amount of money they owed. Thirty-six percent said their insurer denied their appeal, similar to the share of people who were unable to reverse their prior authorization denials. More than 60 percent of those who challenged their claim denial and had received a decision on their appeal at the time of the survey said that their insurer took one month or more to reach a decision.
Some focus group participants described a time-consuming and stressful process to appeal coverage denials. They often felt “caught in the middle” between their provider and insurance company as they tried to navigate a system that seemed designed to work against them.
[The insurance company] said, ‘You’ve had enough [physical therapy appointments].’ My physical therapist [says I need more], he’s still arguing for me, but they said no. . . . It’s almost like they will always give you an initial denial and see whether or not you’ll actually fight them on it.
John, who had a prior authorization denial for physical therapy following shoulder surgery
When asked who they held responsible for their coverage denial, nearly nine in 10 people blamed their insurance company. And many also blamed the health care system in general. Others viewed their providers as responsible for the denial, and more than one in five blamed the government for their experience.
In focus groups, some participants described how their ordeal with a coverage denial caused them to “totally lose trust” in their health care provider or insurance company, particularly when they had been explicitly told by at least one party that their care would be covered. Participants’ frustration with the health care system was palpable, and many remarked that insurance companies or the health system needed to change.
Denied: Nathan’s Story
Nathan didn’t anticipate a months-long fight with his insurance carrier while his wife battled cancer. Early in her treatment, the oncologist ordered genetic testing to look for mutations that would influence her response to therapies. Nathan and his wife were initially told that diagnostic genetic testing would be covered by their insurance, at least partially. But after the testing was completed, they were shocked to learn their insurance would not cover it.
Nathan began the frustrating process of contesting the denial. “You get in this loop of, holy cow, you ask eight people the same question. You get eight completely different answers.”
The couple eventually appealed to the oncologist, who submitted additional information to justify the necessity of the testing. While the insurance company elected to cover part of the testing, Nathan still couldn’t get a clear answer on his final bill amount.
What Can Government Do to Help Consumers?
Prior authorization can be a useful tool for protecting patients from low-value care that provides little benefit or might actually harm them. However, the processes insurers currently use lack clear rationales that patients and their providers can understand. Most troubling is that prior authorization is preventing patients from getting the care they need while placing additional burdens on physicians and their staff.
When asked what policymakers might do to help consumers, focus group participants said there should be greater transparency in insurer decision-making with “no ambiguity” in which procedures are covered. Some participants thought there should be external oversight by “another entity outside the insurers themselves” and said there must be clear reasons “why an insurance company is rejecting coverage, particularly when the test or procedure is ordered or recommended by a doctor.” There was also a desire for transparency to see where their premium dollars were going. Said one participant, “They are not using the money to pay for my care, and that is what frustrates me a lot.”
A Patchwork of Inadequate Laws and Regulations
The United States has a dated and patchwork system of regulations governing coverage denials and patients’ right to appeal them. Denial rules for employer plans have not been updated since 2000.2 In 2010, the ACA extended those rules to apply to all nongrandfathered individual and marketplace plans.3 While the Biden administration issued a new set of regulations on denials in 2024, these apply only to plans that fall under the jurisdiction of the Centers for Medicare and Medicaid Services (CMS), including marketplace plans in the 30 states that use the federal HealthCare.gov platform. They do not apply to employer plans or marketplace plans in states that run their own marketplaces.
Several states have passed laws that go further than federal requirements. States, however, lack jurisdiction over large, self-insured employers, which employ the majority of Americans.
In 2025, the largest U.S. health insurers announced a voluntary commitment to streamline prior authorization processes, including reducing the number of services subject to prior authorization and honoring preapprovals for a set period when people switch health plans.4
Clearly, there is a need to bring order to the fragmented set of laws governing coverage denials. Congress can accomplish this through standardization across all types of insurance and through the expansion and strengthening of rules regarding transparency in coverage decisions, oversight of insurers, and patients’ rights to appeal decisions. Options include:
Expanding the right to appeal. Consumers in nongrandfathered health plans, including employer plans, have the right to appeal coverage denials, and insurers are required to review and reconsider their decisions. If an insurer still denies coverage, patients have the right to an independent third-party review, and the insurer must accept the outcome of that review.
However, federal regulations restrict third-party appeals to denials based on medical necessity, which one study found made up just 5 percent of all denials.5 The majority of denials are for unspecified reasons, administrative issues, excluded services, and lack of referral or prior authorization.6 Consumers would be better served if all denials were eligible for external review.
Standardizing and streamlining prior authorization procedures in all health plans. The Biden administration issued a rule in 2024 seeking to increase transparency and standardization of prior authorization procedures for insurers selling plans in the 30 marketplaces that use HealthCare.gov, as well as those in other public programs.7 Beginning in January 2027, these payers must maintain a secure electronic portal with their list of covered items and services, documentation requirements for prior authorization, and a record of prior authorization requests and responses. CMS recently introduced a new proposed rule that would extend these requirements to prior authorization of prescription drugs.8
The federal government could expand both rules to cover all marketplace and employer plans. It also could require much greater transparency about insurer criteria for selecting services that need prior authorization.9
Learning from states’ approaches to prior authorization. At least 10 states have implemented a “gold card” approach for providers that reach a threshold level of prior authorization approvals. This enables providers to deliver certain services or prescribe drugs without seeking prior authorization.10 Several other states have shortened timelines for insurers to respond to prior authorization requests, required reviewers to meet clinical qualifications, or exempted or limited some services from prior authorization review, such as mental health care or care for chronic conditions. Although these state actions do not affect people in self-insured employer plans, they can inform federal policy.
Funding consumer assistance programs. The ACA authorized Consumer Assistance Program (CAP) grants to help states establish or strengthen services for patients to inform them of their rights and help them resolve health plan disputes. In the first year, CAP grants allowed states to recover more than $18 million for patients.11
Although federal funding for CAP grants has ended, the programs still exist in 31 states and the District of Columbia and continue to save consumers money (for example, Connecticut recovered $4.3 million for patients in 2021).12 Reinstating federal funding could help establish CAPs in the 20 states that currently don’t have them.
Reporting health care claim denials and appeals. The ACA requires all nongrandfathered health plans, including all employer plans, to report data on claim denials, the reasons for the denial, and the total number of denied and appealed claims.13 However, the federal government has limited enforcement to just marketplace plans sold through 30 marketplaces operated by the federal government. The Biden administration’s 2024 rule increases data reporting requirements for these plans, but patients may not be aware that this information is available on an insurer’s website.14 Expanding public reporting of these decisions to include all marketplace plans and employer plans — and making the data accessible and understandable to consumers on publicly accessible websites — would further the public’s understanding of insurer practices.
HOW WE CONDUCTED THIS SURVEY
The Commonwealth Fund 2025 Affordability Survey was administered by SSRS from July 22 to October 27, 2025. The survey consisted of telephone and online interviews in English and in Spanish and was conducted among a random, nationally representative sample of 6,353 adults ages 19 to 64 years living in the United States. The survey interviews were completed via a multiframe approach, which included address-based samples (ABS), prepaid cell phone samples, and the SSRS Opinion Panel. Interviews were conducted online or on the phone via ABS (n=1,794), via prepaid cell phones (n=328), and online via the SSRS Opinion Panel (n=4,231).
The sample was designed to exclude anyone age 65 and older, while also allowing for a sufficient sample of those anticipated to experience more health care affordability challenges (such as coverage denials, billing errors, or medical debt). Statistical results were weighted in stages to compensate for sample designs and patterns of nonresponse that might bias results. In the first stage of weighting, base weights were applied to account for sampling probabilities and were computed separately for each of the three sample frames. The base-weighted samples were combined using a compositing adjustment. Finally, the combined sample was calibrated to match target population benchmarks.
The resulting weighted sample is representative of the approximately 196 million U.S. adults ages 19 to 64. The survey’s margin of sampling error is +/– 1.5 percentage points at the 95 percent confidence level. The ABS portion of the survey achieved a 14.4 percent response rate, the prepaid cell portion achieved a 1.5 percent response rate, and the SSRS Opinion panel portion achieved a 2.5 percent response rate.
This brief focuses on 4,589 adults in the survey with private insurance. The resulting weighted sample is representative of approximately 130.6 million adults ages 19 to 64 with private insurance. The margin of sampling error for the subgroup of those with private insurance is +/– 1.7 percentage points at the 95 percent confidence level.
SSRS conducted eight online focus groups in April 2025, prior to fielding the survey. Six focus groups were in English, and two were in Spanish, with a total number of 45 participants. The focus groups informed the development of survey questions designed to capture people’s experience with coverage denials, billing errors, and medical debt. This brief highlights the experiences of the 27 participants who experienced coverage denials.
The loss of millions of ACA marketplace enrollees will likely force hospitals to confront a growing share of uncompensated care and rising bad debt.
KEY TAKEAWAYS
ACA marketplace enrollment is projected to fall by 21.5% this year after enhanced premium tax credits expired, with more consumers choosing lower-premium, higher-deductible plans.
Hospitals could face growing financial strain from underinsured patients who carry coverage but delay care or struggle to pay large out-of-pocket costs.
The coverage shifts may disrupt payer mix forecasting, value-based care strategies, and revenue cycle performance at a time when hospitals are already navigating elevated costs.
The expiration of enhanced Affordable Care Act (ACA) subsidies is expected to significantly impact the healthcare coverage landscape, and hospital leaders could feel the downstream effects soon.
Analysis from KFF projects ACA marketplace enrollment could fall by 21.5%, or nearly five million people this year, dropping from 22.3 million to about 17.5 million covered lives. At the same time, consumers who remain insured are opting for higher-deductible bronze plans as premiums climb.
For providers, the shift threatens to create more patients who carry insurance, but with deductibles so high that care is often delayed and collections become more difficult.
According to KFF, the average ACA marketplace deductible jumped 37% year-over-year, increasing from $2,759 in 2025 to $3,786 in 2026, marking the largest increase in marketplace history. Bronze plan enrollment climbed from 30% to 40% of all marketplace selections, while silver plan enrollment dropped from 57% to a record-low 43%.
The enrollment decline largely stems from the expiration of enhanced premium tax credits that had expanded affordability and helped drive marketplace enrollment to record highs over the last several years. KFF estimated that average monthly premium payments rose 58% from $113 to $178 after the subsidies expired.
That fluctuation in affordability could meaningfully change hospital utilization patterns.
Patients facing higher out-of-pocket exposure often postpone elective procedures or avoid preventive services altogether until their conditions worsen. For hospitals already contending with thin margins and persistent costs, a growing population of underinsured patients could create additional pressure on revenue cycles and charity care programs.
The impact could particularly be felt for hospitals serving middle-income populations that previously benefited from expanded subsidies. KFF found that individuals above 400% of the federal poverty level, or the “subsidy cliff” population, accounted for nearly half (48%) of the decline in marketplace plan selections despite representing just 7% of 2025 enrollment.
Hospitals in states that experienced rapid ACA marketplace growth during the enhanced-subsidy era may see the biggest disruption. KFF identified 41 states with enrollment drops, with the largest seen in North Carolina (22%), Ohio (20%), West Virginia (17%), and Indiana, Delaware, and Arizona (all 16%).
The trend could also affect strategic priorities for health system executives, particularly around population health management and value-based care models that depend on stable insurance coverage and consistent patient engagement.
If marketplace depletion continues through the rest of the year, especially as consumers fail to keep up with higher premium payments, hospitals may need to revisit forecasting models tied to payer mix, utilization, and uncompensated care.
KFF noted that effectuated enrollment, which measures consumers who pay their premiums and maintain coverage, could decline between 17% and 26% this year due to midyear attrition and unpaid premiums, based on estimates from Wakely Consulting Group.
As a result, hospitals may invest more in front-end financial screening or Medicaid enrollment assistance and community outreach efforts aimed at preserving coverage continuity.
The concern for hospital leaders is that the coverage shifts come at a time when many organizations are already operating with limited financial flexibility. While hospitals have shown signs of improved operational discipline, many organizations continue to struggle with elevated expenses. Kaufman Hall’s latest National Hospital Flash Report for March found that bad debt and charity per calendar day was up 18% year-over-year, partly offsetting financial progress.
At a House Ways and Means Committee hearing, lawmakers targeted pricing and market power while executives pointed to cost pressures and reimbursement gaps.
KEY TAKEAWAYS
House Ways and Means Committee members cast hospitals as central figures contributing to increased costs for patients.
CEOs from major health systems highlighted labor costs, Medicare Advantage delays, and uneven reimbursement.
Ongoing disconnect between lawmakers and hospital leaders continues to affect affordability policy and provider strategy.
A hearing before the House Ways and Means Committee brought hospital finances into focus as lawmakers questioned the drivers of healthcare spending and health system CEOs described the reality facing providers.
The discussion centered on pricing, profit margins, and consolidation, with members of Congress pressing for accountability, while CEOs of HCA Healthcare, CommonSpirit Health, New York-Presbyterian, and ECU Health pointed to cost pressures and reimbursement challenges impacting business decisions.
Though both sides agreed that rising costs remain a significant issue, the hearing illustrated a divide in how those costs are understood. That tension continues to influence both policy proposals and provider strategy as the debate over affordability moves forward.
Committee chairman Jason Smith, R-Mo., opened the hearing by comparing hospital profitability with major corporations and tying that performance to what patients pay for care.
“Hospitals with more than 100 beds have a higher profit margin than Delta Air Lines, Target, or Disney,” Smith said. “Turns out charging an arm and a leg for health care is more lucrative than the Happiest Place on Earth.”
Smith placed responsibility on the entire healthcare system and highlighted insurers, which also faced the committee in January, but stressed that hospitals must answer for their role.
“This committee isn’t interested in hearing about how the high prices your businesses charge are someone else’s fault,” Smith said. “The blame game didn’t work with insurers, and it won’t work today. Simply put, hospitals are charging an insane amount for care. Hospital prices have skyrocketed 300 percent in just over two decades – more than any other sector of our economy.”
That line of questioning reflects a growing focus in Washington on hospital pricing as a central factor in affordability, and a push to rein in price increases through policymaking.
During the hearing, lawmakers raised concerns about the impact of consolidation on negotiated rates, the role of large systems in shaping local markets, and the degree to which higher commercial prices ripple through employers and households.
Executives described a more complex financial picture that extends beyond headline margins.
Sam Hazen, CEO of HCA, acknowledged elements of the committee’s concerns while emphasizing that hospital reimbursement varies widely based on factors like patient mix and acuity.
“There are certain aspects of your discussion here that have merit,” Hazen said. “I think there’s also merit to the hospitals receiving a premium in certain circumstances, so we would be more than willing to work with you on that.”
Payment friction emerged as a recurring theme, particularly in relation to Medicare Advantage. Wright Lassiter III, CEO of CommonSpirit, pointed to delays and denials as a source of strain for large nonprofit systems.
“Medicare Advantage plans are the most challenging today,” he said. “We have $4.3 billion in unpaid Medicare Advantage claims, with nearly $1 billion of that being more than 150 days past due for care that CommonSpirit has delivered to patients and communities that you represent.”
The conversation also turned to consolidation and access in regional markets. Michael Waldrum, CEO of ECU Health, described consolidation as a response to shifting market dynamics rather than a strategy aimed at expanding pricing leverage.
“Consolidation in our market is not driven by preference, it is how we survive,” he said. “As some exit and others enter with profit-driven agendas, systems like ECU Health are left to serve as a safety-net. The result is reduced access, worsening outcomes and increasing costs.”
A statement submitted by the AHA for the hearing reiterated the current pressures facing hospitals, but noted an effort to reduce the cost of care by “improving efficiency, embracing innovative technologies and redesigning how services are delivered.”
The AHA called on insurers, purchasers, drug and supply manufacturers, and policymakers to work together with hospitals on four key areas of the healthcare system: improving the health of individuals and communities, advancing value through care transformation, reducing regulatory and administrative waste, and innovating to improve care quality and outcomes.
However, the gap between how lawmakers view hospital pricing and how health system leaders contend with rising costs and uneven reimbursement continues to limit alignment on policies aimed at improving affordability.
In part two of our conversation below, we discuss potential reforms and policy solutions and how to achieve them.
Miranda is a health policy professor at the University of Pittsburgh and was the Roosevelt Institute’s 2025 author-in-residence.
Stephen Nuñez: You wrote the book before HR1 (the “One Big Beautiful Bill Act,” or OBBBA) was passed. There are myriad ways this bill will make health care worse for people. Is there anything that you’re particularly focused on, given your research into the causes and consequences of this (quasi-)managed-care system we seem to have backed ourselves into?
Miranda Yaver: In addition to the broad coverage losses and increases in administrative burdens associated with enrolling and staying enrolled in health insurance, a couple of things happened. First, with the expiration of the enhanced premium tax credits, those with Affordable Care Act (ACA) marketplace insurance saw their premiums jump up dramatically. That means denials of coverage that do arise may be more harmful because people have less financial wiggle room with which to get creative with stopgap measures.
With both premium increases and new administrative complexity around eligibility verification, there’s also greater potential for patient churn among health insurers, which creates a setting that can lead to myopic coverage decisions from insurers who feel they can pass the buck rather than make up-front investments in patient health. For example, an insurer might deny coverage for a diabetic’s continuous glucose monitor with the expectation that by the time the patient faces costly complications from poorly managed glucose, they’ll be with another insurer.
I think whenever we’re introducing new fiscal pressures in the insurance market, we need to worry about private insurers turning to prior authorization as one way to make up some of that financial deficit.
Stephen: I was joking on social media the other day that if you ask an ordinary person about the American Medical Association (AMA), you’re likely to get positive comments (“doctors are the good guys!”), but if you ask a social scientist you might get a tirade or perhaps a hissing sound. The AMA has since the time of President Franklin D. Roosevelt worked to prevent the expansion of “socialized medicine” and has been a large lobbying barrier to several attempts over the decades to expand public insurance and push industry reform. And yet pre-authorization (and post-procedure coverage denial) undermines doctors’ autonomy and bandwidth in ways that seem to really irk them. Politics can make strange bedfellows, so I’m wondering if you see any fruitful avenues for collaboration with the AMA on this issue?
Miranda:I think that’s absolutely right, and in Coverage Denied, I certainly highlight both perspectives: In chapter one, I walk through the political origins of prior authorization and its entrenchment. It’s hard to talk about the origins of this managed-care tool without reflecting on the yearslong outcry over socialized medicine, but I also highlight the AMA’s more contemporary work around prior authorization and physician burden reduction, as well as broader issues of professional autonomy. The AMA’s physician surveys call attention to the sweeping impact (or at least, perceived impact) of prior authorization—from time and staffing demands to adverse effects on patients. The organization has also led the charge in advocacy and model legislation to do things like regulate the qualifications of reviewing physicians, promote transparency concerning prior authorization requirements, require more timely processing, and reduce the volume of prior authorizations. None of those issues address the broader philosophical objections to prior authorization—that is, that health coverage decisions are being made by companies with fiduciary responsibilities to shareholders rather than by treating physicians—but they do reduce the extent to which patients and their physicians are dealing with the constant headaches of these processes.
The AMA rightly frames these prior authorization headaches as sources of physician burden and burnout. Even if physicians might prefer to do away with prior authorization, and even though promoting transparency and timeliness won’t necessarily result in fewer denials, these reforms could take the guesswork, “black-box” feeling out of prescribing. In turn, physicians could more easily assess whether and when to move on to a plan B rather than endure the protracted delays common under the current system. Regulation of the qualifications of reviewing physicians could (at least on the margins) reduce the odds of erroneous denials that reflect lack of familiarity with more recent treatment protocols outside a doctor’s field of specialty, and which necessitate burdensome appeals to rectify. And even in this highly polarized and gridlocked political climate, some of these measures are passing at the state level with unanimous or near-unanimous support.
But this does not disrupt the reliance on prior authorization or confront the philosophical objections. A larger-scale intervention into this facet of the US health-care system would require more sweeping health reform from Congress than is feasible in the foreseeable future given *gesticulates wildly at the world.* Although the AMA continues to oppose single-payer, over the decades they have become more conciliatory toward issues of health coverage expansion and now support a public option. A public option would certainly move our health insurance system forward because private health insurers (which have been heavily reliant on prior authorization, delays, and denials) would have to compete with a government plan. Still, my money is very much on single-payer—which would extract the profit focus—for delivering the most relief for those in need of health care. But politics is complex and often much more a dynamic of incrementalism than waving a magic wand, and I’m a big believer in moving the needle where we can and when we can, even if the bigger philosophical issues of health insurance delivery will have to wait a few years.
My money is very much on single-payer—which would extract the profit focus—for delivering the most relief for those in need of health care.
Stephen: So we have path dependence, we have a health-care system that is for-profit and generates poor outcomes (for hospitals, doctors, patients, even insurance companies alike), we have a host of actors, and we have the complexities of federalism on top of that. Things feel pretty dire! What are some things we could do at the state and/or federal level to solve or at least mitigate the problems you detail in the book?
Miranda: One area where states have begun to take action is the role of AI, which health insurers are increasingly using to bulk-process claims and prior authorizations. California’s SB 1120, which went into effect this year, stipulates that when insurers’ AI programs recommend denials, they must be reviewed by physicians in the appropriate specialty. These technologies are advancing faster than regulatory oversight tools can keep up with, and unlike the relatively low-stakes penalty assessed when, say, a student uses AI for a paper and hallucinates a citation, when AI programs get health coverage decisions wrong, the consequences can be dire. And especially amid the ongoing litigation against Medicare Advantage plans’ use of AI to deny (with reversal rates of 80–90 percent), this could be a valuable shift.
When AI programs get health coverage decisions wrong, the consequences can be dire.
Some states are doing things that I’m not as fond of: Gold card laws, under which physicians who secure around 92 percent or more approval for their prior authorizations become exempt from these processes. It sounds good at face value, but it’s really replacing one form of physician burden with another because it’s assessed at the plan-service level, such that one might have a wallet full of gold cards to keep track of—a gold card for head CT scans with Aetna and abdominal CTs with Cigna, and so on. Texas’s law was so restrictive that just 3 percent of physicians qualified as “high performing” under its terms, so its impact has proven quite limited.
There are other options worth thinking about that are highly feasible and don’t require revisiting big philosophical questions about the US health care system. For example, plain-language rules in health insurance communication could help prevent patients from falling through the cracks due to complex and technical explanations of denials and appeal processes. The average American adult reads at around the 8th grade level, but most health insurance materials are written in at least the 10th grade level. Lower-income and lower-educational attainment patients and non-native English speakers are especially vulnerable in this system. This would also be relatively simple to administer and enforce. The Washington State Office of the Insurance Commissioner is a great model of guiding patients through appeal processes—from an accessible YouTube video to template appeal letters for different types of denials. Of course, this doesn’t address the propensity to deny in the first place, but it can mitigate the ensuing patient burden.
It would also be relatively feasible for states to limit prior authorization’s application to only domains of health care where there are at least relatively recent evidence bases of abuse or overprescribing. All too often, prior authorization is applied to areas of medicine where this overuse is not a documented concern. Lower lumbar spine MRIs are a commonly cited example of overprescribing, such that health insurers will often require a few weeks of physical therapy before being able to proceed with the scheduling of the MRI. That might not necessarily be an inappropriate use of prior authorization, whereas applying this process to a drug like PReP is far less logical, since it is life-saving and there is no evidence of abuse. States could, at the least, require insurers to justify the use of prior authorization for these types of procedures with data and evidence.
At the federal level, the House of Representatives approved by a voice vote the Improving Seniors’ Timely Access to Care Act in 2022, but despite bipartisan support, the legislation died in the Senate. This bill was centrally aimed at streamlining existing prior authorization requirements. It would require Medicare Advantage plans to deliver timelier decisions through electronic processes. This wouldn’t increase the odds of approval, but it would mitigate delays before either initiating appeal or moving on to a plan B.
In the background of all of these state efforts is the reality that state reforms cannot touch the majority of employer-sponsored health insurance plans. This quirk, which deviates from the federalism embedded into so many other areas of health policymaking and beyond, is due to the constraints of the Employee Retirement Income Security Act (ERISA). ERISA preempts state laws that “relate to” self-insured health plans, which cover most workers in employer-sponsored insurance. Because of the limits of what states can do to move the needle on equitable coverage, comprehensive health insurance reform really needs to happen at the federal level, which presents obvious challenges in the current political environment.
Because of the limits of what states can do to move the needle on equitable coverage, comprehensive health insurance reform really needs to happen at the federal level.
Stephen: Cost control/overutilization is a fundamental problem, even if the way the US “solves” for it is particularly awful. I can think of a variety of ways single-payer public health insurance helps: no insurance churn so no short-termism; deductibles, copays, and coverage are subject to a democratic process; and the government has monopsony power to negotiate down provider rates. And yet the fee-for-service conundrum and responses to it still exist in other countries with models closer to single-payer.
Are there any models or policies from the international context that you find promising, even if not politically feasible in the US right now? I’m thinking of things like New Zealand’s no-fault compensation system for medical injury, which means doctors don’t have to run tests simply to avoid lawsuits, or Pay-for-Performance/Value-Based Care models that could base payment on health-care outcomes and not just volume of services.
Miranda: My work is very US-centric, but I’ve grown increasingly interested in Switzerland.Even though traditional Medicare is immensely efficient, spending vastly less on overhead than do private insurers, Americans largely maintain the perception that the private sector is comparatively more efficient in policy delivery. That constrains our political choices (though this preference is becoming weaker over time, as more Americans are open to a government-run system). Given this underlying preference, are there ways that we can make private health insurance work? I think Switzerland shows that the answer is “yes, but.”
Even though traditional Medicare is immensely efficient, spending vastly less on overhead than do private insurers, Americans largely maintain the perception that the private sector is comparatively more efficient in policy delivery.
The Swiss health insurance system is actually more privatized than ours, and like our system, there’s a great deal of decentralization across localities. Where it diverges is its coupling of privatization with significant regulation as opposed to a broader embrace of free-market principles. The Swiss are legally required to be insured (though they have many options from which to choose), and on top of the standard but comprehensive insurance package, people can purchase supplemental private insurance to fill in any gaps or gain access to better hospital accommodations (e.g., a private room) or to see additional health-care providers. Consequently, nearly everyone in Switzerland is insured. In contrast with the relatively consolidated insurance market we have—with UnitedHealthcare, Cigna, CVS Health/Aetna, Elevance, Centene, Humana, and Kaiser Permanente dominating the markets, especially in certain regions—the Swiss have 56 insurers from which to choose. But the Swiss government exerts considerable regulatory oversight over both quality and prices.
So, you’ve got nearly universal coverage, market competition, regulation of pricing so as to mitigate exploitative charges to patients and the system writ large, and privatization. But all of these elements are in combination with enough regulation that you’d be unlikely to run into the insurance barriers that are such a dominant American experience and that make up the focus of my book.
The challenge, of course, is that to get this better coverage (which unsurprisingly produces better health outcomes), the Swiss both accept a higher tax rate than US politics tends to find palatable, and they accept the insurance mandate (whereas there was public consternation, driven by conservative political leaders, over the ACA’s individual mandate). To be sure, Americans’ attitudes could shift: We’ve certainly seen significant growth in support for the ACA, and the share of Americans who see it as the federal government’s responsibility to ensure health-care access has increased significantly over recent years. To the extent that these trends continue, that could facilitate a broader menu of health reform options.
But there are also some questions about scalability given that Switzerland has roughly the same population as New Jersey, is quite homogeneous, and invests more broadly into addressing social determinants of health. All too often in the US, we ignore those social determinants, which are truly in the driver’s seat of our health, while pouring money at health-care delivery. This leaves us with high health spending but a suboptimal return on investment. Switzerland can serve as some inspiration to right-size US reliance on private industry, though the extension may be difficult amid political preference for lower tax rates and deregulation.
Stephen: Is there anything else we haven’t discussed that you’d like to highlight?
Miranda:One elephant in the room amid discussions of health insurance barriers—their proliferation and their persistence—is why health insurers have been able to remain so largely unaccountable. At least part of this answer comes back to ERISA. To begin with, it preempts states’ efforts at comprehensive coverage reforms. This means that when political conditions aren’t well-suited to federal reforms, while we can often turn to the states to advance progress where they can, ERISA prevents comprehensive prior authorization reforms or the broader reduction of administrative burden in insurance. Further, it denies meaningful legal recourse to patients enrolled in self-insured health plans, which is about two-thirds of covered workers. Under ERISA, denied patients cannot obtain monetary damages (e.g., punitive damages, or damages for pain and suffering) and attorney’s fee recovery is left to the discretion of the judge. All that patients are entitled to receive is the benefit owed, which may be cold comfort to someone whose condition has worsened. And needless to say, less affluent patients will be risk-averse in taking legal action with this vulnerability to being left to cover their own legal costs.
The lack of meaningful remedies is where it becomes really clear that health care was an afterthought in ERISA, which was motivated by pension concerns. If your employer tries to screw you out of your pension, you can sue and get your pension back, but health conditions can change and make this enforcement apparatus ill-suited. Further, lawyers will likely be reluctant to take on cases that lack a monetary value. And if insurers know that patients are especially unlikely to sue insurers under these conditions, effective control over these entities can be harder to come by because wrongful denials are virtually costless. So, ERISA’s denial of meaningful remedies for wrongful coverage denials can not only be harmful to the patients when such denials arise, but insurers may have less incentive to exercise caution when deciding whether to cover costly care because they won’t face a meaningful penalty. In the worst case scenario for them, they eventually cover the treatment if the patient challenges the denial, which they rarely do. This design can thus increase the probability that insurance barriers arise in the first place. Congress tried to fix this problem in the late 1990s with the Patients’ Bill of Rights, but it didn’t come close to enactment. That bill is a critical issue for legislators to revisit. I’m currently writing another book that looks squarely at what accounts for the entrenchment of this feature of our health insurance system and the ways it disrupts equitable access to health care.
“There are more ways people can be denied by their health insurer than they realize.”
It’s not news to any of us that the US health insurance system needs massive change. The sheer scale of administrative and financial burden on patients and providers is untenable. I spoke with Miranda Yaver about her research on one underdiscussed aspect of the insurance maze: coverage denials.
Miranda is a health policy professor at the University of Pittsburgh and was the Roosevelt Institute’s 2025 author-in-residence. Her book Coverage Denied is out today, April 23, from Cambridge University Press.
Health insurance coverage denials and how they affect patients
Stephen Nuñez: In my own recent research on health-care policy, I detailed the consequences of our broken system for patients: medical debt, bankruptcy, and delayed or forgone treatments that often lead to worse health outcomes down the road. I focused on some of the better-known aspects of American health care, like underinsurance through high premiums, high deductibles, co-pays, and gaps in coverage (such as being between jobs).
In your new book, you focus on another aspect of the health-care system: denial of coverage among people who think they are insured against injury and illness. Could you explain the different ways this plays out?
Miranda Yaver: When we talk about problems like underinsurance in America, we’re typically referring to high out-of-pocket medical costs within the plan terms (such as high deductibles or high cost sharing). What I work to do in Coverage Denied is show that there’s this additional, less-discussed dimension of underinsurance: inadequate protection by health benefits in which one is enrolled, not due to plan terms, but rather due to insurer decision-making about what is actually medically necessary. Strikingly, there are more ways people can be denied by their health insurer than they realize.
Prior authorization, or required health insurer preapproval for prescribed care (typically costlier care, though it has certainly extended to lower and even low-cost care in recent years), is the realm of denials with which Americans are likely the most familiar. This is when your health-care provider wants you to get a CT scan, but you can’t proceed with scheduling until it gets cleared by your health insurer—and it might get denied. When people are denied prior authorization for health-care services, they face delays or denials of medical tests or treatments, potentially risking worsening health, unless they can afford to pay out of pocket (but health care in the United States is notably expensive, so that is rarely an option).
There are appeal processes in place that a patient denied prior authorization and their physician can pursue, though it can take time to submit additional information and receive a redetermination, and physicians might only be given hours to respond to a request to avoid a patient being denied again. This might mean that the patient cannot proceed with scheduling a diagnostic test. In the case of, say, a prescription medication, the patient may go unmedicated—potentially leading to worsening of symptoms —or be on a second-choice regimen to avoid an entire gap in care, pending the insurer processes that will take an unknown period of time to resolve. And if the patient’s conditions worsen, they may eventually require higher-level (and consequently, more expensive) medical care.
The irony here is that prior authorization is partly a measure aimed at cost containment, but if denials are ultimately delays that necessitate more pronounced medical intervention (whether receipt of medication in the emergency department, or even getting admitted), then this practice can undercut insurers’ underlying profit objectives.
People can also receive concurrent denials, which occur when the insurer decides during the course of a medical treatment that it will decline coverage for further care. The result of this mid-treatment decision can be treatment disruption, if not altogether discontinuation, that can undercut optimal health outcomes for the patient.
Retrospective denials occur when the insurer denies payment for health care that was already provided to the patient. While this does not leave the patient vulnerable to declining health with respect to that condition, it does raise the prospect that they will have to take on medical debt and potentially forgo other care so as to avoid risking accruing additional medical expenses. Additionally, though infrequently, one may be vulnerable to a retroactive denial, which occurs when an insurer retracts payment for a service that they already approved, leaving the patient themselves responsible for the payment (e.g., because the insurer determined that they should not have approved it previously). This can also render the patient vulnerable to assuming new medical debt that can be financially destabilizing and foregoing further health-care expenses. While this may be an appropriate error correction on the part of the health insurer, it can drive significant uncertainty and destabilization for the patient, who might not have continued to pursue the care if they had better information at the outset.
These types of claim denials (i.e., denials post-treatment) operate quite differently from prior authorization denials. The good news is that they shouldn’t result in a patient’s worsening condition per se (though anxiety about a denial of coverage for test A may lead to reluctance to pursue test B). The bad news is that this can contribute to the patient’s financial destabilization, potentially leading to medical debt that hurts their credit and thus broader economic opportunity. And of course, we know that medical debt is unevenly distributed across racial and socioeconomic groups, and health insurance barriers constitute another driver of those inequities.
Given that patients are often making these decisions with informational disadvantages—we don’t have a good sense of what care is in fact medically necessary, let alone the criteria with which our insurers are evaluating this—this multitude of ways that patients can be left both medically and financially vulnerable lays bare just why accessing health care in the US can be so anxiety-provoking (not to mention inequitable). And while analyses have shown that some providers do prescribe medical care that is of low or questionable value (in turn, running up quite a tab), all too often, the burden falls on patients, who get caught in between their prescribers and their insurers.
Stephen: What remedies are there for patients when denials happen, and do people even know about them or how to obtain them?
Miranda: As I mentioned, there are appeal processes in place, which insurers are legally required to provide patients with information about when they are issuing a notice of a denial. Some insurers are especially transparent about their process—UnitedHealthcare, for example, publishes online its detailed description of the three-layered standard appeal process and three-layered expedited appeal process. But there are a few things that can and often do get in the way of patients understanding and acting on this right, so that fewer than 1 percent of denied marketplace claims and less than 12 percent of Medicare Advantage (the privatized version of Medicare) prior authorization denials are appealed.
For starters, appeal explanations are already complicated processes that are often written in a way that is difficult for the average reader to understand. That means many people don’t even know what their rights even are. Additionally, people may underestimate the value of appealing. “I’m just one person going about their day. How could I possibly stand a chance going up against a health insurance giant?” And in fact, when I asked 1,340 people to guess how often health insurance appeals are won, most survey respondents thought patients win less than 20 percent of the time. In truth, it’s closer to a coin flip, with various estimates lying in the 40–60 percent range, and 52 percent of my survey respondents winning their appeals if they appealed. But if you think that this endeavor of appealing is likely to be fruitless, it makes sense that one wouldn’t exert the time and energy—the burden—of appealing.
I asked all of my survey respondents who were denied by their insurer but did not appeal why they chose not to do so. The two most common reasons were that (a) they didn’t realize they could appeal (often because the information was in fine print or not conveyed in plain language, or they saw the denial and got so discouraged that they didn’t read further) and (b) they didn’t think they stood a chance at winning (though many said that if they had known it was a coin flip, they’d have been more likely to appeal their own denial). Respondents also cited confusion about how to navigate the red tape of this insurance process. So, on the one hand, there’s a lot of evidence that coverage denials are not only destabilizing to health and finances, but that administrative burden gets in the way of patients pursuing appeals to reverse these adverse decisions. On the other hand, my findings point to the possibility of some simple information interventions to improve patient knowledge and, in turn, improve access to health benefits, even if we can’t tackle (yet) the complexity of the appeal processes themselves.
But the underlying reality is that insurers expect that patients are unlikely to go through the appeal process, which is difficult enough on a good day (and we’re rarely having our best day when we need to appeal to insurers). In fact, one person I interviewed, who reviews claims for a major health insurer, said they were told that denying is perfectly fine because there is an appeal process—even though they have the data to confirm that most patients don’t go through with them. This is why I characterize these processes not as rationing care through denial, but rather rationing by inconvenience, or accumulations of inconveniences.
Stephen: This sort of thing seems even crueler than high premiums and deductibles, where at least you know what you’re (not) getting. The uncertainty and arbitrary and almost Kafkaesque conditions experienced by patients who suddenly find themselves without the safety net they thought they had purchased is really striking.
You did a lot of interviews for this book. Are there any cases that stand out to you, that really illustrate the absurdity of it all?
Miranda: It is absolutely the case that this uncertainty and apparent arbitrariness—the “song and dance”—is overwhelming and heart-wrenching for patients (as well as for their providers) in a way that goes beyond the broader but more predictable frustrations about care being unattainable due to, for example, a high-deductible health plan. One physician interviewee told me about his experience with prior authorization burdens:
“It feels like there are people sitting around a room conspiring to figure out how to delay care further. And every day that they can delay your care is money kept in their pocket longer.”
One patient story that stuck out was surely an administrative error, but nevertheless burdensome for both patient and physician to correct. This patient was getting a wrist MRI with contrast: First, the patient had radioactive dye injected, and then the scan was to be performed. Her insurer approved the radioactive injection but not the scan that made that exposure necessary. Now, at face value, that sounds silly—and it is. But what it took to correct it was a recognition that this was absurd (when a lot of patients don’t read itemized medical bills, let alone understand them), and a degree of health insurance literacy and administrative capital that enabled her to successfully navigate the complexity of the health insurance appeal process.
But there were some really heart-wrenching stories. One was from a low-income woman in the South who had taken time away from a years-long nursing career due to medical complications following the birth of her daughter. Amid prolonged severe lower abdominal pain and vaginal bleeding, she was ordered a CT scan and spent months navigating insurance complexity to get prior authorization, to no avail. When the insurer asked for additional documentation of medical necessity, she brought to bear all of her skills as a nurse, using not only technical medical terminology to document her symptoms but indicating numeric pain ratings based on exacerbating factors, ameliorating factors, and the like—things that the average individual can’t do, because most people have limited medical knowledge. “I’m a nurse. I know how to document stuff. I’ve been doing it for 15 years,” she recounted. But it was to no avail that she described her condition as clinically and as elaborately as possible when seeking insurer approval. “I got specific, they denied it, and they picked a different reason.”
Then, the hospital erroneously said that the prior authorization was approved, but this patient ended up stuck with such a big bill that not only did she have to put off necessary home repairs amid a failing roof, but she even contemplated divorcing her husband and the father of her daughter in order to have an income that would qualify for Medicaid. This level of financial and family devastation wasn’t anomalous.The average American can’t accommodate an emergency $1,000 expense without going into debt, and as most people can attest to, it’s not hard to accrue a $1,000 medical expense.
And alongside all of this was a real loss of trust in the system and feeling of inadequacy amid the navigation of red tape. One diabetic lawyer said of his battle to get a continuous glucose monitor,
“Is there something wrong with me? Do I not deserve this? Do I think my need is more important than it really is? The process makes you feel so small.”
Diabetes treatment was an area in which coverage barriers were very common. After one interviewee battled her insurer to get on a more sustainable insulin regimen, she said,
“It colored the way I interacted with insurance for the rest of my life.”
Relatedly, it was striking to see the prevalence of prior authorization requirements in corners of health-care delivery where there is not evidence of overutilization and abuse, the mitigation of which is ostensibly a central goal underlying the administration of prior authorization. PrEP is one such medication, which is critical in preventing HIV transmission and thus an important aspect of LGBTQ health. This isn’t a medication that people just take “for fun,” nor is it a medication that is abused or overprescribed—but there can be prior authorization attached to it nevertheless. Another example is insulin, which is literally lifesaving for millions of Americans, but can still have onerous prior authorization and formulary restrictions attached to it. As I spoke with these patients who felt like they were constantly playing the role of Sisyphus pushing the boulder up the hill, it is little wonder why they lost trust in, and felt betrayed by, the insurers to whom they had been paying monthly premiums for years.
How we got here: Why US health insurance is the way it is
Stephen:It seems that there’s a fundamental issue in health care around constraining costs and preventing overtreatment in the form of unnecessary/low-value/wasteful care. Doctors want to be thorough (and don’t want to be sued for malpractice), patients don’t know how to distinguish between necessary and unnecessary care, and insurers don’t want to pay, for example, to run an endless battery of useless tests. But while this might be a fundamental problem in health care, the ways in which it plays out in the United States are unique and tied to our for-profit insurance system.
Can you describe some of the features of our system that have contributed to “managed care” (plans that cut costs via pre-authorizations, drug tiers, step therapy, etc.)?
Miranda: During the New Deal, there was some hope that amid this expansion of national power to lift the US out of the Great Depression, there might be sufficient support to carry national health insurance across the finish line. But even Franklin D. Roosevelt’s immense popularity wasn’t enough to get this done, and it became clear pretty quickly that trying to tie health insurance to Social Security was going to compromise both, and Social Security was an absolute must-have. Harry Truman then spent his presidency fighting tirelessly, albeit unsuccessfully, for national health insurance, but faced immense opposition campaigns from organizations like the American Medical Association (AMA), which used the slogan “The Voluntary Way is the American Way” in an effort to curb movement toward a compulsory insurance program that they likened to “socialized medicine.” In the background of all of this, employer-sponsored insurance had just gained prominence during World War II and further advanced through the labor movement: The Stabilization Act of 1942 precluded raising wages to attract much-needed workers, so health insurance became the perk of choice.
Eisenhower didn’t unravel the New Deal, but he did favor privatization over national insurance. When the 1960s rolled around, the previous ambitions of national health insurance were scaled down to prioritize targeting two vulnerable populations, the indigent (who would get Medicaid) and the elderly (who would get Medicare). Amendments to the Social Security Act in 1965 ultimately secured this new coverage. And in fact, LBJ signed these into law at the Harry S. Truman Presidential Library in Independence, Missouri, as a nod to his long-fought efforts toward this expansion.
But of course, these programs cost money, in part thanks to the fee-for-service arrangements according to which they were designed, such that there was little oversight over billing and the physicians could earn more by ordering more tests and treatments. So, it’s around this time that we see the introduction of some very narrowly circumscribed utilization management, such as certifying hospital lengths of stay. Of course, having a physician tell an insurer, “Yes, this patient does still need to be in the hospital to treat X” is a far cry from its current sweep. But the rising health-care costs also fueled the enactment of the Health Maintenance Organization (HMO) Act of 1973, which encouraged the development of HMOs, which are private insurance plans. What would later follow was the more flexible preferred provider organizations (PPOs). Ironically, with this latter, more flexible mechanism of health insurance delivery came the loss of a key cost-control mechanism, giving rise to the set of concerns that led to the proliferation of prior authorization.
The Balanced Budget Act of 1997 further cemented the United States’ reliance on privatization, bringing Medicare Advantage onto the scene and escalating the privatization of Medicaid. It’s in this moment that we see at a large scale the privatization of traditionally public health insurance programs whose enrollees would now come to experience managed care plans’ cost-containment tools like prior authorization. And as health-care innovation—from new drugs to new technologies—flourished in the US, both quality and cost increased, spreading prior authorization into new corners of health-care delivery. Today, if you’re being prescribed a higher-cost drug, high-tech imaging, a surgery, a major procedure, and even some less costly drugs, you can bet on prior authorization or some form of step therapy (in which a patient must try lower-cost drugs before “stepping up” to what was initially prescribed).
At the end of the day, it’s a tough issue of politics, economics, medicine, and law all wrapped up in one. We don’t have unlimited amounts of money to spend on health care without making very hard (and likely politically unpalatable) choices in other areas of policy delivery, so we need to find ways to contain costs, hopefully without compromising quality of care. We often misperceive more care as equating to better care (sometimes it is, but it certainly isn’t a guarantee), which then places demands on physicians who need to be mindful of patient satisfaction ratings as well as malpractice liability. That can in turn drive some degree of defensive medicine (or ordering unnecessary tests and procedures) that comes with a price tag.
And in the background of all of this is the reality that health insurers don’t have a ton of incentive to make up-front investments in our health—even those that have a good return on investment—because people change health insurers so frequently. This means that while it may seem like poor financial planning for Cigna to deny a patient Drug A, by the time a costly complication manifests for the patient, they may no longer be on Cigna, but rather UnitedHealthcare, or they may have aged onto Medicare. So, in addition to concerns about privatization, cost containment (as well as profit maximization given the need to report quarterly growth), and overutilization (which can undercut those cost-containment objectives), there’s also some passing of the buck that may not yield great patient outcomes and may even drive up costs in the system writ large, but not for the insurer that issued the initial denial.
So, then we get to the question of whether there are better alternatives to contain costs. One way to make up the deficit is that insurers could raise premiums, but we know that’s untenable for most people and would drive problems of adverse selection. Negotiating down the cost of health-care delivery by providers would certainly be a nonstarter with the AMA as well as with the broader physician community, especially given the high cost of medical training and recent politics around loan forgiveness. Improving drug price negotiation with the pharmaceutical industry is important, and we’ve moved in that direction narrowly, but that still won’t touch a lot of the problems here.
Another very underdiscussed aspect of this problem is the reality that while overutilization is a commonly cited concern driving the implementation of prior authorization, physician burdens associated with prior authorization and the appeals it can necessitate can actually drive issues of underprescribing to avoid these challenges.
Stephen: A big theme of the book is path dependence, the idea that each legal or regulatory decision sets us down a path and makes it harder to reach other outcomes. For example, I was struck by the fact that the backlash against narrow networks implemented by HMO plans probably made pre-authorization more common.
Maybe a bigger surprise was the ways that the Affordable Care Act (ACA) may have inadvertently contributed to the current situation. Could you explain more?
Miranda: I’ll preface this by saying that I’m a huge fan of the ACA, but a few aspects of it are relevant to the story I’m telling here. First, it directly built on the private health insurance framework (the setting in which delays and denials of coverage are the most common) and left prior authorization largely undisturbed, with the exemption of emergency department care and in-network OB-GYN care. So, overall, there’s increased patient participation in private health insurance plans, which come with more prior authorization except in some narrowly circumscribed areas. But there’s also the possibility that when Congress told these private health insurers to cover all these people they’d done a very good job of finding ways to avoid covering—those with what had been declinable preexisting medical conditions (around 27 percent of non-elderly US adults, according to a 2019 KFF estimate)—the insurers look for other ways to curb costs. They can’t deny patients anymore, so it’s possible that denial of payment for prescribed care became the attractive alternative.
Stephen: When doing research on medical debt, I found that the debt problem was a lot worse for people on employer-sponsored insurance plans or ACA marketplace plans than for folks on Medicaid and Medicare (though a substantial portion of Medicare recipients are still carrying debt from their time uninsured and underinsured prior to aging into Medicare.)
You quote health-care expert Jacob Hacker in the book, who said, “Medicare should be the model for health security.” But a large part of the book details how both Medicaid and Medicare are also increasingly becoming managed-care systems. Can you explain what is happening and why?
Miranda: The US health insurance system is definitely made far more complex through its fragmentation, as well as its entwining of public and private programs, which can culminate in contradictory popular sentiment like “keep your government hands off my Medicare” and what Suzanne Mettler has characterized as the “submerged state.” And of course, Medicare is not the only government insurance program that has become heavily privatized. Not only are about 54 percent of seniors in Medicare Advantage, but about three-quarters of Medicaid is privatized.
Privatization of these two critical health insurance programs, which combine to cover roughly 4 in 10 Americans, is problematic for many reasons, but in the context of this book, it means adding a lot of prior authorization—and the delays and denials that come with it—for a population that has generally lower health-insurance literacy and is consequently less well-equipped to navigate the burdensome repercussions of these processes. Unlike Medicare Advantage, where 99 percent of enrollees have prior authorization, traditional Medicare has historically used prior authorization sparingly and denies care infrequently, though Centers for Medicare and Medicaid administrator Mehmet Oz’s introduction of the WISeR model that experts agree may lead to more denials. Medicare has been a game changer in enabling seniors to have quality coverage at a time in their lives when they generally have greater health needs but limited disposable income—and it provides this coverage with low administrative spending relative to private insurance and outside the confines of means-testing that can be stigmatizing and thus dampen policy take-up. But its privatization over the last three decades has produced outcomes that look a lot more like the broader private health insurance landscape (whether employer-sponsored insurance or the ACA marketplace) in terms of prior authorization, delays and denials of coverage, and burdensome and inequitable processes to appeal those adverse decisions.
On the managed Medicaid side, we also see frequent reliance on prior authorization and high incidence of delays and denials. Not only is this a population that has generally low health insurance literacy (raising the burdens of appealing barriers to coverage), but it is also generally less healthy (raising the stakes of these barriers to coverage). Moreover, due to their low income, they’re especially unlikely to be able to front the cost of medical treatment in order to avoid a gap in care pending an insurance appeal.
Blaming hospitals isn’t wrong. But it’s incomplete—and it’s exactly the story insurers want told.
Zack Cooper argued this week in The New York Times that Americans may be blaming the wrong culprit for rising premiums. In his view, the bigger driver is hospital market power—fueled by years of consolidation that policymakers have done little to stop. On that point, he’s on solid ground saying that hospital prices have climbed steadily, and oversight has lagged.
Where the argument falls short is in how it portrays insurers. It suggests they are largely on the defensive—unable to push back on powerful hospital systems and left to rely on tools like prior authorization and claim denials as a workaround. In that telling, insurers come across less as drivers of the problem and more as constrained players navigating a difficult market.
That’s not consistent with what I saw working inside the industry, or with how the business is structured to operate.
Cooper’s academic work on hospital consolidation is serious and worth engaging with. But the argument he made in the Times—whether intended or not—tracks closely with a line the insurance industry has advanced for years. It’s a familiar frame, and one I recognize because I helped design it.
The industry’s oldest trick
When I was head of corporate communications at Cigna, one of my core job responsibilities was to ensure that the public and policymakers understood what we called the “true drivers” of medical inflation. Those drivers were never us. They were hospitals charging too much, drug companies gouging patients, and — when we needed a villain closer to home — ordinary Americans overusing the health care system. The finger-pointing was deliberate, coordinated, and effective. As any magician will tell you, misdirection is the oldest trick in the book.
AHIP, the industry’s trade and lobbying group, is running that same playbook today with the full force of the industry behind it. In recent months it has blanketed Washington with the message that “hospital costs account for more than 40 cents of every premium dollar” and that hospitals should “stop looking around for someone else to blame.” This is not an inaccurate claim. It is an incomplete one, deployed with the precision of a public relations campaign rather than the rigor of a policy argument. The fact that Cooper’s op-ed reinforces that message — even from an independent and credentialed source — is a gift to an industry that has been under unprecedented scrutiny since the murder of a UnitedHealthcare CEO in late 2024.
I am not suggesting Cooper wrote his piece on AHIP’s behalf. I am suggesting that a structurally incomplete argument, published in arguably the country’s most influential newspaper at this precise moment, serves the insurance industry’s interests whether or not that was anyone’s intention.
Who started the consolidation arms race?
Cooper’s framing also elides a crucial piece of history. Hospital consolidation did not happen in a vacuum. Hospitals began merging in significant part as a defensive response to the growing bargaining power of large insurers. Providers seeking to consolidate often cited a desire to acquire bargaining leverage with market-dominant payers, arguing that their own consolidation could counter the consolidation of increasingly powerful insurers.
Insurer consolidation begat hospital consolidation, which begat higher prices, which begat higher premiums. It is an arms race in which the only losers are patients and employers.
In the third episode of the HEALTH CARE un-covered Show, we take a deep dive into prior authorization’s toll — from doctors to federal policy — featuring Dr. Wendy Dean, Dr. Seth Glickman and Rep. Suzan DelBene (D-WA) on CMS’s new AI-driven WISeR model.
Cooper is right that hospital market power is now the dominant force driving costs. But the insurers that consolidated first — and that benefited by squeezing providers in the short run — helped create the conditions for the hospital consolidation wave that followed. Neither side’s hands are clean. The arms race, which dates back to the rapid horizontal consolidation that occurred in the insurance industry in the 1990s and early 2000s, is what patients are now paying for.
Now to the incentive problem Cooper’s framing obscures. In commercial insurance — particularly the self-funded arrangements that now cover most large employers — the insurer often earns fees tied to the total size of claims processed. Higher hospital prices mean larger claims. Larger claims can mean higher revenue for the insurer administering the plan. This is not a conspiracy. It is arithmetic. The incentive to hold the line on hospital prices is weaker than Cooper suggests because in many arrangements, higher costs flow through to the insurer’s bottom line.
The Affordable Care Act’s medical loss ratio rules were supposed to fix this by requiring insurers to spend 80% to 85% of premiums on care. What those rules actually do, in a rising-cost environment, is allow absolute profits to grow even as the percentage stays fixed. If the pie gets bigger, the insurer’s slice gets bigger too — even at the same ratio.
The network access trap
In markets where a single hospital system controls the majority of beds, the insurer faces a problem that has nothing to do with negotiating skill. It cannot exclude that hospital from its network and still have a product to sell. Employers and individuals will not buy a plan that locks them out of the dominant regional provider. The hospital knows this. The insurer knows this. What gets called “negotiation” in these markets is often closer to ratification.
The insurer’s response to this trap — when it cannot win at the hospital price table — is not to fight harder. It is to redirect. Costs that cannot be controlled at the source get shifted somewhere more manageable: onto patients, through higher deductibles and narrower benefits; onto providers, through prior authorization burdens and claims denials; onto employers, through premium increases framed as the inevitable result of “medical trend.”
This is the point Cooper comes closest to and doesn’t quite reach. He writes that insurers “are incentivized to lower health spending, but in many markets don’t have the ability to put meaningful pressure on hospital prices.” That’s true. What is also true is that they put pressure on everything else, which all too often has the effect of reducing access to medically necessary care.
Prior authorization, step therapy, utilization management — these are not crude approximations of cost control. They are the rational corporate adaptation to a problem the insurer has decided not to solve at its source. They extract value from the system by making care harder to access rather than cheaper to provide. And they do so in a way that is largely invisible to the public as a cost-shifting mechanism, because each individual denial looks like a clinical decision rather than a financial one.