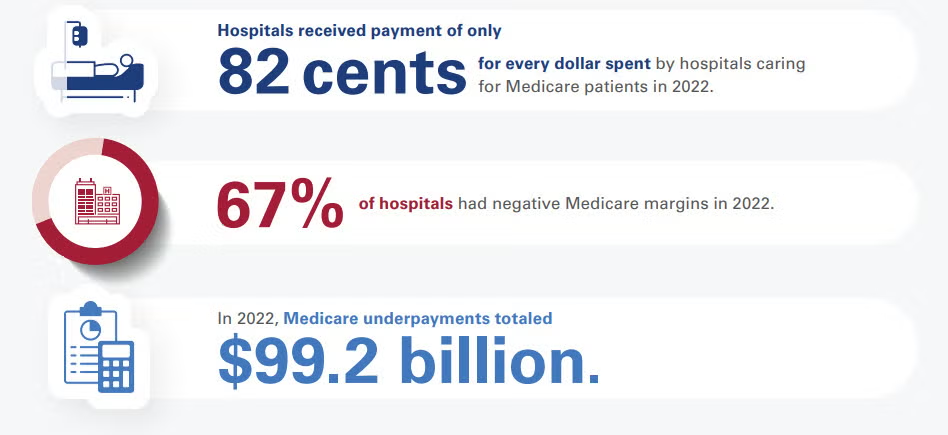
Medicare reimburses hospitals at an average of 82% to 87% of the actual cost of providing patient care. According to long-term data from the American Hospital Association (AHA) and the Congressional Budget Office (CBO), this means hospitals face a shortfall, receiving roughly 82 to 87 cents for every dollar they spend caring for Medicare beneficiaries.
Financial Impact and Hospital Margins
Because Medicare reimbursement rates are fixed by the federal government, they often fail to keep pace with the rising costs of labor, drugs, and supplies:
Negative Profit Margins: The Medicare Payment Advisory Commission (MedPAC) reported that hospitals experienced an average -12% margin on fee-for-service Medicare services, with projections remaining deeply negative at -10%. [1]
Widespread Losses: Approximately 67% of all U.S. hospitals operate at a net financial loss specifically on their Medicare patient population. [1]
Aggregate Underpayments: This payment-to-cost deficit translates to roughly $99.2 billion in annual underpayments that hospitals must absorb or offset through other revenue streams.
How Hospitals Balance the Deficit
To remain financially viable while absorbing underpayments from Medicare and Medicaid, hospitals rely on cost-shifting to the private sector:
Commercial Insurance Rates: Private, employer-sponsored health plans pay hospitals significantly more to subsidize public program shortfalls. On average, commercial insurers reimburse hospitals at 196% to 199% of Medicare rates.
Payer Mix Vulnerability: Hospitals located in regions with high concentrations of elderly or low-income residents are at higher financial risk. At 96% of U.S. hospitals, government programs (Medicare and Medicaid) account for more than half of all inpatient days.
If you are tracking hospital financials or healthcare policy, would you like to see how Medicaid reimbursement rates compare, or look closer at the differences between inpatient and outpatient Medicare payment structures?
Medicaid reimburses hospitals at an average of 88% to 90% of the actual cost of care, but this figure heavily relies on supplemental government funding. Without these extra state and federal payments, standard Medicaid base rates only cover roughly 58% to 65% of hospital costs.
Because Medicaid is jointly funded by federal and state governments, the exact payment-to-cost ratio varies wildly by state, fluctuating between 49% and 169% of Medicare benchmarks.
The Core Components of Medicaid Payments
Medicaid hospital payment structures are highly complex and divided into two primary tiers:
Base Rates (Severe Shortfalls): Standard Fee-For-Service (FFS) base rates and Managed Care Organization (MCO) plans pay well below actual expenditures. According to industry data published by the American Hospital Association (AHA), standard MCO plans cover just 65 cents on the dollar, while FFS base payments plummet to 58 cents on the dollar.
Supplemental Payments (The Lifeline): To minimize this gap, states issue extra payments to hospitals. These account for over 52% of total Medicaid hospital spending nationwide and are broken down into:
Disproportionate Share Hospital (DSH) Payments: Extra funds legally required for safety-net hospitals serving high volumes of low-income or uninsured patients.
Non-DSH Supplemental Payments: Upper Payment Limit (UPL) adjustments and state-directed payments meant to artificially boost base rates closer to commercial or Medicare levels.
Operational Impacts on Hospitals
The gap between Medicaid base reimbursement and actual cost strains hospital systems in several distinct ways:
Widespread Financial Loss: Even after accounting for all safety-net supplemental payments, roughly 62% of U.S. hospitals operate at a net loss on their Medicaid patient populations.
Aggregate Underfunding: The total nationwide Medicaid underpayment deficit adds up to approximately $24.8 billion annually that hospitals must absorb.
The Commercial Subsidy: Because public programs underpay, hospitals shift costs onto employer-sponsored health plans. As a result, private insurers are charged nearly double (up to 200%) what Medicare and Medicaid pay for the exact same medical services.
Minnesota lawmakers approved a $205 million funding package to stabilize Hennepin Healthcare, but it underscores that the safety-net risk is escalating. Here’s what Hennepin told us.
KEY TAKEAWAYS
Hennepin’s financial struggles highlight how hospitals with heavy Medicaid and uninsured populations remain vulnerable when reimbursement growth lags expense inflation.
CFOs should model scenarios involving Medicaid funding reductions, rising uncompensated care, and sustained labor-cost pressures to assess liquidity and capital needs.
While government funding can provide short-term relief, finance leaders should focus on long-term sustainability through revenue diversification, service-line optimization, and proactive advocacy efforts.
Hennepin Healthcare’s financial crisis has become one of the most closely watched healthcare stories in the country. Now bolstered with state funding, its story illustrates the mounting pressure on safety-net hospitals.
The CFO Take Away
Think of this headline as an underscore to the growing vulnerability of health systems whose payer mix is concentrated in government programs. Hennepin Healthcare’s situation demonstrates that even large, clinically essential institutions can find themselves in liquidity crises when reimbursement growth consistently trails expense inflation.
CFOs should view this as a warning to stress-test their organizations against scenarios involving Medicaid funding reductions, higher uncompensated-care volumes, and continued labor-cost pressure. The strategy lesson here is that traditional margin-improvement initiatives alone may not be enough. CFOs should be strengthening advocacy efforts, diversifying revenue streams where possible, reassessing service-line profitability, and building long-range capital plans that assume greater reimbursement volatility.
The market is tightening, and the broader takeaway is that safety-net economics are becoming a board-level risk issue. Organizations that wait until cash reserves deteriorate before pursuing structural solutions will find themselves relying on emergency legislative interventions rather than executing deliberate financial strategy.
The System
Hennepin Healthcare leaders have warned lawmakers that the organization faces severe financial challenges driven by a combination of factors: rising labor and operating costs, inadequate reimbursement from government programs, and a heavily Medicaid-dependent population.
The system has already tried to shrink costs by reducing beds and eliminating services, while seeking additional state support to stabilize operations. But policymakers ultimately negotiated a funding package worth approximately $205 million to help preserve the organization’s role as Minnesota’s largest trauma center and a critical provider for vulnerable and low-income populations.
In an email to me, the system stated:
“Hennepin Healthcare is deeply grateful to the lawmakers who acted with urgency and collaboration, and to our employees, patients, and advocates whose voices brought needed attention to this crisis. The stabilization funding does not resolve the long-term impacts of HR1 or the structural deficits that uniquely challenge safety-net hospital systems. But it does accomplish two essential things: it delivers historic support that sustains us, and it gives us the time and stability to work with the state on durable, long-term solutions.
Our immediate priorities are to stabilize our team and invest in patient care while carefully stewarding the funds allocated to us. We have essential needs that have been deferred because of financial challenges, including staffing, equipment, and other investments that support patient care.
Looking ahead, our strategy is focused on both operational improvement and long-term sustainability. We will continue working with state leaders, the Governor-appointed task force, and our future professional governing board to identify lasting solutions that strengthen Minnesota’s healthcare safety net and ensure Hennepin Healthcare can continue serving patients for generations to come.”
It’s clear the system views the package only as a bridge. It’s obviously not a solution. But beyond that, it’s also clear that this is not a Minnesota-confined story.
Hennepin Healthcare showcases the financial fragility of safety-net hospitals nationwide. In 2023, well before any of today’s Medicaid chaos, safety-net hospitals provided roughly $11 billion in uncompensated care.
Roughly three-quarters of Hennepin Healthcare’s patients are uninsured or covered by public insurance programs, creating a structural gap between the cost of care and reimbursement levels.
Hennepin Healthcare was projecting up to $50 million in operating losses for 2026 and a staggering $1.7 billion in deficits over the next decade. The organization’s repeated losses and dependence on government intervention underscore the challenges many urban safety-net systems face as Medicaid funding uncertainty, amongst other pressures, converge.
New National Health Expenditure projections show sustained cost growth outpacing GDP, driven by Medicare expansion, rising drug spend, and persistent utilization pressures.
KEY TAKEAWAYS
Medicare is projected to grow faster than other payers, increasing exposure to lower reimbursement rates and tightening system-wide margins.
Utilization is driving costs. Post-pandemic service use remains elevated, undermining the assumptions that demand would normalize.
Rapid pharmaceutical growth and shifting federal pricing policy make pharmacy costs unpredictable and scenario-dependent.
The latest National Health Expenditure projections from Health Affairs and CMS confirm what CFOs already suspect: cost growth is structural. Total U.S. health spending is expected to grow at roughly 5.4% annually through 2034, consistently outpacing GDP growth of about 4.1%, pushing healthcare’s share of the economy from roughly 18% today to more than 20% by 2034.
The first major implication is funding-source imbalance. Medicare is projected to grow the fastest at roughly 7.7% annually, driven by demographics and utilization intensity. Medicaid and commercial insurance trail at about 5% each, but still above general inflation. This divergence matters. Payer mix will steadily tilt toward government payers with structurally lower reimbursement growth. Even small shifts in payer composition will exacerbate pressure on operating margins unless productivity gains or rate improvements offset them.
Secondly, utilization is what’s really driving the next wave of cost growth. Recent data show elevated service use across hospital, physician, and pharmaceutical categories, with little evidence that post-pandemic demand has normalized. That suggests budgeting cycles can no longer assume regression to pre-2020 utilization trends. For CFOs, this complicates volume forecasting: demand is becoming less predictable and more sensitive to coverage expansion and policy-driven enrollment changes.
Third, prescription drug spending is now the fastest-growing category, with retail pharmaceuticals set to outpace hospital and physician services through the projection window. The combination of specialty drug uptake and policy-driven price reforms creates a dual volatility problem: higher baseline spend alongside uncertain future savings from federal negotiations and benefit redesigns. CFOs in both provider and payer organizations should treat pharmacy cost projections as scenario-driven, not point estimates.
Fourth, federal policy is increasingly the dominant driver of revenue exposure. The federal government’s share of total health spending is expected to rise from roughly 31% to 33% by 2034, reinforcing dependence on Medicare and federal Medicaid financing. At the same time, policy volatility—particularly around subsidies, eligibility rules, and drug pricing—introduces new forecasting risk that cannot be diversified away. CFOs should expect more frequent mid-cycle reimbursement adjustments and greater lag between policy adoption and financial realization.
Fifth, the insured population is expected to slightly decline as a share of total population over the next decade. This is a subtle but important signal for providers, because even small coverage shifts can disproportionately affect elective volume, bad debt exposure, and charity care assumptions. CFOs should incorporate coverage elasticity into long-range planning models, especially in markets with high exchange enrollment sensitivity.
Finally, healthcare is steadily absorbing a larger share of the U.S. GDP. Look out for structural revenue tailwinds for the sector and intensifying political and payer pressure to contain costs. CFOs should expect sustained scrutiny on operating efficiency, administrative overhead, and price justification across all service lines.
Ultimately, the shift here is from static 10-year budgeting to dynamic scenario planning. Health systems that quickly model policy sensitivity, payer mix drift, and utilization volatility in real time will be better positioned than those relying on historical cost curves that just no longer hold up.
The administrations new ACA rules encourage health insurers to offer loans for medical bills instead of addressing the soaring out-of-pocket costs driving Americans into debt.
Most Americans are familiar with UnitedHealth, the largest private health insurer in America – if not because the corporate giant provides their medical coverage, then because of the massive publicity when the CEO of its key subsidiary was assassinated on a Manhattan street in December 2024.
The shooting of Brian Thompson also sparked a nationwide debate over Big Insurance practices, after many came forward with horror stories about their denied claims for urgent medical care or other bad health insurance experiences. Yet there is one thing most Americans do not know about UnitedHealth: It also has a bank.
But a number of physicians did know about Optum Financial by the spring of 2025, and they were not happy. Some doctors said their practices had been forced to borrow money from Optum to deal with a crippling cyberattack on the medical payments system, and Optum then pressured them to quickly repay the money. One New Jersey specialist in pediatric neurology and neurosurgery told The New York Times: “Optum, in my opinion, is acting like a loan shark trying to rapidly collect.”
Now, financially pressed U.S. families might learn what it’s like to owe money to Optum, under a new plan from the Trump administration.
With out-of-pocket medical costs for Americans skyrocketing, new guidelines for the Affordable Care Act marketplace suggest that insurers begin offering loans to patients with sky-high deductibles and unexpected large medical bills, a loan that presumably would be repaid with interest.
“We note that multiyear and 1-year catastrophic plans may be able to offer relief from the high deductible and maximum annual limitation on cost sharing through other mechanisms,” reads the final rule. “For example, issuers of catastrophic plans could consider financing the deductible by providing enrollees a loan.”
Experts say the ACA rules for 2027 and 2028 from the Centers for Medicare & Medicaid Services reveal the administration’s focus on expanding consumer choice and reducing federal outlays while ignoring the core issue: higher out-of-pocket costs.
“They’re putting a lot of stock into the idea that people really want these extremely, extremely high deductibles and out-of-pocket costs,” said Katie Keith, director of the Center for Health Policy and the Law at the Georgetown University Law Center. “And so they’re coming up with all these attempts at workarounds, including things like making your insurance company your bank.”
The New York Times noted that UnitedHealth, with its Optum financial unit, is the one large insurer that’s already equipped to offer loan packages to patients who can’t afford their bills. In addition to its controversial program of loans to physician practices, Optum’s bank currently offers government-approved Health Savings Accounts, or HSAs, which allow patients to set aside pre-tax earnings for future medical bills. A UnitedHealth spokesperson wouldn’t comment to the Times on the new ACA rules.
It’s understandable why the Big Insurance icon wouldn’t be eager to weigh in on a concept that will only fuel consumer anger over the increasing unaffordability of health care. U.S. Rep. Shontel Brown, an Ohio Democrat, weighed in on the Trump administration scheme on the social media platform X by noting this would “supercharge medical debt.” She added: “This could ruin people’s finances, while creating a financial incentive for insurers to deny coverage.”
Indeed, a 2025 report from the health-policy organization KFF found that UnitedHealth had – along with two Blue Cross Blue Shield affiliates – one of the nation’s three highest rates of claims denials for its ACA Marketplace policies. Its reported denial rate of 33% was nearly double the overall national rate of 19%. Now UnitedHealth – which posted more than $12 billion in profits in 2025, the highest of the nation’s insurers – could make even more money from denying claims or raising deductibles and offering loans.
The crisis of high out-of-pocket medical costs in America has been spiraling rapidly since the Trump administration and the Republican-controlled Congress rejected extending enhanced federal subsidies that had made coverage under the ACA, or Obamacare, reasonably affordable.
For millions of Americans, the end of those subsidies – with some consumers getting 2026 monthly premium bills that have more than doubled – has meant shifting to the lowest level of Bronze ACA plans, which come with high annual deductibles. This will mean thousands of dollars in bills for an unexpected major illness.
The soaring premiums have also seen many families joining the growing ranks of the uninsured. One early analysis from KFF predicted that as many as 5.5 million Americans – or about 25% of the peak enrollment – will have dropped their ACA insurance by the end of 2026, The new negative aura around health insurance – higher premiums, higher-out-of-pocket costs for those choosing inferior plans, or those without any coverage at all – is behind a recent report that about one-third of all Americans are cutting routine expenditures or even skipping meals to deal with their rising doctor bills and drug costs.
Instead of continuing the subsidies that had brought a steep rise in ACA enrollment earlier in the decade, the Republican-led government insists it is addressing the growing affordability crisis with new options that dangle lower premiums with the much greater risk of painful out-of-pocket costs in an emergency.
The government’s new ACA rules for 2027 increase the number of people who’d be eligible to buy so-called catastrophic plans that might defray costs for an extreme medical emergency but put consumers on the hook for the costs of most doctor visits or prescriptions. This is on top of new rules that will allow insurers to raise deductibles for the third-tier Bronze plans to $15,600 for individual coverage or $31,200 per family.
The Trump administration hoped to boost catastrophic plans to spike their enrollment as high as 3 million Americans, but Louise Norris, the longtime expert who writes for Healthinsurance.org, noted that a variety of factors have prevented any surge in customers for these high-deductible plans. In some states, she noted, premiums are actually lower for the Bronze plans, and this year, only about 67,000 people have signed up for the catastrophic plans.
Norris said the Trump administration’s idea for insurance-company loans is “that you can pay back that deductible over time, [but] I’m not sure that would really offset those other factors in terms of making those plans appealing.” She added that, “if you don’t qualify for subsidies, and you’re looking for the cheapest plan you can get in a lot of areas, that’s actually going to be a Bronze plan.”
So the government seems determined to make catastrophic insurance popular when American consumers don’t really want it.
Instead, the various schemes in the new ACA rules for 2027 and beyond – pitched with a notion of offering consumers more choices instead of the cost relief that Americans need – are projected to cost a whopping $1.3 billion annually, while it’s projected that two million more people will likely drop their ACA coverage because of the expense.
While the Trump administration and its GOP allies on Capitol Hill own this current crisis, Democrats need to acknowledge their own complicity in the situation.
Democrats in the past have bent to insurers’ demands to make sure all the health plans offered in the ACA marketplace have cost-sharing requirements of some amount and also to allow the out-of-pocket maximum to be unaffordably high for most Americans – especially for people with chronic conditions and those with low incomes.
This year’s midterm election is an opportunity for candidates to promise that health care affordability will be a priority. The centerpiece of such an agenda should be lowering the outrageous out–of-pocket maximums. The Lower Out of Pockets NOW coalition, which I founded, supports a bill sponsored by Massachusetts Democratic U.S. Rep. Jake Auchincloss to extend the Biden-era Medicare prescription drug yearly out-of-pocket maximum of $2,000 (rising to $2,100 this year) to people enrolled in ACA marketplace plans.
Some states already offer innovative cost-control plans. For example, Massachusetts now requires issuers of individual coverage and fully insured group coverage to limit increases in the enrollees’ out-of-pocket costs to the Consumer Price Index inflation rate for the Boston area. For 2027, the cap will be 3.6%. The covered expenses include plan deductibles, copayments and coinsurance bills.
When the idea of loans from insurers like UnitedHealth was reported in The New York Times, an attorney commented on social media that “it’s hard to top this level of dystopia.” This is a wake-up call to focus on the real pathways to affordable health care.
In today’s issue:Hospitals are facing simultaneous payment cuts, new oversight and transparency proposals as policymakers look to rein in health care spendingDemocrats are making the GOP’s tax-and-spending law a centerpiece of their midterm messaging as Republicans pivot to selling its tax cutsA federal judge temporarily blocked Colorado’s first-in-the-nation prescription drug payment cap, handing Amgen an early win… and more.Happy Monday, and welcome back to Health Brief. Hope everyone had a relaxing holiday! Congress isn’t here this week, but the health policy world is showing no signs of slowing down. So let’s get into it. What do you have on your radar?
Speaking of the $900 billion in impending cuts to Medicaid: The One Big Beautiful Bill Act was supposed to be a crowning legislative achievement for Republicans to tout while campaigning in the midterm elections. Among other things: It prevented massive tax increases for most Americans and established a program that allows parents to open investment accounts for children born during President Donald Trump’s second term and receive $1,000 from the government. But the legislation has emerged as a central talking point for the Democratic Party, with congressional Democrats mentioning the law twice as often as Republicans, report Matthew Choi and Clara Ence Morse in The Washington Post newsroom. Democratic candidates are deriding it as the “Big Ugly Bill” and linking the changes it brought to Medicaid and food assistance programs to voters’ anxieties about the cost of living. Republicans, meanwhile, have largely retreated from talking about the law by name, instead opting to emphasize the tax savings and other proposals. Democrats assert that the shift is a sign of the Republican Party’s acknowledgment of the law’s low overall approval. “I don’t care what you call it. It’s what delivers for America,” House Republican Conference Chair Lisa McClain (Michigan) told my colleagues.
Read the full story: “Democrats invoke ‘big, beautiful bill’ far more than Republicans as midterms near. ”INDUSTRY RXA federal judge temporarily blocked Colorado from enforcing a state-set payment cap on a pricey medication for autoimmune disorders called Enbrel, siding with Amgen, the company that makes it, while the lawsuit moves forward. The case centers on whether Colorado’s Prescription Drug Affordability Review Board has the authority to limit what can be reimbursed for a patented drug. The board had determined that Enbrel was unaffordable and set a maximum payment level at roughly 70 percent below Amgen’s wholesale price. The judge found that Amgen is likely to win because an earlier federal appeals court ruling says states cannot impose price caps on patented drugs if doing so conflicts with federal patent law. The court said Congress — not individual states — gets to decide how to balance affordable drug prices with the financial incentives that patents provide for developing new medicines. The judge also agreed that Amgen could suffer “significant harm” if the cap took effect, including weaker negotiating power with wholesalers and contracts that would be difficult to undo later. It rejected the state’s claims that any harm was balanced by carveouts in the law, such as the payment limit applying to employer-based plans. “This is an argument about the scope of damages, not their existence,” the judge wrote.
Why it matters: States across the country have been setting up their own Prescription Drug Affordability Boards (PDABs) in an effort to try and rein in drug costs. Some act as advisory panels that develop policy, while others — including Colorado — are able to set upper payment limits. Enbrel’s price cap became the first in the nation, proving to be a test for other PDABs nationwide.The boards’ overall effectiveness and ability to lower medication prices in the states in which they’ve been established has come into question and became one of the reasons Democratic Gov. Abigail Spanberger (Virginia) vetoed bipartisan legislation to set up a PDAB in the state.“Drug manufacturers took a huge sigh of relief from this decision,” Andrew Twinamatsiko, a director of the Center for Health Policy and the Law at Georgetown Law, tells me.For now, Colorado cannot enforce the payment limit for Enbrel while the lawsuit continues. The ruling does not decide the entire case, but it pauses the state’s price cap until the court reaches a final decision.
What’s next: The court leans on a federal ruling that struck down a pharmaceutical price gouging law in Washington D.C., but Twinamatsiko said that structure of the law — which utilized international reference pricing — is different from how Colorado’s PDAB operates and “there are creative ways” the state could differentiate the two legally.
The tax and spending law known as H.R. 1 includes provisions to revise what is counted as a Medicaid payment error and to recoup more federal funds. The new rules, which go into effect in 2029, target payments with inadequate documentation.
Goals: To review the scope of improper Medicaid payments and the potential impact of H.R. 1 policies on states, providers, and patients.
Methods: Analysis of research, government data, proposals, final rules, and laws.
Key Findings and Conclusion:
Although the provisions aim to reduce erroneous Medicaid payments, error rates could rise due to new Medicaid work requirements and other H.R. 1 provisions that make eligibility determination processes more complex for states. More than 20 states already have improper payment rates that exceed the threshold, meaning they could face significant financial penalties when the provisions go into effect. Policymakers could help reduce payment errors and the financial risk to states by encouraging the Centers for Medicare and Medicaid Services (CMS) and the U.S. Department of Health and Human Services to share best practices with states, use state audit data to improve oversight, and streamline Medicaid regulatory requirements. Additionally, CMS and states already have processes in place — including corrective action plans — to address erroneous payments.
Introduction
The tax and spending law, H.R. 1 (originally titled the “One Big Beautiful Bill”), enacted in July 2025, includes more than $900 billion in cuts to Medicaid, the public health insurance program financed jointly by the federal government and states. Some analysts have projected that, along with the law’s other changes to Medicaid, these cuts — the largest in the program’s 60-year history — will cause more than 7 million Americans to lose their Medicaid health coverage.1 The cuts will also shift costs to states, weaken the fiscal stability of health care providers, and diminish patients’ access to care.2
Supporters of H.R. 1 have asserted that it contains measures to address fraud, waste, and abuse. One of these provisions requires the U.S. Department of Health and Human Services (HHS) to recoup federal dollars for erroneous Medicaid payments — such as payments made for medical services when billing paperwork was missing or Medicaid eligibility paperwork was incomplete — once those payments exceed a certain level. The most recent data from the Centers for Medicare and Medicaid Services (CMS) released in January 2026 indicate that the nationwide error rate is 6.12 percent, slightly more than twice the 3 percent rate allowed under H.R. 1.3 According to that report, 77.17 percent of erroneous payments are due to incomplete documentation (namely missing paperwork), which is not generally indicative of fraud or abuse.4
The Congressional Budget Office (CBO) estimates that the policy change will reduce federal Medicaid spending by $7.55 billion and cause 100,000 individuals to lose their coverage as states tighten their processes to avoid penalties.5 To reduce error rates to comply with the new requirement and avoid financial penalties, states could further restrict eligibility determination processes to add greater certainty to ensuring all documentation has been submitted or require prior authorization before a provider can provide care.
Cumulatively, the implementation of H.R. 1’s broader Medicaid changes — such as implementation of work requirements, more frequent coverage renewals for certain enrollees, and changes to provider taxes — could make reducing improper payments more difficult.6 These changes will increase the administrative burden for states and patients while decreasing the funding available for Medicaid programs. With more administrative requirements and fewer dollars with which to implement programs, the chance of error increases.
This brief defines erroneous Medicaid payments and explores whether improper payment rates are an accurate measure of fraud. We describe how H.R. 1 expands the definition of an erroneous payment while limiting the federal government’s ability to waive penalties on states with improper payment rates that exceed a certain threshold even if they are making good faith efforts to address the errors. We also present data showing the disproportionate impact on some states and offer alternative strategies for policymakers to better support states in reducing improper Medicaid payments.
Defining Improper and Erroneous Medicaid Payments
Improper Medicaid payments, as defined in statute, can be overpayments, underpayments, and payments where there is not enough information to determine whether the payment was correct — such as when medical billing codes are inaccurate, provider paperwork is missing, or applicants submit incomplete documentation. Improper payments also include payments made for individuals who were enrolled in Medicaid despite being ineligible, as well as payments for services that do not comply with Medicaid program requirements such as duplicative payments.
The federal government determines what’s “improper” by reviewing Medicaid fee-for-service claims, managed care payments, and eligibility decisions. “Improper payments” is a broad category, while “erroneous payments” — payments that are incorrect under program rules — represent a more specific subset within it.7 Sometimes the terms are used interchangeably.
How CMS Defines Improper Payments
Improper payments can result from a variety of circumstances, including:
Items or services with no documentation.
Items or services with insufficient documentation.
Items or services with documentation that does not substantiate the payment.
Items or services where the payment was to the right recipient for the right amount, but the payment process did not comply with applicable statutory or regulatory payment requirements.
With respect to Medicaid and CHIP, there is no record of the required verification of an individual’s eligibility factors, such as income.
According to CMS, the improper payment rate is not a “fraud rate” but rather a measurement of payments made that did not meet statutory, regulatory, or administrative requirements.8
More than 75 percent of improper payments — just over 77 percent in 2025, as mentioned above — are due to insufficient documentation, and most involve a state, contractor, or provider missing an administrative step.9 With additional documentation, these payments may be correct.
Calculating Improper Medicaid Payments
Each year, CMS conducts a payment error rate measurement (PERM) audit in 17 states — one-third of all states — so every state is reviewed once every three years. Each state’s improper payment rate is calculated by dividing the total value of overpayments and underpayments in a representative sample from three categories (Medicaid eligibility, fee-for-service, and managed care) by the state’s total Medicaid expenditures.10 CMS also publishes a national Medicaid improper payment rate, which was 6.12 percent in the most recent data.11 In 2025, these improper payments totaled $37.9 billion, including $10.8 billion (28.6%) from fee-for-service Medicaid, $27.0 billion (71.4%) from eligibility, and $0 from managed care Medicaid.12
Since 1983, federal law has set an allowable improper payment rate of 3 percent. When a state exceeds this threshold, the HHS secretary is required to recover the federal share of the excess erroneous payments as a penalty. However, the secretary has long had discretion to waive these repayments if a state was making a good faith effort not to exceed the allowable error rate, and the secretary has generally waived penalties.13
Medicaid Improper Payment Rate for Fiscal Year 2025
Medicaid appropriate federal payment rate: 93.88%; $573.6 billion
Percentage of improper payments resulting from insufficient documentation: 77.17%
Notes: Each year approximately 17 states are reviewed. The national improper payment rate is a combination of the more recent three cycles in 2023, 2024, and 2025. In contrast to the 3 percent allowable error rate for Medicaid, Medicare is allowed a 10 percent error rate.
What Is the Current Process for States to Address Error Rates?
States are required to develop a Medicaid corrective action plan (CAP) and submit it to CMS within 90 days of receiving their PERM error rate to address the errors identified in the PERM review.14 The CAP serves as the formal vehicle through which the state explains why errors occurred and identifies root causes across fee-for-service, managed care, and eligibility categories. In the CAP, which is intended to serve as a performance management tool, a state also commits to specific corrective actions designed to reduce future improper payments.
Once CMS approves the state’s PERM CAP, the state is required to implement the corrective actions in accordance with the approved schedule, usually over the course of multiple years. CMS collaborates with states by providing guidance, technical assistance, templates, and other supports.15 All states are required to keep CMS updated regarding the status of the CAP implementation, but states with PERM error rates above 3 percent are required to do so every other month according to federal regulations.16
A state is deemed to be making a good faith effort if it is meaningfully implementing its CAP in alignment with the underlying regulation even if the state has not yet fully eliminated improper payments. As mentioned, historically the HHS secretary has been allowed to waive penalties if the state was making a good faith effort; however H.R. 1 eliminates the option to do so.
Key Findings
H.R. 1 expands what’s considered an erroneous payment and restricts HHS’ authority to waive penalties.
The law alters erroneous payments, which are included in CMS’ PERM audits, in two primary ways: it expands the definition of an erroneous payment, and it adds restrictions to HHS’ ability to waive the penalty for erroneous payments.
Widening the scope of erroneous Medicaid payments. H.R. 1 expands the definition of erroneous payments to include payments made on behalf of individuals who the state does not know for sure are eligible for Medicaid because insufficient information is available to prove their eligibility (such as someone whose documentation was not saved correctly at enrollment or renewal). Expanding the definition in this way risks overstating improper activity by the states by equating administrative uncertainty with fraud.
Restricting HHS’ authority to waive penalties. The law also limits which erroneous payments can be waived: HHS can waive up to the total amount paid in overpayments on behalf of eligible individuals, or payments where there is not enough information available to prove eligibility. HHS can no longer waive penalties for payments made on behalf of individuals who were ineligible for Medicaid, or for services provided to patients with insufficient information to confirm their eligibility. Guidance from CMS will clarify how this will be implemented. Ultimately, this change takes away HHS’ flexibility to waive financial penalties when states are making good faith efforts to address their errors.
H.R. 1 also expands the type of audits that can be used to determine Medicaid erroneous payment rates. Whereas historically these audits have been conducted by CMS, the law gives the secretary authority to conduct audits directly or to use state audits, such as the Medicaid Eligibility Quality Control program.17
These erroneous payment provisions take effect in fiscal year 2030, which begins on October 1, 2029. In November 2025, CMS indicated that it plans to issue further guidance to states on how to implement this section of the law.18 That guidance has not yet been released and could come in the form of preliminary guidance or a proposed regulation. H.R. 1 does not require CMS to use a specific regulatory pathway for implementation.
H.R. 1’s erroneous payment provisions will have a disproportionate impact on some states.
The following table illustrates the state rates during the most recent audits, including which states had rates over the 3 percent threshold, making them subject to penalties under the new law starting in 2029. As mentioned, the most recent national Medicaid PERM rate is 6.12 percent.19
H.R. 1 already puts extensive strain on state budgets, shifting costs for Medicaid, the Supplemental Nutrition Assistance Program (SNAP), and other programs from the federal government to states. The erroneous payment provision contributes to this by adding yet another potential reduction in federal funding and further jeopardizing states’ fiscal stability. In response, states may adopt stricter approaches to eligibility determinations, such as requiring complete documentation or prior authorization before payments are made. These changes could delay treatment for patients, add additional medical debt or uncompensated care if care is not covered, add additional administrative burden for patients and providers, and put states out of compliance with federal application processing times.
Although the provision is intended to reduce erroneous payments, error rates are likely to rise as states implement other H.R. 1 provisions that make processes more complex — such as adding Medicaid work requirements and doubling the frequency of eligibility redeterminations for individuals eligible for Medicaid under the Affordable Care Act Medicaid expansion. These changes increase the risk of errors, and states may not have sufficient time to fully adjust before the new erroneous payment rules go into effect in 2029.
Recommendations for Reducing Fraud, Waste, and Abuse
Given the potential negative impact of the H.R. 1 provisions on states, policymakers have an opportunity to identify other options that could be more effective at reducing erroneous Medicaid payments. The Medicaid and CHIP Payment and Access Commission (MACPAC), Government Accountability Office (GAO), and National Association of Medicaid Directors (NAMD) have each offered recommendations to reduce unnecessary spending in Medicaid.20
About Medicaid Program Integrity
When designed and implemented well, program integrity initiatives help to ensure that:
eligibility decisions are made correctly
prospective and enrolled providers meet federal and state participation requirements
services provided to enrollees are medically necessary and appropriate, and
provider payments are made in the correct amount and for appropriate services.
Of these, NAMD’s recommendations are particularly helpful to consider as state Medicaid agencies share the federal government’s commitment to safeguarding Medicaid funds. Program integrity efforts depend on effective collaboration between state Medicaid agencies and CMS. NAMD recently outlined five core areas of recommendations to improve program integrity in Medicaid:
Strengthen the federal and state partnership through training, technical assistance, and structured collaboration. Expanding access to the Medicaid Integrity Institute and strengthening peer-to-peer learning opportunities are two options. Other strategies include enhancing the role of the Fraud, Waste, and Abuse Advisory Group and convening key program integrity partners, including Medicaid agencies, program integrity units, and others.
Provide targeted support for high-risk service areas that present elevated program integrity risks. Suggestions include developing national risk indicators for high-risk services and providers, and offering more targeted guidance on monitoring strategies, including more frequent provider reverification and clearer documentation expectations.
Improve data sharing and national visibility. Enhancing use of CMS’ nationwide dataset, the Transformed Medicaid Statistical Information System (T-MSIS), could allow program integrity efforts to be driven by actionable nationwide data — rather than a single state’s data. Agencies could then identify cross-state billing patterns, detect emerging fraud schemes, and flag providers operating across multiple jurisdictions.
Enhance information sharing on providers and enforcement actions across programs. This would involve shifting from passive data collection to actionable intelligence across multiple programs, such as Medicaid, Medicare, and Veterans Affairs.
Expand access to tools, technology, and analytic capacity to support program integrity efforts. Predictive modeling, data analytics, interoperable systems, cross-program datasets, and artificial intelligence tools — with appropriate safeguards — could help states develop a more complete picture and effectively identify suspicious patterns.
Additional details regarding these recommendations are available from NAMD.21
Of note, these strategies — as well as those set forth by MACPAC22 and GAO23 — are collaborative, not punitive. They focus on ensuring states have the resources they need to effectively prevent and address erroneous payments. They acknowledge that as fraud schemes grow increasingly complex and span multiple programs and jurisdictions, stronger coordination, expanded data sharing, and more closely aligned federal and state/territorial strategies are needed to effectively identify and address emerging risks. Both states and CMS can play key roles in helping this happen effectively.
In contrast, H.R. 1’s erroneous payment provisions — combined with the law’s broad Medicaid cuts — create considerable financial risk for states without pairing that with the supports necessary for states to effectively address erroneous payments. As a result, states may need to limit coverage or erect barriers to services for beneficiaries, who are the least likely actors to commit fraud against Medicaid.24
HOW WE CONDUCTED THIS STUDY
This study was conducted by analyzing the underlying statute of the One Big Beautiful Bill (H.R. 1) that was signed into law on July 4, 2025; reviewing CMS data on Medicaid program integrity, including the most recent data from FY2025 that was released in 2026; analyzing relevant regulations that govern requirements related to improper payments and Medicaid corrective action plans; reviewing the preliminary and interim guidance released by the Centers for Medicare and Medicaid Services (CMS) to date to implement H.R. 1; reviewing previous guidance from CMS regarding erroneous payments; reviewing recommendations from advisory bodies such as the Medicaid and CHIP Payment and Access Commission (MACPAC) and the Government Accountability Office (GAO); considering recommendations from entities such as the National Association of Medicaid Directors; and conducting a literature review.
To avoid losing funding, many states are pursuing proven cost-saving strategies like downsizing inpatient care rather than untested approaches, some experts say.
Listen to the article7 min
The Rural Health Transformation Program is beginning to reshape how hospitals in rural America deliver care. But with nearly a trillion dollars in Medicaid cuts looming and pressure to show results or risk losing funding, many states are pursuing the safest path available: paying hospitals to downsize.
Congress established the $50 billion, five-year fund under the One Big Beautiful Bill Act to improve healthcare access, quality and outcomes in rural areas — and to win over a handful of Republicans who threatened not to vote for the bill over concerns it would gut Medicaid funding and take out rural hospitals in the process.
The funds are meant to improve rural healthcare access, which has been declining in the U.S. for years. More than 100 rural hospitals have closed in the past decade, and more than one-third are at risk of closing, according to the nonprofit Center for Healthcare Quality and Payment Reform.
The OBBBA will reduce Medicaid spending by an estimated $911 billion over the next decade and increase the number of uninsured people by 10 million, according to the Congressional Budget Office. The RHT program, meanwhile, could offset 37% of the estimated cuts to federal Medicaid spending in rural areas, or about 5% of the total estimated cuts to federal Medicaid spending, according to a KFF analysis of the CBO’s estimates.
In light of the massive funding cuts, the RHT program may not live up to its promises, experts say.
“If we weren’t facing a trillion-dollar cut in the Medicaid program over the next 10 years, this could be a once-in-a-generation policy,” said Bradley Cunningham, a regulatory and policy analyst at the Association of American Medical Colleges.
In December, all 50 states received their first-year awards, totaling $10 billion and averaging roughly $200 million per state. The program caps direct care spending at 15% of funds, steering the bulk of the remaining money toward infrastructure, technology, workforce and new care models.
However, states only had about seven weeks to prepare their applications. So, their plans largely focus on proven cost-cutting strategies rather than innovation, and now they’re locked into whatever they proposed.
“They had to prioritize speed over thoroughness,” said Aaron Bujnowski, a managing director with the healthcare industry group at consultancy Alvarez & Marsal.
As a result, rural health systems in at least 25 states will need to rightsize to receive funding, NPR reported in April. That can mean cutting services, such as dialysis or labor and delivery, or subsidizing conversions to the Rural Emergency Hospital designation, which requires eliminating inpatient care.
That could affect academic medical centers and other large providers, as they often absorb patients when rural facilities cut services or close. The wave of rural hospital closures over the past decade has already pushed patients to urban academic health systems, increasing volumes and straining capacity.
The point was driven home by an AAMC member who ran the only academic medical center in his state, said Leonard Marquez, senior director of government relations and legislative advocacy at the AAMC.
“He looked at me and said, ‘If my rural hospitals are not healthy, I cannot be healthy,’” Marquez said.
Five buckets, 50 plans
States are taking sharply different approaches to the RHT program. Bujnowski identified five broad categories: Downsizing and REH conversion, as in Kansas and Montana; workforce development, including Maine’s expanded scope of practice for physician assistants; technology and alternative payment models, with 42 of 50 states including some form of value-based care expansion; social determinants of health, including food-as-medicine programs in Arkansas and Pennsylvania; and states that are still refining their plans.
The applications for funding were “so divergent” that it’s difficult to discuss the program in holistic terms, Cunningham said.
Moreover, the program’s clawback authority, which allows the CMS to reduce a state’s funding in subsequent years if it fails to demonstrate outcomes, is weighing heavily on states’ decision-making.
Read More in Hospitals
Because of this, states have strong incentives to pursue proven models rather than untested approaches, as they must demonstrate measurable progress in the first year or risk losing funding in the second.
That dynamic likely limits innovation and spurs cuts because reducing services will quickly lead to direct and measurable progress. So, states are more inclined to expand capitated primary care payments or subsidize REH conversions — interventions with existing track records — than attempt something novel without a demonstrated history of results.
Still, not everyone sees the service cuts as a loss.
Framing the program as incentivizing hospitals to shrink is misleading, said Robert Parris, a managing director who leads government-focused healthcare advisory work at consulting firm Huron. What’s actually happening, he said, is that communities are getting more of what they need and less of what they don’t.
“It’s more about reallocation as opposed to taking away,” Parris said.
The program is also shifting how leaders think — from what services a facility can provide within its own walls to what care the surrounding population actually has access to, said Paul Johnson, a managing director who works directly with rural hospital clients at Huron.
Many hospitals had these changes on their wish lists for years, but they couldn’t justify the investment because they were focused on surviving the next budget cycle.
“It’s almost like a license for them to pivot into things that they know they’ve had to do,” Johnson said.
Programs over people
But with nearly half of rural hospitals operating in the red, the 15% direct-care cap doesn’t replace what they lost from Medicaid cuts, forcing difficult decisions about which services to keep.
Hospital boards are weighing four options, Bujnowski said: Close services, convert to a Rural Emergency Hospital, develop truly innovative payment models or improve access to technology like digital health tools.
In many instances, the first two offer the clearest path to continued funding under the RHT program.
The need to demonstrate outcomes, as well as the looming threat of funding clawbacks, could also cause hospital leaders to become overly focused on program management at the expense of the communities they serve.
“The most common mistake could be to put programs over people,” Bujnowski said.
The best leaders will ensure their initiatives stay aligned with what patients in their communities actually need. Boards should ask what sustained, community-appropriate care looks like beyond 2030, when the program’s funding runs out.
“That should be your North Star,” Bujnowski said.
But whether the program’s limitations allow for genuine transformation — or simply a managed, federally-funded downsizing — is a question that won’t be answered for years.
This week we’re highlighting a trio of stories that shed new light on issues An Arm and a Leg has been tracking closely:
A sharp investigation from our partners KFF Health News on who’s actually filing medical debt lawsuits.
How one state is cracking down on aggressive medical credit card marketing.
Some new, encouraging data suggesting more seniors can afford their medications.
Let’s go!
In at least one state, doctors are now suing patients more than hospitals are
One of the most perplexing realities we’ve come across while reporting on the U.S. health care system (and there are MANY) is this: Hospitals routinely sue their patients over medical debt, yet recoup very little money in the process. So why do they bother?
In fall 2023, we published a two–part investigation with Scripps News and The Baltimore Banner digging into that question.
Since then, we’ve been tracking efforts by advocates, lawmakers, and federal agencies to rein in the most aggressive medical debt collection practices — like destroying a patient’s credit, garnishing their wages, or foreclosing on homes.
And now, in at least one state — Connecticut — KFF Health News and the CT Mirror found that public pressure persuaded many hospitals to stop suing patients over medical debt altogether. Cool!
And recent legislation targeting aggressive medical debt collection practices doesn’t cover non-hospital health care providers. Neither do medical debt protection laws in most other states.
As one Connecticut state senator put it, lawmakers will need to to “go bigger if that’s where the heart of the matter is.”
On a brighter note, Connecticut has passed another law looking out for people facing medical debt…
New rules around CareCredit and other “medical” credit cards
Last week, Governor Ned Lamont signed a bill limiting the aggressive and confusing marketing of medical credit cards inside doctors’ offices and veterinary offices.
Connecticut joins California, Illinois, and New York in passing laws to protect patients from these financial traps.
Health care providers are increasingly pushing medical credit cards as an alternative to in-house payment plans. CareCredit, the biggest player in the field, says these cards are accepted at more than 285,000 locations, including many hospitals.
The appeal for providers is pretty straightforward: Outsourcing billing to a third party reduces administrative burden.
According to Patricia Kelmar, senior director of health campaigns with PIRG, patients frequently don’t understand what they’re agreeing to — whether they’re handed a form at the front desk or an iPad in the exam room.
“It’s just not the place to be looking at terms and conditions,” she says.
As we covered in a previous First Aid Kit, those terms and conditions usually include something scary: deferred interest. In most states, medical debt tied to medical credit cards also isn’t protected by the same consumer laws that cover regular medical debt — New York being the notable exception.
Connecticut’s new law adds meaningful friction that could make it harder for patients to sign up for something they don’t understand:
Health care providers can no longer submit or help fill out applications on a patient’s behalf.
Provider logos are banned from credit card marketing materials, making it clearer the card isn’t affiliated with the doctor or hospital.
Providers can’t charge these cards for services covered by Medicaid.
Kelmar, who’s collecting stories from patients, says it’s a step forward — and a pretty unlikely one, given that Synchrony Financial, which operates CareCredit, is based in Stamford, CT.
Apizza, anyone?
A law from 2022 is making a real difference for seniors
A new study in JAMA finds that legislation capping out-of-pocket prescription costs for seniors has helped many stay on top of their medications.
And, as Undark explains, those good results may be only the beginning. The law was only beginning to phase in during 2024; the full out-of-pocket cap took effect in 2025, and the study’s authors expect even stronger results to follow.
The Trump administration has announced that it will significantly expand access to so-called catastrophic health insurance plans, which are policies with comparatively low monthly premiums but deductibles so high they often leave families effectively uninsured until a medical crisis strikes. CMS described the move as giving Americans “flexibility” and improving access to “affordable healthcare coverage.” But what I call them are “junk plans”.
Back in October, I warned that these plans (often called short-term, limited-duration insurance plans, or STLDIs) were poised for a comeback as enhanced Affordable Care Act subsidies expired and millions of Americans faced sharp premium increases. Well, now these plans are, in fact, a reality.
The Affordable Care Act outlawed most of these junk-style plans because the law requires insurers to cover health care services people need, including prescription drugs, hospitalization, mental health care and maternity care. The ACA also forced insurers to spend most premium dollars on medical care instead of executive compensation, advertising and shareholder returns.
But the ACA never fully solved the deeper affordability crisis in American health care. Premiums have steadily become much too high. Deductibles and other out-of-pocket requirements have put care out of reach for millions as insurers have continued to shift more costs onto patients while simultaneously becoming larger, more powerful and more profitable. The shortcomings of the ACA and the decisions by the President and congressional Republicans have created the perfect opening for catastrophic plans to return.
Affordability’s all the buzz, but Trump’s sweeping payment rule emphasizes consumer choice over cost control.
When families are staring at monthly premiums they can no longer afford, a cheaper option — even one loaded with massive deductibles and coverage gaps — starts looking attractive. That is exactly what insurers are counting on.
In my old job at Cigna, I helped market plans like these. In my book Deadly Spin, I called them what they often really are: “the illusion of coverage.” These policies were designed to look like insurance while minimizing the likelihood insurers would actually have to pay significant claims. Companies like UnitedHealth Group and other insurance and health care conglomerates make enormous profits on catastrophic-style plans because the deductibles are so high and the restrictions so extensive that relatively few claims ever get paid.
Supporters of these plans frame them as “consumer choice.” But choice is a misleading word when many Americans are being financially cornered into skimpier coverage because comprehensive insurance has become unaffordable. People do not think they will get cancer before it happens. No one expects a devasting car crash or for their kid to come down with a confusing illness. The danger with junk plans is that people undoubtedly only discover how weak their coverage is after their lives have already been turned upside down.
And so, both parties in Washington deserve criticism. Republicans are now openly expanding access to catastrophic-style plans. But Democrats also bear responsibility for defending a post-ACA system that still leaves millions of Americans underinsured and financially exposed. Expanding coverage was enormously important. But coverage alone is not enough if using that coverage can still bankrupt you. We need a comprehensive update to the consumer protections in the ACA – expanding junk insurance is not that – and Republicans know better.
The real danger now is that America slowly normalizes a health care system where people are expected to carry insurance cards that offer little meaningful protection until disaster strikes. Once that becomes acceptable, legitimate insurance and junk insurance become indistinguishable.
There are a lot of eye-popping statistics that capture the burden high health care costs put on so many Americans. Nearly three in 10 adults say they have problems paying medical bills. More than 40% say they skip medications because of the cost.
The stat that always stops me in my tracks is the fact that Americans have nearly $200 billion in unpaid medical bills in collections,according to one recent estimate. The average consumer facing collections in 2020 had more medical debt than all other sources of debt — credit cards, phone, utilities — combined.
“If a debt collector is calling you up or is knocking on your door, more than half of the time, it’s for medical debt,” said Neale Mahoney, a Stanford University economist and one of the nation’s leading scholars on medical debt.
Mahoney has spent two decades studying the scale of the country’s medical debt problem, as well as the effectiveness of policies intended to relieve people’s medical debt. From 2022-2023, he worked in the Biden administration on regulations to remove unpaid medical bills from people’s credit reports.
We talked with Mahoney about the fate of those regulations under the Trump administration, and what we’ve learned about the best way to protect people from getting medical debt in the first place.
Here are a few of the takeaways:
The Trump administration is rolling back Biden’s regulation of medical debt. Credit agencies sued to prevent the federal government from banning overdue medical bills from credit reports, and the White House declined to defend it. New guidance under Trump also challenged state protections for medical debt.
Nonprofits — and some local governments — have paid off medical debt for millions of Americans, in hopes of easing stress and improving people’s health. Mahoney’s research points to bigger improvements in health outcomes for patients who got debt relief sooner rather than later. One recent study showed patients who got their bills cleared within a few weeks of getting care were more likely to get diagnosed and treated for heart disease and diabetes than those who didn’t get help. However, an analysis of people who had their debts wiped after carrying them for years found no improvements to self-reported physical or mental health.
Mahoney believes helping patients avoid medical debt through health insurance or hospital financial assistance, which wipes out some or all of a patient’s bill, is the most effective approach. Many people, however, struggle to take advantage of either due to obstacles like restrictions from insurers and extensive applications to get help from hospitals. Patients caught up in what Mahoney has dubbed “the annoyance economy” often end up in money-losing fights. “For too many of us, navigating the U.S. health care system can feel like a second job,” Mahoney said, “at the precise moment when we don’t have the time and energy to take on a second job.”
One promising option to prevent people from falling into medical debt, Mahoney said, is for hospitals to auto-enroll eligible patients for financial assistance — a process known as “presumptive eligibility.” California, Illinois, Oregon and North Carolina have adopted auto-enrollment requirements for hospitals, and more states are considering it. “I would be eager to see hospitals working on this and sharing best practices,” Mahoney said, “so that we can provide relief to people who need it while still recovering payments from people who can afford it.”
One of those reasons is the growing number of states looking to require hospitals to auto-enroll patients in financial assistance programs. I’ve been reporting on this idea of presumptive eligibility for years, and for the last few months, I’ve been working on a special series diving deep into the pros and cons of forcing hospitals to provide more charity care. Those stories will drop this fall.








 Listen to the article7 min
Listen to the article7 min