Cartoon – How’s Your Project Going?



— 2020 drug price increases unlikely to catalyze cost-cutting action, say experts.
Both House Speaker Nancy Pelosi and Republican Sen. Chuck Grassley cited the initial wave of drug price hikes as examples of why their respective bills tackling the cost of pharmaceuticals should move forward. But when Prescription PULSE spoke with a half dozen experts tracking the industry, not one believed the hikes — which averaged around 5 percent across more than 470 drugs — would sway Congress or the administration to drug pricing reform.
“The increases are a persistent reminder that Congress and the administration have done nothing to reduce drug prices. But the increases also happen so regularly that it’s probably unrealistic to think they’ll spur any action this time around,” said Rob Smith, who tracks the political and policy outlook of the drug industry for Capital Alpha Partners.
“I don’t necessarily think the increases themselves improve or diminish the odds of material drug pricing legislation getting across the finish line,” said John Leppard of Washington Analysis.
Of the 471 drugs whose prices have increased, 466 were brand-name medicines, according to GoodRx, which tracks where consumers can get lower-priced medicines. GoodRx doesn’t track doctor-administered drugs so there were likely other increases not captured by their analysis. Other companies are expected to announce price increases as the month goes on.
Despite the focus on drug costs, companies are continuing their habit of regularly raising the prices, often multiple times a year, said Anna Kaltenboeck, a program director and senior health economist at Memorial Sloan Kettering Cancer Center. “This is the starting volley for the year so to speak,” she said.
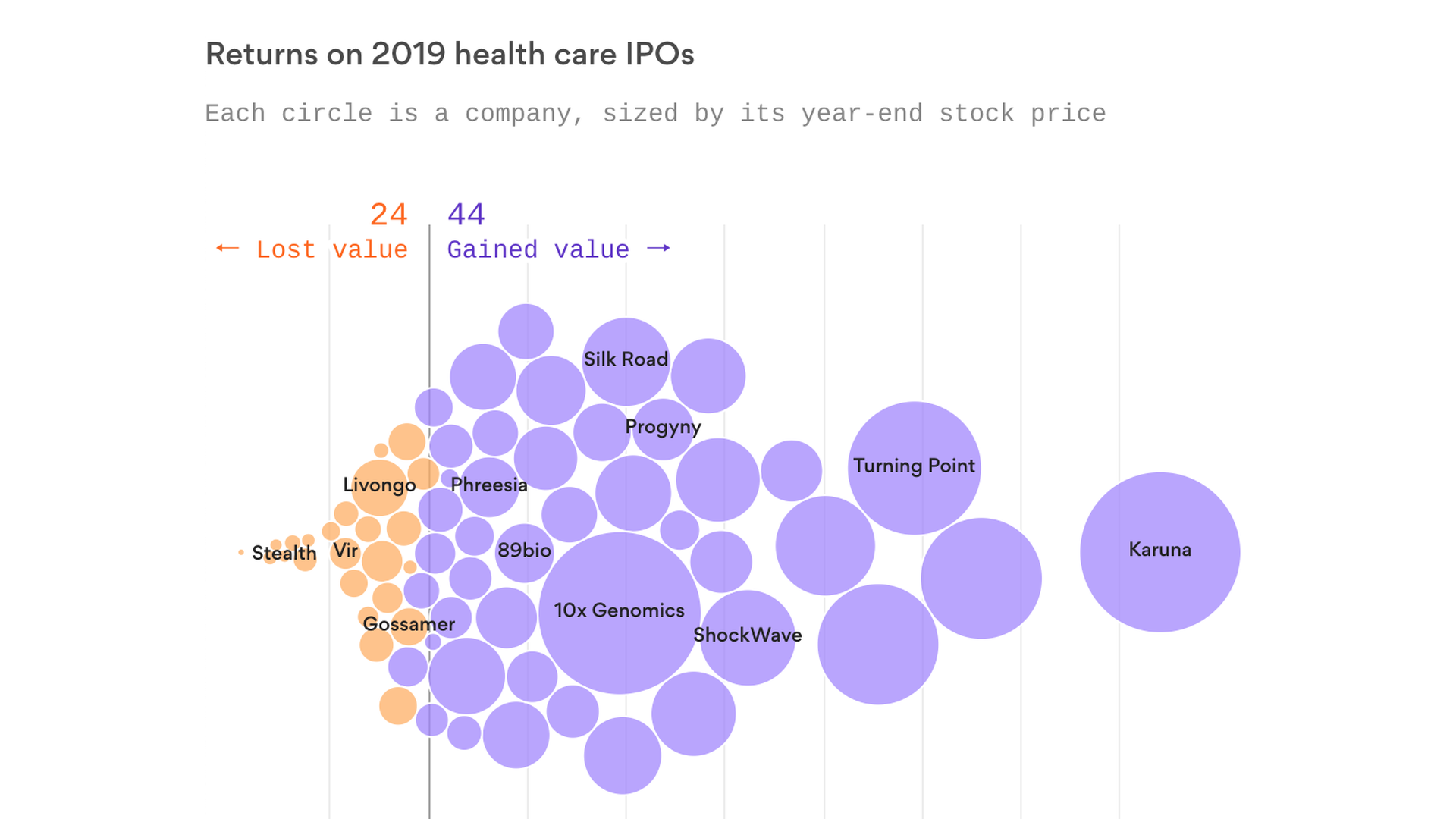
Two-thirds of the 68 health care companies that went public in 2019 traded above their IPO price by the end of year — many of which provided huge initial returns to owners and outside investors, Axios’ Bob Herman reports.
The big picture: The vast majority of health care companies that go public are biotechnology firms. Several of those biotechs in the 2019 class benefited from some promising, but extremely early, clinical trial data.
By the numbers: If you bought an equal amount of shares of every health care company that went public last year and then sold before the calendar flipped, you would have gotten a 47% return on your money.
Winners: Karuna Therapeutics made the biggest leap, as the biotech company’s stock price almost quintupled by the end of the year. Early clinical trial data showed that Karuna’s schizophrenia drug relieved many symptoms, Stat reported.
Losers: SmileDirectClub, which mails teeth-straightening kits, and a handful of biotech startups like Stealth BioTherapeutics saw their stock prices fall by more than half from their IPOs.
The bottom line: Biotech stocks are notoriously fickle. Poor clinical trial data can derail an entire company, and some of these firms inevitably will fail, given the nature of science.
Go deeper: One Medical was one of the first health care IPOs of 2020

Providing close follow-up care from a team of clinical and social workers to the sickest, most vulnerable patients does not reduce hospital readmissions, a new study in the New England Journal of Medicine concludes.
Why it matters: Many doctors and scholars viewed this approach as a promising way to improve care and save money, but it doesn’t appear to do either, Bob writes.
What happened: Unexpected life changes or holes in social programs derailed the lives of many patients who were getting the extra help, and forced them to put their health needs on the back burner.
The bottom line: Giving extra health care support to patients who are struggling with poverty, addiction, hunger and other issues is still the right thing to do.
Go deeper: There is an important difference between “social needs” and “social determinants of health,” health economist Austin Frakt wrote last year.

Some local and state officials want Medicaid to start picking up the tab for inmates’ health care, Stateline reports.
How it works: Medicaid beneficiaries lose their coverage while they’re incarcerated — including pretrial detention for people who can’t make bail — and county governments are generally responsible for providing their care, Axios’ Marisa Fernandez writes.
State and local officials want Medicaid to start paying those bills. A single seriously ill inmate — someone with HIV, for example — can quickly strain county budgets, they said.
40 states have already changed their rules so that Medicaid coverage kicks back in more quickly once people are released from jail.