Medicaid is critical to our nation’s healthcare system, providing necessary care for more than 72 million Americans – including our neighbors and friends.
Who it Affects
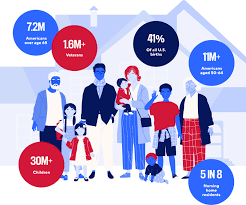
Medicaid covers children, seniors in nursing homes, veterans, people with long-term chronic illnesses, those with mental health issues and working families.
The program helps keep Americans healthy at all stages of life, providing healthcare to families in need — especially as the country continues to recover from record-high inflation.
The Problem
Some policymakers are considering Medicaid cuts that would undermine coverage for countless patients and threaten Americans’ access to comprehensive, 24/7 hospital care.
Medicaid covers health services for patients who otherwise wouldn’t be able to pay for care. Coverage of services is essential for hospitals, and helps ensure all Americans have access to high-quality, 24/7 care, no matter where they live.
Who Medicaid covers
Providing Lifesaving Healthcare Services
Medicaid covers patients with complex and chronic illnesses in need of long-term care, as well as emergency services and prescription coverage.
As the nation faces a growing mental health crisis, Medicaid also ensures millions of Americans — including veterans — have access to mental healthcare and substance abuse services.
Without access to affordable mental healthcare through Medicaid, veterans often lack the long-term support they deserve, and are left to deal with complex health issues years after their service.
In these areas, where primary care providers are few and far between, hospitals become even more vital sites of care — and in some cases, the only sites of care available.
Rural hospitals, already more likely to be at risk of closure, rely on Medicaid funding to stay open and to continue providing lifesaving care to their patients. Nearly 150 rural hospitals have closed or converted since 2010 alone. Further cuts to care would eliminate a lifeline for Americans across the country — with devastating consequences for rural communities.
The Solution
Cuts to Medicaid funding will create irreparable harm for our nation’s most vulnerable communities, including millions of children, veterans, those with chronic illnesses, seniors in nursing homes, and working families. Medicaid helps provide security to these Americans, keeping them healthy at every stage of life.
Congress should vote against efforts to reduce Medicaid funding and instead focus on policies that strengthen access to 24/7 care, rather than take it away.
A pair of senators are asking CMS to require Medicare Advantage plans to cover stays in long-term care facilities at the same rate as traditional Medicare.
Chris Murphy, a Connecticut Democrat, and Thom Tillis, a North Carolina Republican, wrote a letter to CMS Administrator Chiquita Brooks-LaSure Dec. 21, asking the agency to clarify MA plans cannot use different standards to approve long-term care than traditional Medicare.
In their letter the senators wrote they have heard concerns from long-term care hospitals in states that “regularly receive denial letters from Medicare Advantage plans.”
“Unfortunately, Medicare Advantage plan prior authorization practices are creating significant barriers to [long-term hospital] care for critically and chronically ill patients,” the senators wrote.
In a final rule issued in April, CMS said Medicare Advantage plans cannot implement prior authorization criteria that are more stringent than traditional Medicare. In their letter, the senators asked the agency to clarify this statute also applies to long-term care hospitals.
“We write to ask CMS to confirm this interpretation is correct and to request such information be publicly clarified to eliminate confusion for Medicare Advantage plans and ensure that [long-term care hospitals] are treated the same as any other post-acute care provider under the Medicare Advantage regulations,” the senators concluded.
The Medicare Advisory Payment Commission recommends a higher-than-current-law fee-for-service payment update in 2024 for acute care hospitals and positive payment updates for clinicians paid under the physician fee schedule. It recommends reductions in base payment rates for skilled nursing facilities, home health agencies and inpatient rehabilitation facilities.
MedPAC gave Congress recommendations on payment rates in both traditional fee-for-service and Medicare Advantage for 2024, satisfying a legislative mandate comparing per enrollee spending in both programs.
MedPAC estimates that Medicare spends 6% more for MA enrollees than it would spend if those enrollees remained in fee-for-service Medicare.
In their March 2023 Report to the Congress: Medicare Payment Policy, commissioners said they were acutely aware of how providers’ financial status and patterns of Medicare spending varied in 2020 and 2021 due to COVID-19 and were also aware of higher and more volatile cost increases.
However, they’re statutorily charged to evaluate available data to assess whether Medicare payments are sufficient to support the efficient delivery of care and ensure access to care for Medicare’s beneficiaries, commissioners said.
FEE-FOR-SERVICE RATE RECOMMENDATIONS
MedPAC’s payment update recommendations are based on an assessment of payment adequacy, beneficiaries’ access to and use of care, the quality of the care, the supply of providers, and their access to capital, the report said. As well as higher payments for acute care hospitals and clinicians, MedPAC recommends positive rates for outpatient dialysis facilities.
It recommends providing additional resources to acute care hospitals and clinicians who furnish care to Medicare beneficiaries with low incomes. It also recommends a positive payment update in 2024 for hospice providers concurrent with wage adjusting and reducing the hospice aggregate Medicare payment cap by 20%.
It recommends negative updates, which are reductions in base payment rates, for skilled nursing facilities, home health agencies and inpatient rehabilitation facilities.
Acute care
For acute care hospitals paid under the inpatient prospective payment system, commissioners recommend adding $2 billion to current disproportionate share and uncompensated care payments and distributing the entire amount using a commission-developed “Medicare SafetyNet Index” to direct funding to those hospitals that provide care to large shares of low-income Medicare beneficiaries.
This recommendation got pushback from America’s Essential Hospitals.
“We appreciate the Medicare Payment Advisory Commission’s desire to define safety net hospitals for targeted support, but the commission’s Medicare safety net index (MSNI) could have the perverse effect of shifting resources away from hospitals that need support the most,” said SVP of Policy and Advocacy Beth Feldpush. “The MSNI methodology fails to account for all the nation’s safety net hospitals by overlooking uncompensated care and care provided to non-Medicare, low-income patients – especially Medicaid beneficiaries. Any practical definition of a safety net provider must consider the care of Medicaid and uninsured patients, yet the MSNI misses on both counts.”
Feldpush urged policymakers to develop a federal designation of safety net hospitals and to reject the MSNI.
“Further, policymaking for these hospitals should supplement, rather than redistribute, existing Medicare DSH funding, which reflects a congressionally sanctioned, well-established methodology,” she said.
Physicians and clinicians
For clinicians, the commission recommends that Medicare make targeted add-on payments of 15% to primary care clinicians and 5% to all other clinicians for physician fee schedule services provided to low-income Medicare beneficiaries.
The American Medical Association commended MedPAC, but also said that an update tied to just 50% of the Medicare Economic Index would cause physician payment to chronically fall even further behind increases in the cost of providing care. AMA president Dr. Jack Resneck Jr. urged Congress to pass legislation providing for an annual inflation-based payment update.
MedPAC has long championed a physician payment update tied to the Medicare Economic Index, Resneck said. Physicians have faced the cost of inflation, the COVID-19 pandemic and growing expenses to run medical practices, jeopardizing access to care, particularly in rural and underserved areas.
“Not only have Medicare payments failed to respond adequately, but physicians saw a 2% payment reduction for 2023, creating an additional challenge at a perilous moment,” Resneck said. “As one of the only Medicare providers without an inflationary payment update, physicians have waited a long time for this change. When adjusted for inflation, Medicare physician payment has effectively declined 26% from 2001 to 2023. These increasingly thin or negative operating margins disproportionately affect small, independent, and rural physician practices, as well as those treating low-income or other historically minoritized or marginalized patient communities. Our workforce is at risk just when the health of the nation depends on preserving access to care.”
The AMA and 134 other health organizations wrote to congressional leaders urging for a full inflation-based update to the Medicare Physician Fee Schedule.
MGMA’s SVP of Government Affairs Anders Gilberg said, “Today’s MedPAC report recommends Congress provide an inflationary update to the Medicare base payment rate for physician and other health professional services of 50% of the Medicare Economic Index (MEI), an estimated annual increase of 1.45% for 2024. In the best of times such a nominal increase would not cover annual medical practice cost increases. In the current inflationary environment, it is grossly insufficient.”
MGMA urged Congress to pass legislation to provide an annual inflationary update based on the full MEI.
Ambulatory surgical centers and long-term care hospitals
Previously, the commission considered an annual update recommendation for ambulatory surgical centers (ASCs). However, because Medicare does not require ASCs to submit data on the cost of treating beneficiaries, the commissioners said they had no new significant data to inform an ASC update recommendation for 2024.
Commissioners also previously considered an annual update recommendation for long-term care hospitals (LTCHs). But as the number of cases that qualify for payment under Medicare’s prospective payment system for LTCHs has fallen, they said they have become increasingly concerned about small sample sizes in the analyses of this sector.
“As a result, we will no longer provide an annual payment adequacy analysis for LTCHs but will continue to monitor that sector and provide periodic status reports,” they said in the report.
MEDICARE ADVANTAGE
Commissioners said that overall, indicators point to an increasingly robust MA program. In 2022, the MA program included over 5,200 plan options, enrolled about 29 million Medicare beneficiaries (49% of eligible beneficiaries), and paid MA plans $403 billion (not including Part D drug plan payments).
In 2023, the average Medicare beneficiary has a choice of 41 plans offered by an average of eight organizations. Further, the level of rebates that fund extra benefits reached a record high of about $2,350 per enrollee, on average.
Medicare payments for these extra benefits – which are not covered for beneficiaries in FFS – have more than doubled since 2018. For 2023, the average MA plan bid to provide Medicare Part A and Part B benefits was 17% less than FFS Medicare would be projected to spend for those enrollees.
However, the benefits from MA’s lower cost relative to FFS spending are shared exclusively by the companies sponsoring MA plans and MA enrollees (in the form of extra benefits). The taxpayers and FFS Medicare beneficiaries (who help fund the MA program through Part B premiums) do not realize any savings from MA plan efficiencies.
Medicare should not continue to overpay MA plans, MedPAC said. Over the past few years, the commission has made recommendations to address coding intensity, replace the quality bonus program and establish more equitable benchmarks, which are used to set plan payments, the report said. All of these would stem Medicare’s excess payments to MA plans, helping to preserve Medicare’s solvency and sustainability while maintaining beneficiary access to MA plans and the extra benefits they can provide.
PART D
Medicare’s cost-based reinsurance continues to be the largest and fastest growing component of Part D spending, totaling $52.4 billion, or about 55% of the total, according to the report.
As a result, the financial risk that plans bear, as well as their incentives to control costs, has declined markedly. The value of the average basic benefit that is paid to plans through the capitated direct subsidy has plummeted in recent years.
In 2023, direct subsidy payments averaged less than $2 per member per month, compared with payments of nearly $94 per member, per month, for reinsurance. To help address these issues, in 2020 the commission recommended substantial changes to Part D’s benefit design to limit enrollee out-of-pocket spending; realign plan and manufacturer incentives to help restore the role of risk-based, capitated payments; and eliminate features of the current program that distort market incentives.
In 2022, Congress passed the Inflation Reduction Act, which included numerous policies related to prescription drugs. One such provision is a redesign of the Part D benefit with many similarities to the commission’s recommended changes.
The changes adopted in the IRA will be implemented over the next several years, and are likely to alter the drug-pricing landscape, commissioners said.
The Medicare Payment Advisory Commission voted Jan. 14 to recommend a 2 percent raise in Medicare payments for hospitals next year.
The commission said it wants to give the payment boost to both acute-care and long-term care hospitals. The 2 percent payment increase will result in about a $750 million to $2 billion increase in acute-care hospital spending for Medicare and about $50 million for long-term care hospitals.
MedPAC also plans to recommend no change to the payment rate for physicians in 2022 and a 5 percent decrease for home health firms and inpatient rehabilitation centers.
Although MedPAC will recommend the payment boost, Congress is not required to implement the recommendation.
The vote occurred at MedPAC’s January public meeting.
The Medicare Payment Advisory Commission released its March 2020 report on Medicare payment policy to Congress, which includes a chapter analyzing the effects of hospital and physician consolidation in the healthcare sector.
Here are seven takeaways:
1. Medicare’s Insurance Trust Fund is likely to run out without changes. Trustees from Medicare estimate that the program’s Hospital Insurance Trust Fund, mostly funded through a payroll tax, will be depleted by 2026. To keep the fund solvent for the next 25 years, Medicare trustees advise that the payroll tax immediately be raised from 2.9 percent to 3.7 percent, or Part A spending to be reduced by 18 percent.
2. MedPAC recommends boosting payment rate for three sectors:
Hospitals. MedPAC recommended a 3.3 percent raise in Medicare payments for hospitals next year. The commission said it wants to give hospitals a 2 percent boost overall and tie the other 1.3 percent to quality metrics to motivate hospitals to reduce mortality and improve patient satisfaction. Currently, CMS has scheduled a 2.8 percent increase in 2021 Medicare payments.
Outpatient dialysis services. MedPAC recommended that the End Stage Renal Disease Prospective Payment System base payment rate is raised by the amount determined under current law. This is projected to be a boost of 2 percent
Long-term care hospitals. The commission recommended a 2 percent increase in the payment rates for long-term care hospitals in 2021.
3. MedPAC recommends unchanged payment rates for four sectors:
Physicians: Under current law, there is no update to the 2021 Medicare fee schedule base payment rate for physicians who treat Medicare patients. MedPAC is recommending that CMS keeps the physician rate the same as it is this year.
Surgery centers. MedPAC recommended eliminating an expected 2.8 percent payment rate bump for surgery centers next year. It said its decision was due to not having enough cost data from surgery centers.
Skilled nursing. MedPAC is recommending skilled nursing facilities receive no change to their base rate next year to better align payments with costs while exerting pressure on providers to keep their cost growth low.
Hospice. MedPAC recommends that the hospice payment rates in 2021 be held at their 2020 levels
4. MedPAC recommends payment rate reductions for two sectors:
Home health. The commission recommended a 7 percent reduction in home health payment rates for 2021.
Inpatient rehabilitation hospitals. MedPAC is recommending that CMS reduce the payment rate to inpatient rehabilitation facilities by 5 percent for fiscal year 2021.
5. MedPAC builds on its recommendation to revamp quality programs. MedPAC is furthering its recommendation to replace Medicare’s four current hospital quality programs with a single hospital value incentive program. MedPAC said it believes that this recommendation would provide hospitals higher aggregate payments than they would get under current law.
6. MedPAC’s findings on hospital and physician consolidation. MedPAC said that consolidation gives providers greater market power, which has a statistically significant association with higher profit margins for treating non-Medicare patients. Higher non-Medicare margins also are associated with higher standardized costs per discharge. But the direct association between market power and standardized costs per discharge is statistically insignificant, the commission found.
“The effect of consolidation on hospitals’ costs is not clear in theory or from our current analysis. From a theoretical standpoint, the merger of two hospitals could initially create some efficiencies and bargaining power with suppliers. But over time, higher prices from commercial payers could loosen hospitals’ budget constraints and lead to higher cost growth, thus offsetting any efficiency gains,” MedPAC’s report states.
7. MedPAC’s findings on the 340B Drug Discount Program. MedPAC was asked to analyze whether the availability of 340B drug discounts creates incentives for hospitals to choose more expensive products than they would without the program. MedPAC studied the effect of 340B market share on higher drug spending on cancer treatments between 2009 and 2017. The commission found that for two of the five cancer types studied, 340B participation boosted prices by about $300 per patient per month. However, the boost in spending attributed to 340B was much smaller than the general increase in oncology spending, which includes rising prices and the launch of new products with high drug prices. For example, cancer drug spending grew by more than $2,000 per patient month for patients with breast cancer, lung cancer, and leukemia/lymphoma.
“The MedPAC report released today uses rigorous analysis and finds little evidence 340B participation influences cancer drug spending. Modest differences may be attributable to the types of patients treated in 340B facilities. The safety-net hospitals that participate in the 340B drug-pricing program are essential providers of cancer care in this nation, especially to patients who are living with low incomes, those living with disabilities, and patients requiring more complex oncology care,” said Maureen Testoni, president and CEO of 340B Health, an association that represents more than 1,400 hospitals participating in the 340B program.