Wisdom Thought – Character vs Reputation

On November 2-3 in Austin, I moderated the 4th Annual CSO Roundtable* in which Chief Strategy/Growth Officers from 12 mid-size and large multi-hospital systems participated. The discussion centered on the future: the issues and challenges they facing their organizations TODAY and their plans for their NEAR TERM (3-5 years) and LONG-TERM (8-10 years) future. Augmenting the discussion, participants rated the likelihood and level of disruptive impact for 50 future state scenarios using the Future State Diagnostic Survey. *
Five themes emerged from this discussion:
1-Major change in the structure and financing of U.S. health system is unlikely.
2-Health costs, affordability and equitable access are major issues facing the health industry overall and hospitals particularly.
3-The regulatory environment for all hospitals will be more challenging, especially for not-for-profit health systems.
4-By contrast, the environment for large, national health insurers, major (publicly traded) private equity sponsors and national retailers is significantly more positive.
5-The system-wide shift from volume to value will accelerate as employers and insurers drive lower reimbursement and increased risk sharing with hospitals and medical groups.
My take:
The role of Chief Strategy Officer in a multi-hospital system setting is multi-functional and unique to each organization. Some have responsibilities for M&A activity; some don’t. Some manage marketing, public relations and advocacy activity; others don’t. All depend heavily on market data for market surveillance and opportunity assessments. And all have frequent interaction with the CEO and Board, and all depend on data management capabilities to advance their recommendations about risk, growth and the future. That’s the job.
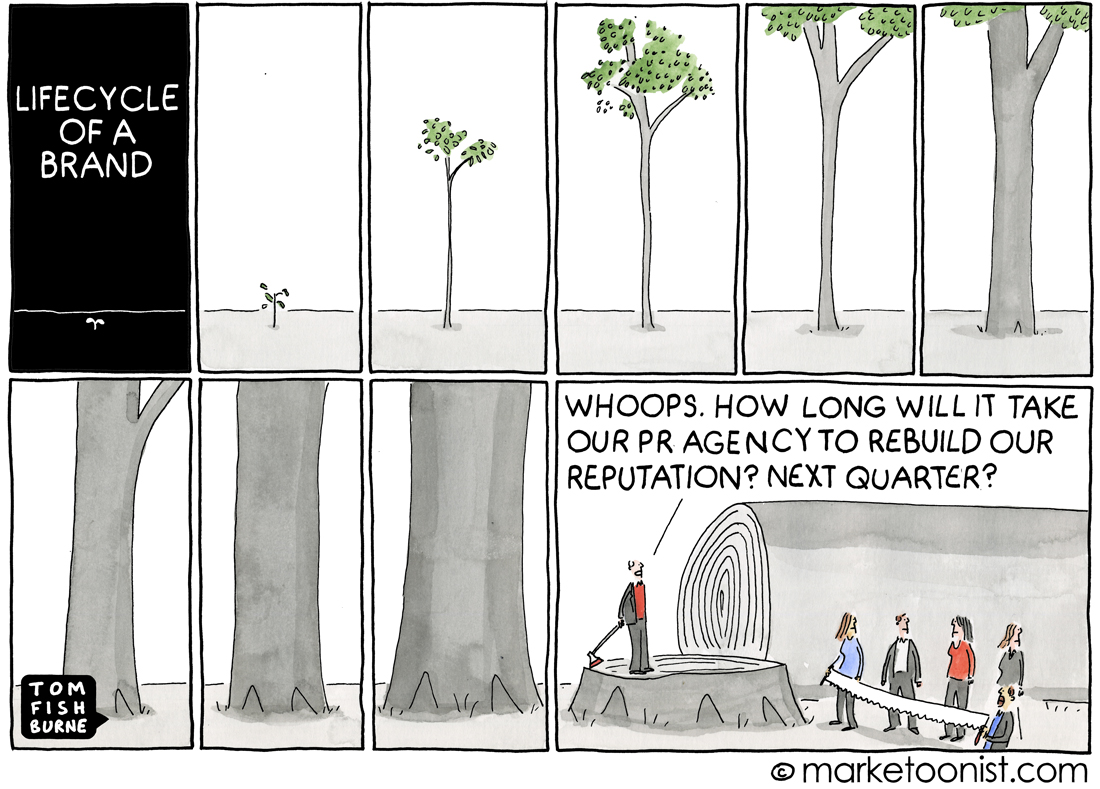
CSOs know that hospitals are at a crossroad, particularly not-for-profit system operators accountable to the communities they serve. In the 4Q Keckley Poll, 55% agreed that “the tax exemption given not-for-profit hospitals is justified by the community benefits they provide” but 45% thought otherwise. They concede their competitive landscape is more complicated as core demand shifts to non-hospital settings and alternative treatments and self-care become obviate traditional claims-based forecasting. They see the bigger players getting bigger: last week’s announcements of the Cigna-Humana deal and expansion of the Ascension-LifePoint relationship cases in point. And they recognize that their reputations are under assault: the rift between Modern Healthcare and the AHA over the Merritt Research ’s charity care study (see Hospital section below) is the latest stimulant for not-for-profit detractors.
In 1937, prominent literary figures Laura Riding and Robert Graves penned a famous statement in an Epilogue Essay that’s especially applicable to hospitals today: “the future is not what it used to be.”
For CSO’s, figuring that out is both worrisome and energizing.

Legacy health brands are losing their significance as healthcare consumers place higher value on convenience than reputation. That’s the idea behind a July 1 tweet by Sachin Jain, MD, the CEO of Scan Group and Scan Health Plan.
“We are in an era of the declining significance of big healthcare brands,” he said.
To Dr. Jain, big healthcare brands are the ones commonly known for being the best in a specific specialty or renowned in their region. While many big healthcare brands have high quality performance metrics to hang their clout on, Dr. Jain believes reliance on name alone is problematic.
“There’s been an arrogance by a lot of healthcare organizations that have kind of sold on brand. There’s going to be a reckoning for some of those organizations. My personal view is that the next generation of healthcare consumers is going to be less aligned to think about brands in the same way,” Dr. Jain told Becker’s.
Today’s patients are paying more attention to convenience, digital access and price than reputation. Cost of care, ease of scheduling and accessibility are beating out recognition, Dr. Jain said.
At Scan, Dr. Jain said the Long Beach, Calif.-based Medicare Advantage insurer that serves more than 220,000 members is hyperfocused on staying as human as possible and fulfilling unmet needs for its community.
“Elite healthcare brands are entering this fun phase where they are becoming underdogs. They need to have a chip on their shoulders almost to thrive and perform in this next phase,” Dr. Jain said. “Because I’m not sure payers are necessarily going to continue to pay the same premiums per brand.”