Medicaid is critical to our nation’s healthcare system, providing necessary care for more than 72 million Americans – including our neighbors and friends.
Who it Affects
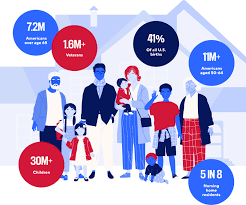
Medicaid covers children, seniors in nursing homes, veterans, people with long-term chronic illnesses, those with mental health issues and working families.
The program helps keep Americans healthy at all stages of life, providing healthcare to families in need — especially as the country continues to recover from record-high inflation.
The Problem
Some policymakers are considering Medicaid cuts that would undermine coverage for countless patients and threaten Americans’ access to comprehensive, 24/7 hospital care.
Medicaid covers health services for patients who otherwise wouldn’t be able to pay for care. Coverage of services is essential for hospitals, and helps ensure all Americans have access to high-quality, 24/7 care, no matter where they live.
Who Medicaid covers
Providing Lifesaving Healthcare Services
Medicaid covers patients with complex and chronic illnesses in need of long-term care, as well as emergency services and prescription coverage.
As the nation faces a growing mental health crisis, Medicaid also ensures millions of Americans — including veterans — have access to mental healthcare and substance abuse services.
Without access to affordable mental healthcare through Medicaid, veterans often lack the long-term support they deserve, and are left to deal with complex health issues years after their service.
In these areas, where primary care providers are few and far between, hospitals become even more vital sites of care — and in some cases, the only sites of care available.
Rural hospitals, already more likely to be at risk of closure, rely on Medicaid funding to stay open and to continue providing lifesaving care to their patients. Nearly 150 rural hospitals have closed or converted since 2010 alone. Further cuts to care would eliminate a lifeline for Americans across the country — with devastating consequences for rural communities.
The Solution
Cuts to Medicaid funding will create irreparable harm for our nation’s most vulnerable communities, including millions of children, veterans, those with chronic illnesses, seniors in nursing homes, and working families. Medicaid helps provide security to these Americans, keeping them healthy at every stage of life.
Congress should vote against efforts to reduce Medicaid funding and instead focus on policies that strengthen access to 24/7 care, rather than take it away.
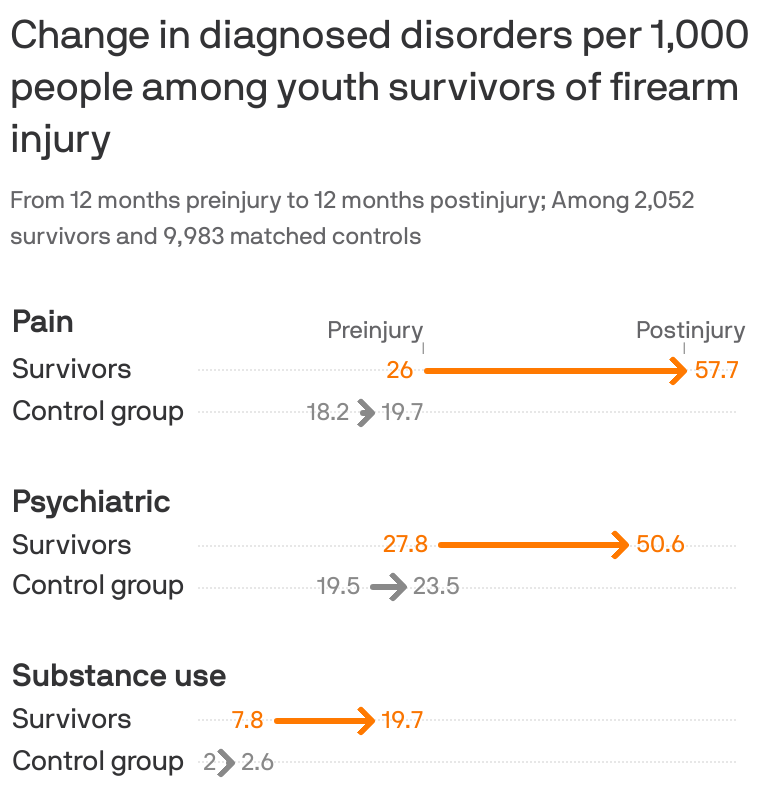
Young survivors of shootings face a litany of physical, psychiatric and substance abuse disorders that can combine to drive up their health costs almost 2,000%, according to new research.
The big picture:
Guns have become the leading cause of death among kids, but many more survive being shot. Their needs offer a rare and detailed look at the cumulative consequences of gun violence and the burden it places on survivors, their families and the health system.
By the numbers:
Using a trove of claims data for employer-sponsored insurance, researchers in Health Affairs compared over 2,000 child and adolescent shooting survivors and 6,000 family members with much larger control groups that did not suffer gun injury between 2007-2021.
In the year after being shot, survivors had a 117% increase in pain disorders including musculoskeletal pain and headaches compared with the control group, with a 293% increase for those more severely wounded.
There was a 68% increase in psychiatric disorders, such as PTSD and mood disorders, with a 321% increase among those with worse injuries.
Substance use disorders rose 144% percent — and cases rose regardless of the severity of the injury.
Emergency room visits for gun injuries among kids doubled during the pandemic, according to separate research published Monday in Pediatrics.
There is also an impact on families’ mental health and even the types of care they got in the aftermath of a child surviving a shooting, researchers found in the Health Affairs study.
Diagnosed psychiatric disorders among mothers and fathers increased by about 30% — and the increases were much larger among parents of children who died.
Mothers had a 75% increase in mental health visits, while other routine care like office visits and lab tests declined slightly for themselves and the siblings of survivors.
That was consistent with a “crowding out” effect when more acute health care needs arise, researchers said.
What they’re saying:
“Our study shines light on the substantial effects incurred not just directly by victims and survivors of gun violence, but indirectly by parents and siblings who, we found, often relinquish their own routine health care to the more acute health needs of the family,” senior study author Chana Sacks, co-director of the MGH Gun Violence Prevention Center, said in a statement.
Survivors’ health care costs also soared 17-fold to nearly $35,000 on average over the course of a year. Two-thirds of the cost was in the first month after being shot, while survivors used more health care across the board — including more visits to doctor’s offices, ER trips, imaging and mental health services.
Insurers covered the vast majority of the care, but families were on hook for about 5% of the cost.
Between the lines:
Researchers looked at claims data for workplace health insurance only, so the results don’t include kids without insurance or those enrolled in Medicaid — a major source of coverage, especially for children of color.
Governor Newsom signs into law four bills expanding access to quality behavioral health care at a ceremony in Sacramento on September 25, 2020. Photo: Paula Ginsborg via YouTube
Governor Gavin Newsom has signed into law four bills intended to improve Californians’ access to mental health and substance use disorder services.
“I pledged to put these critical services within reach of more Californians,” Newsom said in a September 25 statement. “The bills I am signing today will help Californians access the behavioral health services they need to recover.”
The coronavirus pandemic and the resulting economic downturn have persuaded Americans of the importance of behavioral health care services. In the last half of August, a National Council for Behavioral Health poll (PDF) found that the gap has widened considerably between demand for mental health and addiction treatment services and the financial viability of organizations that provide them. Over half of NCBH member organizations reported that in the three months before the survey, more Americans sought their services even as these providers lost, on average, 23% of their annual revenue.
A different survey, conducted in the last week of June, showed that one in four people age 18 to 24 seriously considered suicide in the past 30 days. That troubling finding was published in the Morbidity and Mortality Weekly Report of the US Centers for Disease Control and Prevention.
In California, where the wildfire season got off to an early and destructive start, the converging crises are expected to worsen residents’ mental health. “We are very concerned about the layering of multiple stresses on the people of California,” Jim Kooler, DrPH, assistant deputy director of behavioral health in the California Department of Health Care Services, told Jocelyn Wiener in CalMatters.
Here are the four behavioral health bills that the governor approved:
Strengthening California’s Mental Health Parity Law
Gaps in California’s mental health parity law will be bridged under SB 855 by State Senator Scott Wiener (D-San Francisco). “Current state law requires health plans to cover medically necessary treatment of just nine serious mental illnesses,” Jocelyn Wiener reported in an article about SB 855.
Mental health parity laws “have existed in both state and federal law for years, but insurers have used a complex determination of ‘medical necessity’ to deny care” for mental health issues and substance use disorders, Sigrid Bathen wrote in Capitol Weekly. (A recently published CHCF paper by researchers at Georgetown University’s Center on Health Insurance Reforms assessed California’s progress in enforcing the 2008 federal Mental Health Parity and Addiction Equity Act.)
The new state law requires commercial health plans and insurers outside of Medi-Cal (which is regulated by different standards) to provide full coverage for treatment of all mental health conditions and substance use disorders. This includes treatments for post-traumatic stress disorder, generalized anxiety disorder, and opioid use disorder, Sophia Bollag wrote in the Sacramento Bee. The new law also establishes specific standards for what constitutes medically necessary treatment and criteria for the use of clinical guidelines.
Creating a Certification Process for Peer Support Specialists
Under SB 803 by State Senator Jim Beall (D-San Jose), California will create a system to certify peer support specialists, define their roles, and help to scale up the Medi-Cal workforce.
In 2019, CHCF’s Lisa Aliferis visited Washington State to learn about its innovative statewide peer support program. A certified peer support specialist “identifies as having a significant life-altering mental health [or substance use] challenge and has been in recovery for at least a year,” Aliferis was told by Patti Marshall, the peer support program administrator for the Washington Health Care Authority’s behavioral health and recovery division.
Last year, California had not adopted a similar program — even though the US Centers for Medicare & Medicaid Services issued Medicaid reimbursement guidelines for peer providers in 2007. Now, research has shown that peer support for those with co-occurring mental health and substance use diagnoses prevents rehospitalizations and facilitates their ability to live in the community. “When we say [peer support] saves lives, it’s not hyperbole,” Michelle Cabrera, executive director of the County Behavioral Health Directors Association of California, told Jocelyn Wiener in an article about peer support specialists. “It really is a linchpin in moving people [with mental health and substance use disorder issues] into recovery and stabilizing them long-term.”
Expanding Community Paramedicine
Community paramedicine is a locally designed, community-based, collaborative model of care that leverages the skills of paramedics and emergency medical services (EMS) systems to take advantage of collaborations between EMS and other health care and social service providers. Among other expanded roles, community paramedics are trained to handle behavioral health needs and, depending on the locally designed program, can transport intoxicated patients to sobering centers or mental health treatment, and help frequent 911 callers to obtain behavioral health, medical, housing, and social services. All of these protocols take pressure off hospital emergency departments that traditionally have been the only permitted destinations for patients cared for by EMS agencies.
In 2015, California began testing the model of care through 13 community paramedicine pilot projects across the state. An external evaluation conducted by the Healthforce Center at UCSF found that “community paramedics are collaborating successfully with physicians, nurses, behavioral health professionals, social workers, and outreach workers to fill gaps in the health and social services safety net.”
AB 1544 by Assemblymember Mike Gipson (D-Carson) will expand the pilot projects by authorizing local EMS agencies to develop alternative destination programs.
Making Substance Use Disorder Treatment More Accessible
One-third of adults who receive county services for serious mental illnesses have a co-occurring substance or alcohol use disorder, according to Assemblymember Sharon Quirk-Silva (D-Fullerton). She authored AB 2265, which will authorize counties to use Mental Health Services Act (MHSA) funds — historically limited to mental health services — to treat Californians with co-occurring mental health and substance use disorders.
By removing barriers to using MHSA-funded services for such conditions, AB 2265 will “[increase] access to substance use disorder treatment, [improve] care coordination, and [lead] to a more integrated behavioral health care system,” according to the governor’s office.
The U.S. Department of Justice is charging 10 defendants for an “elaborate” pass-through billing scheme that used small rural hospitals across three states as shells to submit fraudulent claims for laboratory testing to commercial insurers, jacking up reimbursement.
The defendants, including hospital executives, lab owners and recruiters, billed private payers roughly $1.4 billion from November 2015 to February 2018 for pricey lab testing, reaping $400 million.
The four rural hospitals used in the scheme are: Cambellton-Graceville Hospital, a 25-bed rural facility in Florida; Regional General Hospital of Williston, a 40-bed hospital in Florida; Chestatee Regional Hospital, a 49-bed facility in Georgia; and Putnam County Memorial Hospital, a 25-bed hospital in Missouri. Only Putnam emerged from the scheme relatively unscathed: Chestatee was sold to a health system that plans to replace it with a newer facility, Cambellton-Graceville closed in 2017 and RGH of Williston was sold for $100 to an accounting firm earlier this month.
Dive Insight:
The indictment, filed in the Middle District of Florida and unsealed Monday, alleges the 10 defendants, using management companies they owned, would take over rural hospitals often struggling financially. They would then bill commercial payers for millions of dollars for pricey urine analysis drug tests and blood tests through the rural hospitals, though the tests were normally conducted at outside labs, and launder the money to hide their trail and distribute proceeds.
The rural hospitals had negotiated rates with commercial insurers for higher reimbursement for tests than if they’d been run at an outside labs, so the facilities were used as a shell for fraudulent billing for often medically unnecessary tests, the indictment alleges.
The defendants, aged 34 to 60, would get urine and other samples by paying kickbacks to recruiters and healthcare providers, like sober homes and substance abuse treatment centers.
Screening urine tests, to determine the presence or absence of a substance in a patient’s system, is generally inexpensive and simple — it can be done at a substance abuse facility, a doctor’s office or a lab. But confirmatory tests, to identify concentration of a drug, are more precise and sensitive and have to be done at a sophisticated lab.
As such they’re more expensive and are typically reimbursed at higher rates than screening urine tests. None of the rural hospitals had the capacity to conduct confirmatory tests, or blood tests, on a large scale, but frequently billed in-network insurers, including CVS Health-owned Aetna, Florida Blue and Blue Cross Blue Shield of Georgia, for the service from 2015 to 2018, the indictment says.
Rural hospitals are facing unprecedented financial stress amid the pandemic, but have been fighting to keep their doors open for years against shrinking reimbursement and lowering patient volume. That can give bad actors an opportunity to come in and assume control.
One of the defendants, Jorge Perez, 60, owns a Miami-based hospital operator called Empower, which has seen many of its facilities fail after insurers refused to pay for suspect billing. Half of rural hospital bankruptcies last year were affiliated with Empower, which controlled 18 hospitals across eight states at the height of the operation. Over the past two years, 12 of the hospitals have declared bankruptcy. Eight have closed, leaving their rural communities without healthcare and a source of jobs.
“Schemes that exploit rural hospitals are particularly egregious as they can undermine access to care in underserved communities,” Thomas South, a deputy assistant inspector general in the Office of Personnel Management Office of Inspector General, said in a statement.
Increases in Worry Over Health Care Costs and Skipping/ Postponing Treatment Due to Cost Over the Last Year
PERCENTAGE WHO SAY THEY ARE VERY OR SOMEWHAT WORRIED ABOUT…
The California Health Care Foundation (CHCF) released earlier today its second annual California Health Policy Survey. It provides insights into Californians’ experiences and attitudes about health coverage, health care costs, access to care, mental health, substance use treatment, the health care workforce, and homelessness. The poll was done in conjunction with SSRS, a national survey research firm.
Mental Health Ranks #1
Among health issues, Californians’ top priority is ensuring people with mental health problems can get treatment (52% say it is “extremely important”). Next is lowering the price of prescription drugs (47% extremely important), followed by making sure all Californians have health insurance (46% extremely important).
As it did last year, access to mental health care ranks in the top two health priorities for Democrats, Republicans, and independents alike.
“For too long, the health care system has treated mental health concerns as a second-tier issue,” said CHCF President and CEO Sandra R. Hernández, MD. “For two years in a row, the people of California are sending a clear message that this is the top health care issue they want addressed.”
The poll also found that large numbers of Californians who need mental health care struggle to get it. Among those with insurance who tried to make an appointment for mental health care in the past 12 months, nearly half (48%) found it very or somewhat difficult to find a provider who took their insurance. Over half (52%) of those who tried to make an appointment (with or without insurance) believe they waited longer than was reasonable to get one.
More Are Worried about the Cost of Health Care
Californians rank health care affordability as a top priority among a range of public challenges presented in the poll—with 84% of respondents citing it as extremely or very important. Support for making health care more affordable cut across party identification, race, and income lines.
Compared to last year, more Californians are worried about paying for a variety of health care costs. Just over half of Californians (51%) have skipped or postponed physical or mental health care due to cost — up from 44% last year. Of those who took such a step, 42% said it made their condition worse.