https://www.thefiscaltimes.com/2017/08/10/Taxpayers-Will-Pay-Price-Uncertainty-Over-Obamacare-2018

The health insurance industry remains in the throes of a largely unnecessary crisis of confidence, according to an analysis released by the Kaiser Family Foundation on Thursday.
With the open enrollment period approaching for Obamacare insurance plans sold through state exchanges, Kaiser Foundation experts were able to analyze the proposals for 2018 submitted by insurance companies to 20 states and the District of Columbia — the only places where enough information is made public to allow an assessment of what health care costs would look like for an average policyholder under the insurers’ requested rate structures.
“Insurers attempting to price their plans and determine which states and counties they will service next year face a great deal of uncertainty,” the authors wrote. “They must soon sign contracts locking in their premiums for the entire year of 2018, yet Congress or the Administration could make significant changes in the coming months to the law – or its implementation – that could lead to significant losses if companies have not appropriately priced for these changes. Insurers vary in the assumptions they make regarding the individual mandate and cost-sharing subsidies and the degree to which they are factoring this uncertainty into their rate requests.”
What that means for consumers is a bit of a mixed bag. Almost all insurers are seeking rate increases, with some approaching a 50 percent jump. But the actual impact on consumers varies depending on where they buy their insurance and how much money they earn. One thing is for sure, though: The federal government, and therefore taxpayers, will be on the hook for larger subsidy payments.
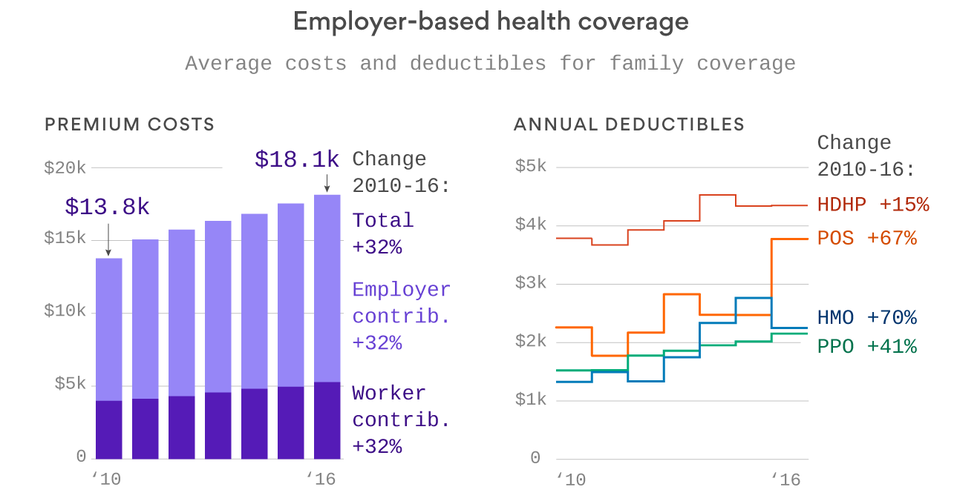
Because the majority of Americans obtain health insurance through an employer-sponsored plan or from federal programs like Medicare and Medicaid, the impact of the premium increases of exchange-based policies will mean little to a large element of the population.
Of those who buy insurance on the exchanges, the overwhelming majority receive tax credits meant to keep their premium payments to a specific fraction of their annual income. The remaining 16 percent, depending on their income, receive either a smaller subsidy or no subsidy at all. It is these people who, if they live in some of the regions facing large premium increases, who will be hurt the most.
The Kaiser study gathered information from the largest city in each of the 20 states plus the District of Columbia. (Benchmark levels for tax credits are based on the second-cheapest Silver Level plan available in the largest city in a state.) They estimated the change in costs for a 40-year-old non-smoker earning $30,000 a year.
In only one state was the annual premium expected to fall in 2018: Rhode Island, which anticipates a 5 percent drop. Vermont’s premiums will remain static in 2018 if the data holds. The other 19 states can all expect increases, from a modest 3 percent in Michigan to a whopping 49 percent in Delaware.
The average increase in the data collected by Kaiser is 17 percent.
However, none of those costs would be passed on to the consumer making $30,000 a year. In fact, because of adjustments to the tax credit, he could expect to see monthly costs fall by 3 percent, to $201, next year, regardless of what premium levels do where he lives.
But somebody has to pay when premiums go up, and if it isn’t the consumer, it’s the Treasury and by extension, the taxpayer.
The change in premium payments required to keep that 40-year-old’s health insurance premium at $201 per month will increase very sharply in many states, depending greatly on how far from the premium cap a silver plan was in 2017.
In Washington State, according to Kaiser, the premium tax credit would increase 239 percent, from $31 per month to $105. In New Mexico, it would jump 183 percent, from $51 to $144. In Rhode Island it would fall 13 percent, while in Vermont it would rise a modest 2 percent. On average, though, the amount of premium payment picked up by the federal government will increase by about 63 percent in the states reviewed by Kaiser.
Perversely, as Kaiser points out, that fiscal wound is largely self-inflicted. While it is impossible to gauge just how much of this year’s rate increases are attributable to insurers being nervous about whether the federal government would slash support payments in the middle of the 2018 policy year, the answer is surely non-trivial, and the dollars are coming out of the pockets of taxpayers.