Policymakers and advocates often promote drug price transparency to lower costs and improve equity. While transparency is an important first step toward accountability and informed public budgeting, it does not guarantee affordable prices or fair access to medicines.
Transparency Has Some Benefits
Drug price transparency helps show how and why medicines cost what they do along the supply chain (i.e., from the manufacturer to the pharmacy), which makes it easier to identify where costs can be reduced or better regulated. By making this information public, transparency allows patients, payers, and policymakers to make more informed decisions and encourage manufacturers to prices drugs more fairly. Ultimately, it supports a fairer system where patients can better afford and obtain the treatments they need, improving access to care.
States with Drug Transparency Laws
While federal policy to improve price transparency is lacking, the states have moved to make things clearer for patients and payers. Vermont was the first U.S. state to enact a drug price transparency law in 2016. Since then, many others have followed suit. At least 14 states have passed some version of transparency legislation, though the details and their enforcement of these laws differ widely.
For example, only Vermont and Maine require drug companies or insurers to disclose the actual prices paid after discounts (called the “net price”). Alternately, Oregon and Nevada require drug manufacturers to publicly report their profit to state government agencies. And Connecticut, Louisiana, and Nevada mandate pharmacy benefit managers (PBMs) to report the total rebates they receive, but not the amounts for each specific drug. Despite these efforts, no state has yet achieved full transparency across the entire drug supply chain.
Transparency is Not Enough
Even with clear pricing, Americans still pay about 2.6 times more for prescription drugs than people in other wealthy countries. Early evidence suggests that these laws have done little to curb drug prices. To date, only four states – California, Maine, Minnesota, and Oregon – have published analyses of their own laws. These reports share common concerns: difficulty tracking pricing across the supply chain and uncertainty about whether state agencies have the authority (or the will) to act when data is incomplete or unreliable.
Most transparency laws fall short on requiring detailed cost or profit data, focusing instead on broad price trends. As a result, this narrow scope makes it difficult to identify the exact drivers of high drug prices. Even when transparency discourages manufacturers from raising prices, these policies do not directly control pricing or define what constitutes an ‘unjustified’ price increase. Manufacturers can simply adjust by setting higher launch prices or implementing smaller, more frequent increases to stay below reporting thresholds. Still, the result is a system where drug costs can vary by as much as $719 for the same 30-day prescription even when prices are publicly listed.
What can also be done?
Creating a consistent national framework could replace the current patchwork of state laws and improve oversight of how drugs are priced. For example, the Drug Price Transparency in Medicaid Act (H.R. 2450) could do just that: it would standardize reporting requirements and reveal how drug prices are set, rebated, and reimbursed. But transparency alone can’t lower costs—it only shows the problem.
To make transparency meaningful, policymakers must address the underlying contracts and incentives that drive high prices.
Hidden rebate deals and opaque pricing structures between PBMs and drugmakers often inflate costs and limit patients from seeing savings. Transparency legislation should also be paired with value-based pricing that links payments to clinical benefits. Federal programs like the Medicare Drug Negotiation Program provide additional leverage, but broader reforms are needed to reach the commercial market (i.e., where most Americans get their prescription drugs and still face high prices).
Still, transparency can have downsides, especially globally. Fully public drug prices could push companies to stop offering lower prices in low- and middle-income countries. To avoid cross-country comparisons, they could raise prices across the board, making medicines less affordable where they’re needed most. To make transparency more equitable, policymakers should combine disclosure with protections that preserve affordability worldwide.
Conclusion
In short, transparency is necessary but an incomplete fix for America’s drug pricing system. Simply shining a light on how prices are set isn’t enough. Policymakers need to be paired with other reforms, such as removing the incentives that encourage high prices, holding PBMs and manufacturers accountable, extending the negotiating power beyond Medicare, and protecting prescription drug access both at home and abroad. Without these other steps, transparency laws risk highlighting unfairness without actually improving it.
Sweeping changes to Medicaid and the Affordable Care Act are combining with rising health costs to make 2026 a high-stakes year for hospital operators.
Why it matters:
While major health systems like HCA are likely to weather the worst, some safety net providers and facilities on tight margins could close or scale back services as uncompensated care costs mount and uncertainty around future policies swirls.
“We took a big hit in 2025,” said Beth Feldpush, senior vice president of policy and advocacy at America’s Essential Hospitals.
“I don’t think that the field can absorb any further hits without us really seeing a crisis.”
State of play:
Last year’s GOP tax-and-spending law will decrease federal Medicaid funding by nearly $1 trillion over the next decade, translating into millions more uninsured, lower reimbursements and higher costs for hospitals.
The Trump administration is also considering big changes to the way Medicare pays for outpatient services that could reduce hospital spending by nearly $11 billion over the next decade, including paying less for chemotherapy.
Hospitals have the rest of this year to boost their balance sheets, invest in technology including AI, and even consider merger plans before the biggest changes take effect in 2027, Fitch Ratings wrote in its annual outlook for the nonprofit hospital sector. The financial outlook remains stable for the sector overall next year, the report predicts.
“People are already very proactively looking at those out years and saying, if that’s the worst-case scenario that I’ve got to deal with, what can I do today to make that impact less,” said Kevin Holloran, a senior director at Fitch.
Threat level:
Hospitals in some instances have started closing unprofitable services like maternity care and behavioral health care in the face of financial pressures.
More than 300 rural hospitals are at immediate risk of closing their operations entirely, according to a December report.
Safety net providers also are going to court to fight an administration effort to make them pay full price for medicines they currently get at a steep discount and reimburse them later if they’re found to qualify under the government’s 340B discount drug program.
“Those hospitals that have been underperforming … they are going to continue to struggle,” said Erik Swanson, managing director at consulting firm Kaufman Hall. “Those who are doing really, really well may continue to see growth in their performance.”
Private equity firms will likely continue buying up and building new businesses in outpatient service areas like ambulatory surgery, labs and imaging, he said.
“Hospitals and health systems should continue to expect quite a bit of challenge and disruption in those spaces.”
Congress still could extend the industry some lifelines, though any effort to delay or roll back some of the biggest Medicaid cuts face tough odds this year.
Sen. Josh Hawley (R-Mo.) introduced a bill to repeal parts of the GOP budget law that would slash hospitals’ Medicaid dollars.
Lawmakers are debating whether to renew enhanced ACA subsidies that expired at the end of 2025 and could result in millions more uninsured patients, but that effort would also have to overcome significant GOP opposition.
“Our job is to make sure that we create a predicate that, as these provisions come online, they may very well need to be revisited,” said Stacey Hughes, the American Hospital Association’s executive vice president for government relations and public policy.
What’s ahead:
Beyond policy changes, hospitals also are dealing with inflationary pressures, including rising medical supply costs, and administrative overhead from insurer pre-treatment reviews.
Those trying to pad their margins may ramp up their use of artificial intelligence to code patient visits in a way that increases reimbursements from public and private payers, Raymond James managing director Chris Meekins wrote in an analyst note.
While hospitals have historically been able to navigate big policy challenges, if things don’t go their way, it could turn into a “tornado of trouble,” Meekins wrote.
Congressional negotiators are working to revive the health care deal that was dropped from a government spending package in late 2024 — but the odds of resurrecting enhanced Obamacare subsidies as part of the effort appear dire.
Why it matters:
Long-stalled bipartisan priorities that are in play include an overhaul of pharmacy benefit manager practices, as well as a measure that would place more controls on Medicare outpatient spending.
They’d likely be combined with a renewal of health programs due to expire Jan. 30, including certain Medicare telehealth flexibilities and funding for community health centers.
Driving the news:
Leadership and health committees in both parties have quietly swapped offers on a package over the past week while attention was primarily focused on the fight over expired Affordable Care Act tax credits.
Democrats included a three-year extension of the ACA subsidies in their latest offer knowing that GOP leadership is likely to reject it, sources said.
That would still leave intact most of the health care deal that was destined to ride on a government funding package before it was scuttled at the last minute by Elon Musk and then President-elect Donald Trump.
What we’re hearing:
Asked about the likelihood of a health package without the ACA subsidies, Senate Finance Committee Ranking Member Ron Wyden (D-Ore.) pointed to the overwhelming 26-0 vote in his committee for the PBM overhaul in 2023.
“I’m not going to negotiate with myself but the reality is I think a 26-0 vote in the Senate … it’s like unheard of,” Wyden told Axios, adding he is “feeling upbeat” about getting the PBM bill over the finish line.
Senate Finance Chairman Mike Crapo (R-Idaho) also told Axios he is “feeling optimistic” about the PBM bill, saying there is “broad support here and at the White House.”
That measure includes provisions like “delinking” the price of a drug from PBM compensation in Medicare Part D.
The prospective package would also include a measure that would require off-campus hospital outpatient departments to have a unique identifier number.
It’s a cost-saving measure designed to prevent outpatient departments from billing payers at higher amounts associated with full-service hospitals.
But it would stop short of a full-scale, more sweeping change known as site-neutral payments that would more closely align Medicare payments to hospital outpatient departments with freestanding physician offices.
The intrigue:
The outlook for renewing enhanced ACA subsidies, which help millions of Americans afford their premiums, is much bleaker.
While a separate bipartisan group of senators continues to meet in search of a compromise, a key negotiator, Sen. Bernie Moreno (R-Ohio), told reporters on Tuesday that a release of a proposal would be punted until after next week’s Senate recess.
Even if the group can release a proposal — which would include GOP-backed changes like eliminating $0 premium plans — there is deep skepticism in both parties that it can actually pass.
Many Republicans are opposed to any kind of ACA subsidy extension, saying it is wasteful spending that benefits insurance companies.
Top Democrats are pushing for a clean subsidy extension without GOP-backed changes and blasting Republicans for blocking it, in what could be a preview of midterm campaign messaging.
Between the lines:
There still are significant divisions over whether to include new limits on the ACA funding going to plans that cover abortions.
The bipartisan group has discussed a potential compromise that would increase audits and levy penalties on insurance companies that don’t comply with existing rules requiring them to segregate taxpayer money from paying for abortions.
The idea immediately drew fire from the anti-abortion group Susan B. Anthony Pro-Life America, and many Senate Republicans think it does not go far enough.
The bottom line:
There still could be an election-year health deal — just don’t expect it to address ACA subsidies.
The 119th Congress headed into the holidays no doubt looking forward to quality time with their loved ones and a fat goose on the dinner table—or whatever the privileged stewards of the People eat at Christmas—with what seemed like little concern for the mess and panic they left behind. Messy panic like what the nearly 25 million Americans getting their health insurance through the ACA are facing as their monthly premiums increase at astronomical rates. (Assuming they stick with the devil they know.) Now they’re back, surely refreshed with all engines blazing on their New Year’s resolution to make health care more affordable. It is, after all, what the People want.
But while what to do with the ACA gets fought over like an unloved middle child in a divorce, another form of health care dupery will continue to operate like a mob-run casino.
Many of us navigate our health care thinking that if we can land a full-time job at a company offering benefits, we—and our families—will be covered for most physical and mental health issues without complete disruption to our financial health. And in many cases, sure, that tracks. What we’re not seeing is the financial fleecing that those companies are experiencing at the hands of third-party administrators (TPAs). What’s more is that the companies aren’t seeing it either. And that’s not a bug. It’s a feature.
An employer has options when deciding how to provide health benefits to its employees. One is to contract directly with an insurance company and pay fixed premiums. Another is to self-insure. Self-insured employers pay for all enrolled member benefits and claims directly from their own funds instead of paying those aforementioned fixed premiums. It’s an attractive option for employers because even though the company assumes the financial risk, it offers control over costs, plan design and claims-related data, all of which can help the company run more efficiently and with greater fiduciary understanding. They’re popular, too, with approximately 57% of private sector workers enrolled in these self-funded plans, according to KFF. To facilitate the company’s coverage, employers contract with a TPA to broker plan details, manage claims, pay providers, assist plan members and ensure the benefit program remains compliant with state and federal regulations.
This is theoretical.
TPAs say they’re looking after the company, but they don’t. They’re looking after themselves and their parent companies. And just who are these parents? Blue Cross Blue Shield, UnitedHealthcare, Cigna, and Aetna. Or, as they’re collectively called, the BUCAs. The usual suspects in the web of health care greed and deception.
It’s like taking a pregnancy test then being told the results can’t be shared with you because the results belong to the stick with the pee on it.
Skimming the till the TPA way
The Employee Retirement Income Security Act (ERISA) was passed in 1974 to protect patients by requiring transparency, fiduciary standards and fair claims processes for employer-sponsored health (and retirement) plans. TPAs have found clever ways to avoid ERISA accountability in the way they structure the administrative services agreements (ASAs) they sign with employers. One is by enlisting gag clauses in the ASAs to protect TPAs from showing their work to the employer, which obviously defeats the whole purpose of choosing to self-fund and have more oversight of how their money is being spent. The Consolidated Appropriation Act of 2021 prevented these gag clauses. But TPAs are nimble and clever, and when pressed to offer up information, such as any of the data related to claims managed and paid, TPAs argue they don’t have to because the data is proprietary. It’s an odd argument to make. It’s the employer’s money being spent and their employees being treated. It’s like taking a pregnancy test then being told the results can’t be shared with you because the results belong to the stick with the pee on it.
Not sharing crucial plan information with the employer is one thing, tacking on fees under the guise of good stewardship is another. Like the overpayment recoupment fee. Here’s how this could play out:
The TPA discovers a provider was overpaid due to an error made by duplicating payments, incorrect coding, or any other administrative whoopsie
The TPA recoups the overpaid amount, say, $5,000, then takes a percentage of the recouped money—typically 30% — as a fee for cleaning up the mess they made
They recover the extra $5,000 the employer paid, the employer gets back $3,500 while the TPA banks $1,500
This means that the employer paid a total of $6,500 on a $5,000 claim, making carelessness an incentive for TPAs
Shared savings fees are put in play when someone enrolled in a health plan uses an out-of-network (OON) provider. As we know, OON claims are often hefty bills. Seemingly, in good faith, the TPA will negotiate a discounted rate with the provider. It could look like this:
The OON provider bills the employer $50,000
The TPA negotiates the provider down to $20,000 then takes their shared savings fee out of the $30,000 savings
Again, this fee rate is often around 30%. That puts $9,000 in the TPA’s pocket
The TPA is incentivized here to push members to go OON, and why not? A $30,000 savings sounds real good. But employers aren’t getting the opportunity to weigh in on these negotiations because they are, you know, “proprietary.”
Putting it honestly, TPAs are the neighborhood mafioso.
TPAs also have skip lists, which are providers they do not apply oversight to when looking for billing errors, which they rarely do anyway, but these lists make it more, um, official. In May 2024, W.W. Grainger, Inc., a product distribution company with 20,000-plus employees (and their family members) filed a lawsuit against Aetna claiming Aetna took money paid by Grainger intended to pay for claims, paying providers only a portion of the money, keeping the rest for itself. The suit claims, “Aetna did not use the fraud prevention techniques it regularly employs when administrating claims for its own fully insured plans. Aetna never refunded or credited the difference to the Plans.” The suit further states, “Aetna also engaged in active deception to conceal its breaches of its duties to the Plans. Aetna prevented Grainger from discovering Aetna’s improper conduct, including by limiting audit rights, providing false or inaccurate claims reports, and preventing Grainger from obtaining or accessing data about the actual financial transactions between Aetna and the health care providers.”
Many other similar suits have been filed against TPAs but are either dismissed or held up in the court’s web of confusion and legal ballet.
The uphill battle for Capitol Hill
Putting it kindly, TPAs are middlemen sold as a way to lighten the administrative load for a company. Putting it honestly, TPAs are the neighborhood mafioso. Imagine with me, a neighborhood dry cleaner… One day, a wise guy walks in and tells the owner that he needs to pay 30% of the profits each week in exchange for protection. “Protection from what?” the dry cleaner asks. “From, you know, trouble. And you don’t want any trouble. Not at a nice establishment such as this.” There’s no way the dry cleaner can win. Either pay the guy or risk going to open the door one morning only to discover the door is the only thing left standing after the place mysteriously burned down overnight.
A bill introduced last year by Senators John Hickenlooper (D-Colo.) and Roger Marshall (R-Kan.) called the Patients Deserve Price Tags Act (PDPTA) is designed to make health costs more transparent and provide employers with better tools to hold TPAs accountable as well as to strengthen and expand existing transparency measures like requiring TPAs to disclose compensation practices truthfully, completely and upfront instead of leaving the burden to employers. The bill would make void any provisions in ASAs that support limiting access to employers. Furthermore, it would empower the Department of Labor (DOL) to fine TPAs $10,000 for each day a violation continues. TPAs would also be required to make quarterly reports detailing pricing and compensation practices and report the total they have been paid in rebates, fees, discounts and other forms of payment. Failure to provide this information would be a violation of ERISA, and the DOL could fine the TPA $100,000 per day until the report is provided.
But will it pass? And if so, how much of it will get hacked away thanks to BUCA lobbying efforts? And is another bill even the answer? Legislation has been passed to defend against these practices, and yet, they persist. Apparently, doing the same thing over and over again and expecting a different result is not insanity, but progress for Congress. Another bill may just add to the complexity of things. And the big question remains: Will it save self-insured employers money? Doubtful. TPAs can simply raise the price of doing business. That’s BUCA forecasting 101—everything can always be more expensive.
Perhaps Washington needs to begin thinking of TPAs and BUCAs like the organized criminals they are and bring a RICO case against them.
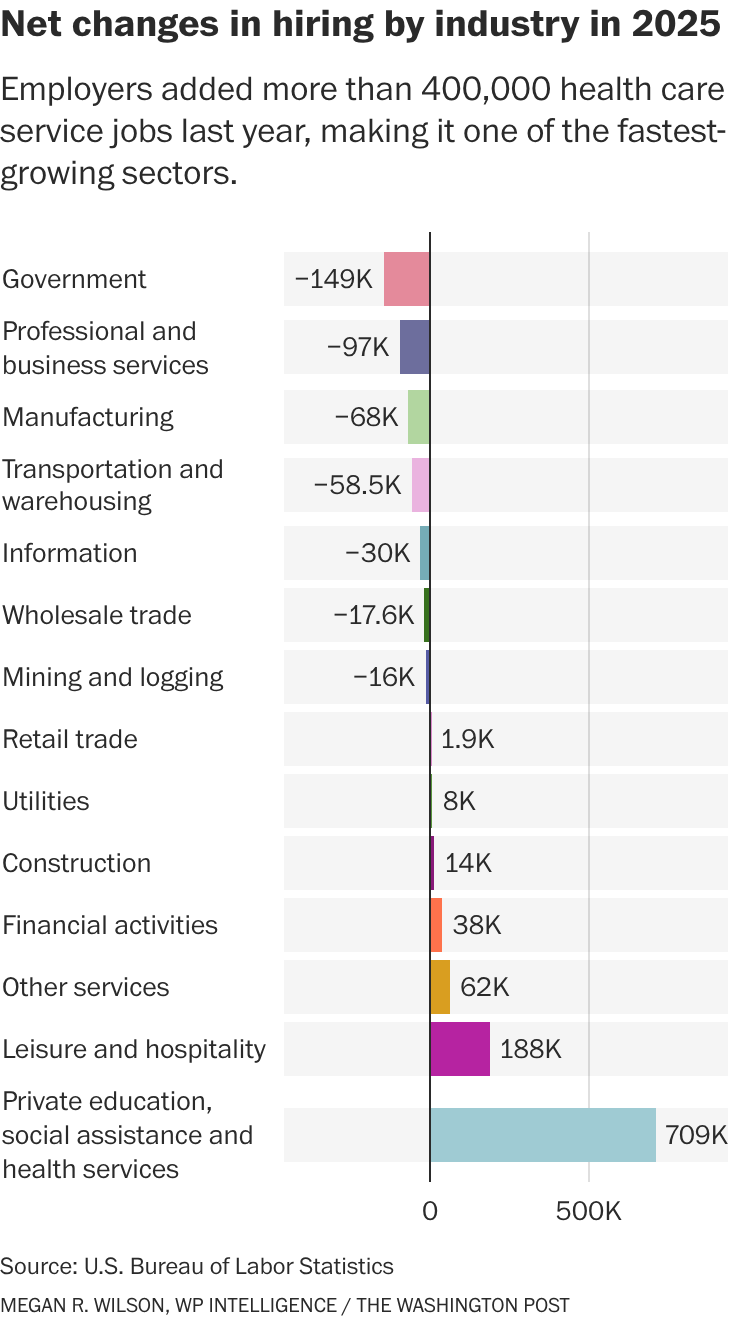
The health services industry was once again a bright spot in the economic data in today’s jobs report, which otherwise landed with a thud and capped off the weakest year for overall hiring since the pandemic.
The growth underscores how much health care employers are propping up the overall labor market — accounting for most of the gains, both in sheer numbers and percentage growth.
“The fundamental reason why health care employment continues to grow so strongly is that the aging population continues to boost demand for health care services,” said Jed Kolko, a senior fellow at the Peterson Institute for International Economics. “The population will continue to age, so that fundamental driver of demand continues.
”Behind the numbers: Although economists expect the health industry to continue expanding, they note that 2025 represented a slowdown from the previous year. Although many factors are at play, multiple analysts said the Trump administration’s restrictive immigration policies may be to blame. More on that later.
It’s not a huge surprise that people working in places such as hospitals, dentists’ offices and nursing homes represent the largest growth in hiring: Health care makes up about 18 percent of the overall U.S. economy — which means that $1 out of every $5 that Americans spend goes to health care. Advertisement
But this also highlights how health services hiring is keeping broader U.S. employment from sliding — even as other industries cool. Patients and providers alike are bracing for cost and workforce pressures in 2026.
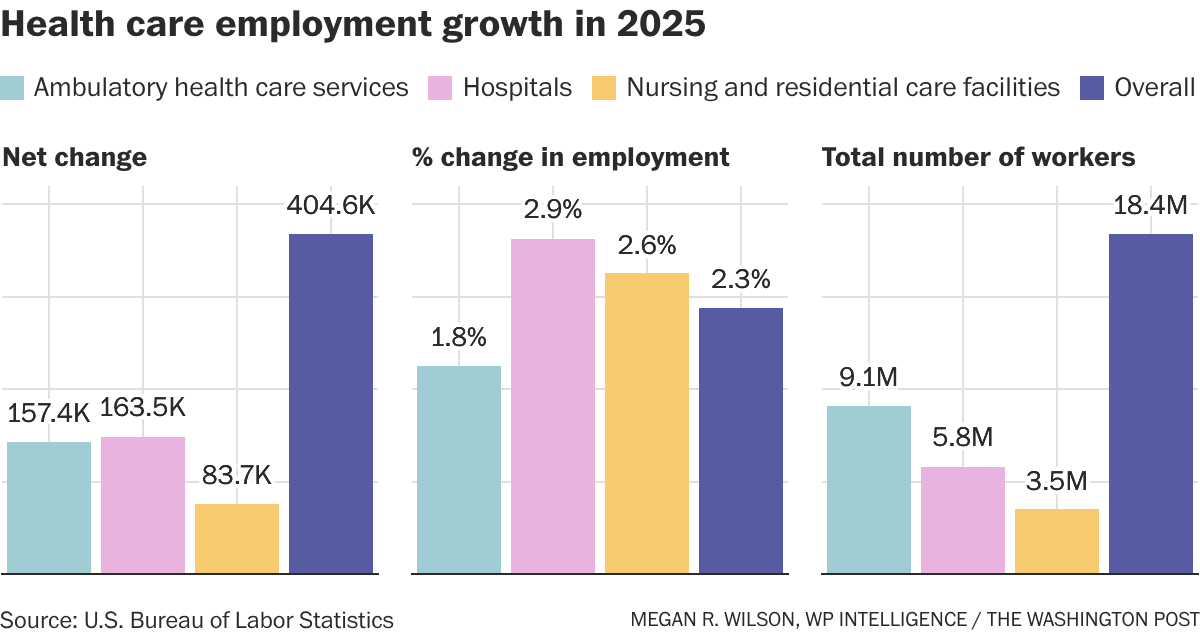
Dive in: Although the number of people working in health services increased by more than 404,000 in 2025, it’s still a slowdown from the level of growth the sector saw the year before. In 2025, the health industry added about 34,000 workers per month, according to federal data, compared to an average monthly gain of 56,000 health jobs in 2024. This included people working in hospitals, residential care facilities or nursing homes, diagnostic labs, and for home health providers .
Here’s how it breaks down:
Hospitals represented the highest employment growth rate — 2.9 percent — in the health services industry, followed by jobs at nursing homes and residential care facilities, at 2.5 percent.
“We’re getting older and sicker. And, on top of that, we’re getting older and sicker in a way [where] we don’t have young people around to take care of the older, sicker people, right?” said Richard Frank, economic studies senior fellow at Brookings and director of its Center on Health Policy. Advertisement
“So what used to be long-term care delivered by family members when we had four or five kids per household, that looks very different today,” Frank said. “You’re going to have to pay people to do that work.
”While economists anticipate health care hiring to continue to grow — in part for that very reason — there two major policy shifts loom as a dark cloud over the industry and may impact the health services workforce.—
Immigration: Providers around the country have said that the Trump administration’s approach to immigration has hampered their ability to hire people. The administration has been cracking down on legal immigration as well as on people who have come to the U.S. illegally. Meanwhile, immigrants make up 28 percent of the long-term care workforce and 32 percent of home care workers, according to KFF.—
Medicaid cuts: The Republicans’ tax-and-domestic-policy law enacted last July is expected to slash nearly $1 trillion from the Medicaid program for low-income Americans. Researchers estimate that this will hammer the balance sheets of many hospitals, which are likely to see an influx in patients seeking care but are unable to pay for it. Hospitals and health clinics are already shutting down or laying off workers across the country. Although the Medicaid policy changes — which won’t fully kick in for years — aren’t the only reason for the closures, it shows how vulnerable many providers already are.
Other changes, including the proposed cuts to the National Institutes of Health, could trickle down to communities with research hospitals and ultimately impact the labor market, according to research from the Brookings Institution. New Medicare payment policies that aim to shift care away from expensive hospital services and toward primary care could also have an impact, although it likely won’t be large enough to show up in the data, I’m told.
However: Some states are working to offset some of the administration’s immigration policy changes or health program cuts, which could make it hard to evaluate their impact in the next round of employment data. “There are a lot of … crosswinds blowing in the aggregate that might cover up” the overall impact of these policies,” said Frank.
Other data: Employment in what the government calls “individual and family services” — listed under the “social assistance” category — increased by more than 289,000 people in 2025, representing a nearly 9 percent increase over 2024. These jobs include personal care aides, social workers and substance abuse counselors.
Health care costs hurt Californians every day. Millions can’t afford the care they need. More than half of all Californians skip or delay getting care because it costs too much.
How did we get here?
Health care is too expensive for people in large part because underlying costs in our health care system have grown unchecked for decades. Underlying costs are the “base ingredients” that determine how expensive health care is. Think of things like hospital operating costs, prescription drug prices, and doctor fees — when these costs go up year after year, they get passed on to patients through higher premiums, bigger deductibles, and larger medical bills.
The solution to the affordability crisis isn’t to slash health care spending across the board — that often makes things worse for patients. Instead, we need to be smart about cutting that 25% that doesn’t provide any value for patients.
Some of that rising cost has produced things we actually want, such as breakthrough treatments that save lives, cutting-edge medical equipment, or hospitals retrofitted to withstand earthquakes.
The solution to the affordability crisis isn’t to slash health care spending across the board — that often makes things worse for patients. Instead, we need to be smart about cutting that 25% that doesn’t provide any value for patients. Sometimes that might actually mean spending more money upfront, like making sure everyone can see a primary care doctor, to save money down the road by keeping people healthier.
This work is challenging, but it’s critical. Millions already can’t afford health care. If Californians’ health care costs keep rising the way they have been, even more families will be left behind.
Unchecked growth in the underlying costs of our health care system has driven total health care spending — from families, governments, employers and others combined — to more than triple since 2000, far outpacing inflation, economic growth, and wages.
Here are just a few key examples of the impact on California families:
Health insurance is increasingly becoming unaffordable for California families.
38% of all Californians report carrying medical debt. For Californians with low incomes, that rises to 52%.
Overview of the 3 Reasons
1. Administrative Waste
Health care requires some office work — doctors and hospitals have to schedule appointments, send bills, and keep records. But in the U.S., we spend way too much time and money on administrative tasks, which does nothing to make care better for patients.
Why Does This Happen?
Our health care system is complex. Different hospitals, doctors, and insurance companies often all use different computer systems for clinical data, billing, and administrative tasks. They can’t easily share information with each other. This means:
Staff in different parts of the system spend extra time entering the same information over and over;
Insurance companies and hospitals have to hire more people just to handle paperwork; and
Simple tasks become complicated and expensive.
How Much Money Gets Wasted?
Researchers in 2020 estimated that administrative waste cost the California health care system nearly $21 billion a year, making it the number one source of health care spending that doesn’t do anything to help patients or improve care.
How This Hurts Patients
Administrative waste doesn’t just cost money. It also hurts patient care:
Doctors spend less time with patients because they’re busy with forms.
Patients wait longer to get care.
Doctors have to call insurance companies over and over to find out what’s covered, and this can delay treatment when people need help.
Health care spending depends on two things: 1) how much care people get and 2) the prices that are charged for that care. In California, we have a big problem with pricing.
Same Care, Very Different Prices
The same medical procedure can cost wildly different amounts depending on where you go. For example, a knee replacement might cost $50,000 at one hospital and $70,000 at another. This happens even when both hospitals provide the same quality of care. In other words, the more expensive hospital is not necessarily better.
Lack of Competition Drives Prices Up and Hurts Patients
In many areas, there isn’t enough competition among health care organizations. For example, big hospital systems are buying up smaller hospitals. In some areas, there’s only one major hospital system left. Likewise, a few large insurance companies control most of the market. In some areas, one insurance company dominates.
When hospitals and insurance companies don’t have to compete:
Prices can go up without any improvement in care quality.
Patients have fewer choices about where to get care.
Families pay more for the same treatment.
Some areas become “take it or leave it” markets.
This creates unfair contracts where the biggest companies can demand high prices because patients have nowhere else to go.
When doctors find health problems early, they’re much easier and cheaper to treat. For example:
Regular cancer screenings can find problems before they become serious cancer.
Checking on people with heart problems can prevent expensive hospital stays.
Treating diabetes early prevents costly complications later.
Too often, though, people don’t get these early checks because there might not be a primary care doctor that can see them when they need it. By the time they see a doctor, their problems are much more serious and expensive to fix.
We Don’t Spend Enough on Prevention
Most prevention happens when you visit your primary care doctor for regular check-ups and basic care. But the U.S. has a big problem: We spend only 5 cents of every health care dollar on primary care, while other wealthy countries spend three times that amount.
California research shows that when provider organizations spend more money on primary care:
Patients get better quality care.
People are happier with their treatment.
Fewer people end up in the emergency room.
Fewer people need expensive hospital stays.
Overall health care costs go down.
We could save billions of dollars by helping people stay healthy instead of waiting until they get really sick. It’s like fixing a small leak in your roof instead of waiting until your whole ceiling falls down.
The good news is that we can fix these problems. California is working on several smart solutions right now.
The Office of Health Care Affordability
Created in In 2022, the Office of Health Care Affordability (OHCA) aims to break the cycle of the last decades and make sure that underlying costs in the health care system don’t continue to spiral out of control year over year.
Cost Growth Targets
In 2024, OHCA set an important new target: Total spending by health care’s major players — like hospitals, insurance companies, and large medical groups — can’t increase by more than 3% each year. That’s roughly how much a typical California family’s income grows every year. The target will be implemented in phases over the next several years.
This creates a powerful new incentive for these health care organizations to manage their underlying costs, rather than allowing them to grow unchecked and passing on increases every year to patients. Over time, this should help make health care more affordable for families.
If a health care organization exceeds its spending growth target without a good reason, OHCA will take increasingly serious enforcement actions, starting with guidance to the company on how to meet the target all the way to financial penalties. Penalty money will go into a fund and then back to California families to help them pay for their health care.
Making Sure Quality Stays High
Spending caps are intended to target things like administrative inefficiencies and monopolies, not quality of care.
To ensure health care organizations are focusing in the right places, OHCA is charged with ensuring:
Patients can still get the care they need.
Care quality stays just as good.
Hospitals and clinics have enough doctors and nurses.
OHCA is taking steps to address unfair pricing by reviewing health care mergers and acquisitions.
Congress returns to DC this week to debate the merits of extending the advanced premium tax credits that enable coverage for 4 million in a climate of high anxiety about U.S. intervention in Venezuela and heightened tension with Russia and China.
For many, these unfolding events are numbing: helplessness, frustration and fear are widespread. As 2026 unfolds for U.S. healthcare, the realities are these:
The healthcare economy will be under pressure to do more with less. The health economy is increasingly controlled by private investors and large publicly traded companies in every sector whose shareholder obligations are primary. Public funding from federal, state and local sources is shrinking as a result of the Big Beautiful Bill and pushback from taxpayers who think the system wasteful and ineffective. The S&P Health Index for 2025 closed the year underperforming the broader market. Private equity investments in healthcare except AI solutions that reduce operating costs at scale are troubled. Thus, in 2026, operating margins in every sector will be stressed, access to private capital will be vital and business as usual obsolete.
Mass populism will magnify attention to the healthcare affordability. Per polls, costs of living are issue one to voters. While prices for gas and groceries have moderated, housing and healthcare prices have escalated unabated. Voters think both essential but the majority think consolidation, corporatization and regulatory protections advantage the biggest players and protect special interests. In housing, it’s simpler for consumers: mortgages, rent and utility costs are straightforward. But healthcare is more complicated: out of pocket costs—premiums, co-pays, deductibles, caregivers, OTC et al—are not easily calculable and price estimator tools, patient support and revenue cycle management policies make it easier for consumers. The net result: a large and growing majority of voters think healthcare is unaffordable and government intervention needed.
The mid-term election November 3, 2026 will be likely be the reset for healthcare’s future in 2028 and beyond. All 435 House Seats, 35 U.S. Senate seats and 39 state/territorial governors will be elected. All will face voters anxious about the future and how they’ll pay their bills. The 2026 results will set the stage for 2028 Presidential campaigns that will feature a wide range of alternatives to the healthcare status quo. Some will be incremental; others labeled radical. But all will promise changes unwelcome to many of its prominent incumbents.
Each sector in healthcare—hospitals, physician services, long-term care, insurers, life science manufacturers, enablers and advisors—is vulnerable. None welcomes unflattering attention and all spend heavily on messaging and advocacy to protect themselves. All recognize the elephant in the room—large employers that have patiently funded the system’s profitability and value protective regulation that limit disruption. And in all, implementation of AI solutions that lower operating costs and streamline performance is THE immediate priority.
The realties of 2026 for healthcare are foreboding: business as usual is not an option.