
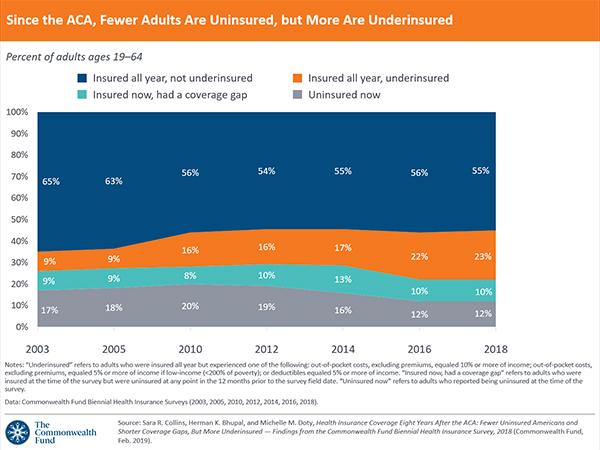
https://www.commonwealthfund.org/chart/2019/aca-fewer-adults-are-uninsured-more-are-underinsured
Hospital Mergers Improve Health? Evidence Shows the Opposite

Many things affect your health. Genetics. Lifestyle. Modern medicine. The environment in which you live and work.
But although we rarely consider it, the degree of competition among health care organizations does so as well.
Markets for both hospitals and physicians have become more concentrated in recent years. Although higher prices are the consequences most often discussed, such consolidation can also result in worse health care. Studies show that rates of mortality and of major health setbacks grow when competition falls.
This runs counter to claims some in the health care industry have made in favor of mergers. By harnessing economies of scale and scope, they’ve argued, larger organizations can offer better care at lower costs.
In one recent example, two Texas health systems — Baylor Scott & White, and Memorial Hermann Health System — sought to merge, forming a 68-hospital system. The systems have since abandoned the plan, but not before Jim Hinton, Baylor Scott & White’s chief executive, told The Wall Street Journal that “the end, the more important end, is to improve care.”
Yet Martin Gaynor, a Carnegie Mellon University economist who been an author of several reviews exploring the consequences of hospital consolidation, said that “evidence from three decades of hospital mergers does not support the claim that consolidation improves quality.” This is especially true when government constrains prices, as is the case for Medicare in the United States and Britain’s National Health Service.
“When prices are set by the government, hospitals don’t compete on price; they compete on quality,” Mr. Gaynor said. But this doesn’t happen in markets that are highly consolidated.
In 2006, the National Health Service introduced a policy that increased competition among hospitals. When recommending hospital care, it required general practitioners to provide patients with five options, as well as quality data for each. Because hospital payments are fixed by the government — whichever hospital a patient chooses gets the payment for care provided to that patient — hospitals ended up competing on quality.
Mr. Gaynor was an author of a study showing that consequences of this policy included shorter hospital stays and lower mortality. According to the study, for every decrease of 10 percentage points in hospital market concentration, 30-day mortality for heart attacks fell nearly 3 percent.
Another study found that hospital competition in the N.H.S. decreased heart attack mortality, and several studies of Medicare also found that hospital competition results in lower rates of mortality from heart attacks and pneumonia.
Another piece of evidence in the competition-quality connection comes from other types of health care providers, including doctors. Recently, investigators from the Federal Trade Commission examined what happens when cardiologists team up into larger groups. The study, published in Health Services Research, focused on the health care outcomes of about two million Medicare beneficiaries who had been treated for hypertension, for a cardiac ailment or for a heart attack from 2005 to 2012.
The study found that when cardiology markets are more concentrated, these kinds of patients are more likely to have heart attacks, visit the emergency department, be readmitted to the hospital or die. These effects of market concentration are large.
To illustrate, consider a cardiology market with five practices in which one becomes more dominant — going from just below a 40 percent market share to a 60 percent market share (with the rest of the market split equally across the other four practices). The study found that the chance of having a heart attack would go up 5 to 7 percent as the largest cardiology practice became more dominant. The chance of visiting the emergency department, being readmitted to the hospital or dying would go up similarly.
The study also found that greater market concentration led to higher spending. And a different study of family doctors in England found that quality and patient satisfaction increased with competition.
For many goods and services, Americans are comfortable with the idea that competition leads to lower prices and better quality. But we often think of health care as different — that it somehow shouldn’t be “market based.”
What the research shows, though, is that there are lots of ways markets can function, with more or less government involvement. Even when the government is highly involved, as is the case with the British National Health Service or American Medicare, competition is a valuable tool that can drive health care toward greater value.

Hospitals and practices have traditionally relied on public and private payers to cover the bulk of patient charges and costs for their services. Everything from their revenue cycle technologies to billing workflows has been tailored to create cleaner claims, reduce denials, and collect payer reimbursement.
But in an environment of record spending and changing attitudes towards purchasing and payment, payers are starting to shift more financial responsibility to their consumers. Nearly 21 million Americans had a high-deductible health plan or health savings account in 2017, and AHIP experts anticipate enrollment in high-deductible plans to continue climbing.
Increases in patient out-of-pocket spending are driving individuals to become more discerning healthcare consumers who demand more value for the medical services they receive. Plans and policymakers argue that the rise in healthcare consumerism will ultimately result in lower cost, higher quality care.
In the meantime, however, high-deductible health plans and other increases in out-of-pocket spending are presenting challenges to providers who are not used to this new player: the patient as a payer.
Three-quarters of providers report that they are seeing a noticeable upward trend in what patients must pay out of pocket. At hospitals, total revenue attributable to patient balances after insurance rose 88 percent from 2012 to 2017.
While payers have been steadily shifting the financial responsibility to consumers, providers have yet to adapt their workflows and systems to collect revenue from this new source while delivering a satisfactory experience to consumers.
For example, nearly all 900 healthcare financial executives recently surveyed by HIMSS Analytics said their organizations still use paper-based billing and collection strategies – despite the fact that the same survey revealed more than half of patients prefer electronic billing methods.
Patients in the survey even said they were more likely to pay their medical bills if they had the option to do so online.
In light of these statistics, providers are facing the difficult task of transforming their manual patient collection processes to address this changing, consumer-focused trend.
“What we’ve seen historically has been that the revenue cycle has been not as well funded or not as strategically prioritized for healthcare delivery networks. A lot of the decision making has been either reactive or more short-term oriented,” Joe Polaris, Senior Vice President of Product and Technology at the health IT company R1 RCM, recently told RevCycleIntelligence.com.
“But we’re starting to see more of a long-term strategic vision coming together for their revenue cycles,” he added. “Organizations understand they need to make transformative change in light of some of the challenges that are only growing in the market, especially the need to be consumer-friendly.”
Revenue cycle technologies that cater to the patient financial experience are part of that transformative change, added Matt Hawkins, the CEO of Waystar, the newly combined revenue cycle management company formed by ZirMed and Navicure.
“Innovators are beginning, more so than ever, to treat the patient as a consumer,” he said. “A lot of health systems are demanding or embracing services or technologies that get them closer to patients from the earliest interaction point.”
The demand for technologies that cater to the patient financial experience is on the rise. And providers could face significant financial losses and patient retention problems if they fail to adapt to healthcare consumerism.
Becoming a patient-centered entity that can collect what it’s owed without alienating its consumers is a significant challenge, experts agree. But embracing a handful of high-impact strategies could help to ensure that both patients and their providers complete the payment process feeling satisfied.
“Consumerism” may be a popular buzzword in the healthcare industry, but providers still have a long way to go before their patients can accurately compare their clinical journeys to their retail experiences.
For one thing, patients often agree to services or procedures with no clear idea of what they will ultimately cost.
Providers rarely offer prices or price estimates to patients prior to service delivery. In fact, the percentage of hospitals that are not able to give consumers price estimates actually increased from 14 percent in 2012 to 44 percent in 2018, a recent JAMA Internal Medicine study revealed.
With patients expecting the ability to plan their expenses, providers are looking to implement new revenue cycle technologies that can deliver accurate cost estimates and boost overall healthcare price transparency.
“How do we give patients shoppable experiences, so they can find out the cost of an MRI?” asked Christy Martin, Senior Vice President of Product Management at Optum360. “In their local care market, where is the best place to go in terms of both quality and cost? Then, if they go to a certain location, what are they expected to pay based on their insurance coverage? What would the out-of-pocket costs be at this point in the year?”
Informing consumers of their patient financial responsibility before the point-of-service is critical for providers seeking to improve the patient financial experience.
“In the immediate future, one of the things that we can unlock using technology is an understanding upfront about what the payment responsibility will be, and have that help inform all of the things that happen subsequent to presenting that to the patient,” Hawkins said.
Providing price estimates up front helped one health system in Oklahoma increase point-of-service collections by $17 million in seven years.
The Consumer Priceline tool at INTEGRIS Health is a database of charges for most procedures and services. The health system also promises to deliver written price quotes to consumers within two days if the service is not already included in the database.
INTEGRIS may be seeing significant patient collection improvements using price estimates, but providers should be aware that databases like the Consumer Priceline tool require a wealth of historical financial data.
“In the immediate future, one of the things that we can unlock using technology is an understanding upfront about what the payment responsibility will be.”
Merely posting chargemaster prices for common services and procedures is not necessarily helpful for patients. Giving consumers information about their patient financial responsibility and out-of-pocket costs is supposed to prevent sticker shock. Yet chargemaster prices are primarily used to start negotiations with payers, and the numbers can seem exorbitant to consumers.
“Chargemaster prices serve only as a starting point; adjustments to these prices are routinely made for contractual discounts that are negotiated with or set by third-party payers. Few patients actually pay the chargemaster price,” the Healthcare Financial Management Association (HMFA) explained to policymakers in May 2018.
Despite reservations about chargemaster prices, CMS recently required hospitals to publish a list of their standard charges online. And providers are scrambling to understand how to present the information in a meaningful way to consumers.
About 92 percent of providers in a recent poll said they were concerned about the new hospital price transparency requirement, and the majority also expressed concerns about how the public would perceive their standard charges.
Now more than ever, revenue cycle technologies that aggregate and analyze information on what patients actually pay will be critical for health systems.
Healthcare is nothing like going grocery shopping. Not only do consumers not have access to prices, but the funding mechanism for medical services is also vastly different from a traditional retail experience.
Unlike what happens during a retail transaction, healthcare consumers rarely pay providers directly for services or procedures rendered. Instead, healthcare consumers use insurance plans, health savings accounts, and a wide range of other funding mechanisms to eventually pay providers after a service is delivered. They may also receive several bills and benefit documents from providers and insurers before receiving the final bill listing their financial responsibility.
As patients become more responsible for their healthcare spend, the onus is on providers to simplify the patient financial experience if they want to boost collections and save their bottom line.
Delivering a navigable and consistent financial experience is key to making the most of the newly consumer-driven environment, Polaris advised providers.
“The patient wants to have a clear and transparent journey through the healthcare system, and that’s much more challenging when they have to navigate different departments on different systems, asking for the same data over and over again, never coordinating, and never communicating a holistic end-to-end experience,” he said.
Integrated and seamless revenue cycle technologies aim to deliver a consistent patient financial experience by simplifying medical bills and bringing all providers in a practice, hospital, or health system under the same billing brand.
For example, a multi-specialty physician group in central Texas boosted patient collections by 24 percent and reduced the amount of patient cash sitting in A/R from 14 to two percent in one year by unifying the patient financial experience across their organization.
“Even though we were one clinic with 60 providers, our collection process treated every healthcare encounter separately,” explained Abilene Diagnostic Clinics CFO Andrew Kouba, CPA. “Patients were receiving bills for each physician they saw, which allowed them to pick and choose which bills to pay. When you get four statements and you think you got one experience, you’re confused as a patient.”
Consolidating all of Abilene’s providers under one billing system helped the group to deliver a consistent patient financial experience, which in turn simplified the payment process for consumers.
Revenue cycle departments are finding that end-to-end systems or interoperable bolt-on solutions are worth the investment. The integrated technologies allow healthcare organizations to guide the patient through the financial experience.
But to truly advance the patient financial experience, revenue cycle technology experts agreed that clinical and financial data integration is also vital.
“Being able to leverage the clinical and billing data to provide a better patient experience all the way around is a key capability,” Martin of Optum360 stated.
“While hospitals are certainly focused on providing high-quality care, there’s also this focus on how they can improve the overall patient financial experience to reduce the confusion, complexity, and lack of understanding around patient responsibility. Health systems are looking to provide ease of doing business to address patient responsibility and reduce patient bad debt.”
Revenue cycle technologies that can leverage both clinical and financial data are crucial to transforming the patient experience into a consumer-friendly encounter. Understanding the whole patient can help providers offer a consistent experience from the front office to the billing department.
Price transparency tools and integrated revenue cycle technologies lay the groundwork for a consistent, intuitive patient financial experience. But revenue cycle technology vendors are also observing an increased interest in self-service portals and kiosks for the ultimate retail-like experience.
The disjointed, manual processes involved in the patient financial experience have not been convenient for consumers. Patients often have to interact with a call center or sit down with a staff member to complete basic tasks like scheduling, filling out insurance forms, or paying a medical bill, Polaris explained. In other industries, these tasks have already been replaced by mobile apps or automated systems.
“With digital self-service, we automate tasks like they do in the airline industry,” he said. “We let the patient book an appointment right on their mobile phone, get all the paperwork, fill out the forms they need, and check in at a kiosk.”
“Automation takes repetitive tasks that are frankly not patient- or consumer-friendly out of the process and makes the whole healthcare experience much more satisfying,” he stressed.
Self-service portals and kiosks have the potential to truly transform the patient financial experience into a more convenient, navigable journey. But healthcare organizations would need to invest in large amounts of revenue cycle automation to achieve this goal, Polaris acknowledged.
“Automation takes a lot of forms,” he explained. “There’s always been robotics, user emulation, and basic automation to complete individual tasks. But very few organizations have driven automation of entire processes, and that’s where we’re seeing more investment in transformative automation.”
Healthcare consumers have already voiced their support for more self-service options and more automation. A recent survey of over 500 individuals showed that in addition to offering more payment options and sending simpler bills, expanding access to self-service tools was a top suggestion for improving the patient financial experience.
“Automation takes repetitive tasks that are frankly not patient- or consumer-friendly out of the process and makes the whole healthcare experience much more satisfying.”
Providers are also expressing interest in implementing the relatively new technology in the revenue cycle space. Kouba from Abilene Diagnostic Clinic in Texas said he wanted to create a type of Disney FastPass for the patient financial experience.
“We want to simplify the process from pre-registration through bill collection and try to automate that similar to Disney’s FastPass,” Kouba stated. “Disney is one of the best experiences of all time and when you go there, they want you to interact with the people, all their products, and just enjoy yourselves. The last thing Disney wants you to think of is the terrible lines.”
“If we can remove the pain points and strive to ease that front piece, the patient will be focused on a friendly conversation when they walk in the door with the person that can answer questions, rather than being pestered to pull out their wallet.”
However, Kouba is not convinced that full automation will take over the healthcare industry any time soon.
As much as adopting retail-style approaches can improve the patient financial journey, providers must still ensure their technologies and processes work for them, too.
For example, Kouba decided that self-service technology that automates scheduling is not ideal for Abilene.
“In our group, most of our physicians like to follow their patients to the hospital, so the difficult piece with self-scheduling, especially from the provider’s side, is their schedules depend on what their rounds look like for the day. It’s very difficult to get them to commit to blocks of time,” he continued.
Self-service and automated tools may still be maturing in the revenue cycle technology space. But providers still have the option to improve the patient financial experience through systems that estimate patient financial responsibility and unify the billing experience.
And providers should be looking to the revenue cycle technology market for help. The rise of patient financial responsibility has been steady. Deductibles and out-of-pocket costs have been growing, particularly since healthcare spending growth rates rapidly accelerate.
Implementing the right tools for their patients and their providers will be key to empowering patients to choose the highest value care while ensuring providers get paid for it.
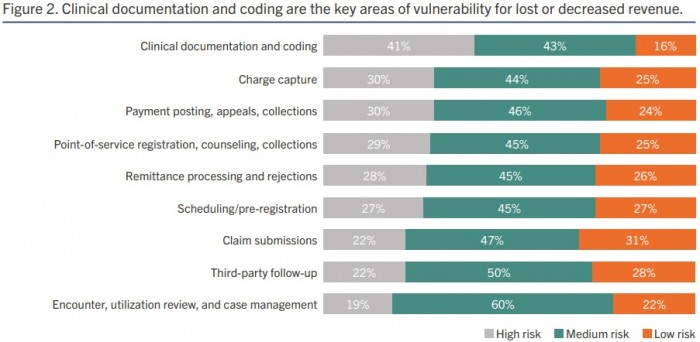
Hospital leaders are concerned that their organization’s clinical documentation and coding processes are vulnerable to errors that could result in lost or decreased revenue, according to a recent survey.
Consulting firm and technology vendor BESLER recently partnered with HIMSS Media to identify the greatest industry challenges and potential opportunities for revenue cycle improvement. They surveyed over 100 leaders within finance, revenue cycle, reimbursement, and health information management (HIM) departments at hospitals and acute-care facilities in October 2018.
The recently released survey results showed that 84 percent of respondents believe clinical documentation and coding are high or medium revenue cycle risk.
Hospital finance leaders were the most adamant that clinical documentation and coding presented significant revenue cycle challenges. Almost one-half of finance leaders chose clinical documentation and coding as their greatest revenue cycle vulnerability.
Although, the area was considered high or medium risk by over one-third of revenue cycle, reimbursement, and HIM leaders as well.
Clinical documentation and coding are creating revenue cycle vulnerabilities because solutions are not optimized for the diagnosis-related group (DRG) payment system, respondents shared. Only about one-third of hospital leaders said DRG optimization is a solved problem. In other words, the majority of hospital leaders (68 percent) do not think their solutions are equipped to manage DRG coding.
The DRG payment system has been around for over three decades. And major payers, including Medicare, use the payment system to determine lump-sum payments for hospitals that treat specific diagnoses.
While the payment system is not new, it is constantly evolving. Payers are attempting to get more specific about diagnoses to ensure hospitals are paid accurately for treating patients with certain conditions. The introduction of ICD-10 in 2015 is a prime example of how the industry has changed the DRG payment system.
But DRG changes are not ideal for providers. Hospitals find it difficult to follow and comply with constant DRG changes, and as a result, DRG coding accuracy has decreased. The report stated that the national benchmark for DRG assignment fell from 95 percent under ICD-9 to 72 percent in 2018.
Revenue cycle solutions, however, are optimized for inpatient coding and audits. Approximately 72 percent of respondents felt their technology is optimized for inpatient coding.
The survey also uncovered that respondents thought the accuracy of inpatient coding at their organizations was about the same as the industry benchmark.
Additionally, the majority of respondents (72 percent) agreed that their revenue cycle solutions are optimized for outpatient coding.
Opportunities to improve revenue cycle management technology remain. And poor coding integrity could result in the top two challenges hospitals face: claim denials (49 percent of respondents) and inaccurate reimbursements (47 percent of respondents).
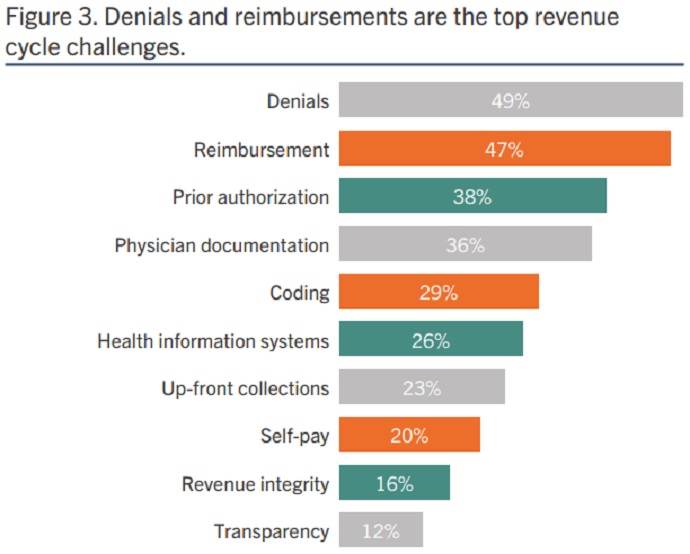
Source: BESLER and HIMSS Media
However, hospitals and health systems face significant obstacles with improving their mid-revenue cycle processes, including DRG coding and documentation. Chief among the challenges is a lack of budget. Nearly one-half of hospital leaders (49 percent) said budget constraints prevented their organization from improving DRG coding and documentation.
Nearly the same percentage of leaders also felt return on investment (ROI) was an obstacle. Forty-eight percent of respondents said difficulty proving ROI from investment stopped their organization from executing DRG optimization efforts.
Other obstacles to improving the mid-revenue cycle included:
- Competing projects (45 percent)
- Lack of staff/headcount to manage improvement efforts (38 percent)
- Lack of familiarly with solutions to address challenges (34 percent)
- Existing solutions already widely entrenched or accepted (32 percent)
- Overcoming internal perceptions that there is no need for improvement (30 percent)
Respondents identified a variety of challenges, but the survey also found a potential solution for hospitals and acute-care facilities. The survey showed that nearly half of respondents (47 percent) have created a revenue integrity program, which ensures organizations are being fully compliant with coding and billing practices while also achieving operational efficiency and legitimate reimbursement.
That means about 53 percent of hospitals still haven’t implemented a revenue integrity program.
About three-quarters of hospitals with revenue integrity programs reported improvements in net collections, increases in gross revenue capture, and/or reduction in compliance risk.






Intermountain Healthcare’s chief information security officer Karl West kicked off the HIMSS19 Revenue Cycle Solutions Summit with a strong message for his captive audience. If you’re a revenue cycle leader, you need to understand a fundamental reality: There’s a whole host of data available for hackers in your rev cycle. Not only is there payment information, there is also member information and all of your PHI. All of those are sources of cyber risk.
For example, patient portal credentials are highly valuable for hackers at around $1,500 or more according to one study, West said.
As such, there needs to be a strong partnership between your cyber organization/operation and your revenue cycle. You also need to understand what are the threats and sources of loss. First, there’s phishing. It’s common and proven to be effective. At Intermountain, they phish their employees four times a year to test their proclivity to fall victim. Even though some find the measure frustrating, it’s essential to flushing out vulnerability.
Malware is also a significant security threat. To thwart such threats, it’s important to keep your systems patched. In your system, you need to have someone watching for vulnerability and patching.
“That’s the basic blocking and tackling,” West said.
Another source of loss is the misconfiguration of public-facing systems, which occurs when at build time, the proper protections are not built in.
And then there are nation-state actors, which are harder to protect against because smaller organizations do not have the resources to spend a lot on cybersecurity. Intermountain has a 24/7 security station/operation with eyes on such threats.
Finally, there are theft or loss/inadvertent accidents that involve employee error or bad action.
“If you aren’t, those are things you should be considering,” West said.
As consumerism continues to drive healthcare, the revenue cycle must move with that trend, and in a consumer-driven revenue cycle organization, fraud, breach, patient card information, PHI, personally identifiable information and the cloud are both assets and areas of risk.
As such, vulnerability management in the revenue cycle should be a big part of your operation and claims processing.
“When a caregiver gives care, they must be current on flu shots and vaccines,” West said. “It’s not an option. It’s a condition of employment. It means that the caregiver is protected to the best ability that we can. In the cyber world, it’s the same. Your networks, laptops and servers, how are you protecting them?”
While updates are annoying, vulnerabilities do need to be patched. Most healthcare organizations patch on an annual basis. At Intermountain, however, it is on a weekly or monthly basis. It’s a different mindset, West said. That is because not only did healthcare cyber attacks increase 320 percent between 2015 and 2016, but the attacks are also growing in sophistication. They don’t just slow systems down – they can cripple them for days, weeks or even months.
So, it is important to know that your patches are in place and your action plans are in place, he said. Have arrangements with vendors and partners. And for the many who have migrated to the cloud to streamline and cut costs, develop a strategy that isn’t just focused on one cloud but the whole cloud and know the controls required to protect you. West asked, does your cloud partner have a vulnerability and what are their safety practices?
“Have an inventory of your partnerships and manage them. Establish governance. As the primary organization, you are the one accountable to your patients,” he said.
Have an inventory of your data – where it is stored, where will it move to, and how it will move safely and securely. This should be a key performance indicator (KPI). Classify your data as public, restricted, private, classified or confidential, such that it is properly protected, and have data loss protection tools.
“When you wonder how did one system get taken down and not another, it’s your patching and practices,” West said.
